
Abstract
This report presents 2 unusual cases along with a review of the current literature. Further, it aims to propose an algorithm for the initial surgical management of migrating ingested foreign bodies, focusing on the use of fluoroscopy, rigid laryngopharyngoscopy, and an external surgical approach. A 42-year-old man presented with progressive odynophagia after swallowing a fish bone 20 days previously, and a 60-year-old woman presented with a painful enlarging mass over the left lower neck for 1 month. The first case involved a horizontally oriented pharyngeal fish bone with a portion in the neck, which was removed under fluoroscopic guidance and rigid laryngopharyngoscopy in succession. In the second case, there was an extraluminal fish bone that had migrated into the sternocleidomastoid muscle, which was retrieved through cervical incision. All foreign bodies were removed without complications. To the best of our knowledge, this is the second report of fluoroscopy-guided ingested foreign body retrieval and the first one with a proposed algorithm for the management of migrating ingested foreign body in the neck. The location and orientation of migrating ingested foreign bodies as well as their relation to structures in the neck are important factors in determining the surgical approach.
Introduction
A small percentage of ingested foreign bodies penetrate the pharyngeal mucosa and migrate into the neck, which requires surgical intervention.1-3 Muscle contraction, horizontal orientation, patient manipulation, and tissue reaction may contribute to the migration.1-9 These migrating foreign bodies are rare; however, they may cause severe complications such as penetration of vessels, deep neck infection, esophageal perforation, retropharyngeal abscess, and thyroid abscess.2,3,5,7,9-15 Immediate diagnosis, visualization, and removal of migrating foreign bodies on endoscopy under local anesthesia can be very difficult.3-5,10,11,14 In addition, some cases presented with subtle or bizarre manifestations such as cervical mass or cutaneous fistula without oropharyngeal complaints.5-8,10,16,17
There are several techniques to retrieve a migrating foreign body in the neck, including the endoscopic and percutaneous approaches. The aim of our report is to describe these procedures with 2 unusual cases, review literature, and propose an algorithm to determine the initial surgical management of migrating ingested foreign bodies.
Case Report
Case 1
A 42-year-old man presented with progressive odynophagia after swallowing a fish bone 20 days previously. Flexible pharyngolaryngoscopy and upper gastrointestinal (UGI) endoscopy failed to locate the fish bone. Computed tomography (CT) revealed a 4-cm fish bone in the hypopharynx, with both ends penetrating the pharyngeal mucosa. The right end was in the retropharyngeal space (Figure 1A and B). A percutaneous extraction route through the left thyrohyoid membrane was planned. Under general anesthesia, we performed a puncture of the left neck and forwarded a small hemostatic forceps under fluoroscopy guidance (Figure 1C and D). However, the fish bone fractured during extraction (Figure 1E). The CT scan was repeated. A small piece of broken fish bone was retained in the left thyrohyoid membrane (Figure 1F). Then, a direct rigid pharyngolaryngoscope was inserted. We removed the granulation tissue with a dioxide (CO2) laser. The rest of the bone was completely extracted (Figure 1G). The overall extracted fish bone was 4 cm (Figure 1H). Video esophagography showed no pharyngocutaneous fistula, and the granulation tissue disappeared 2 weeks postoperatively.
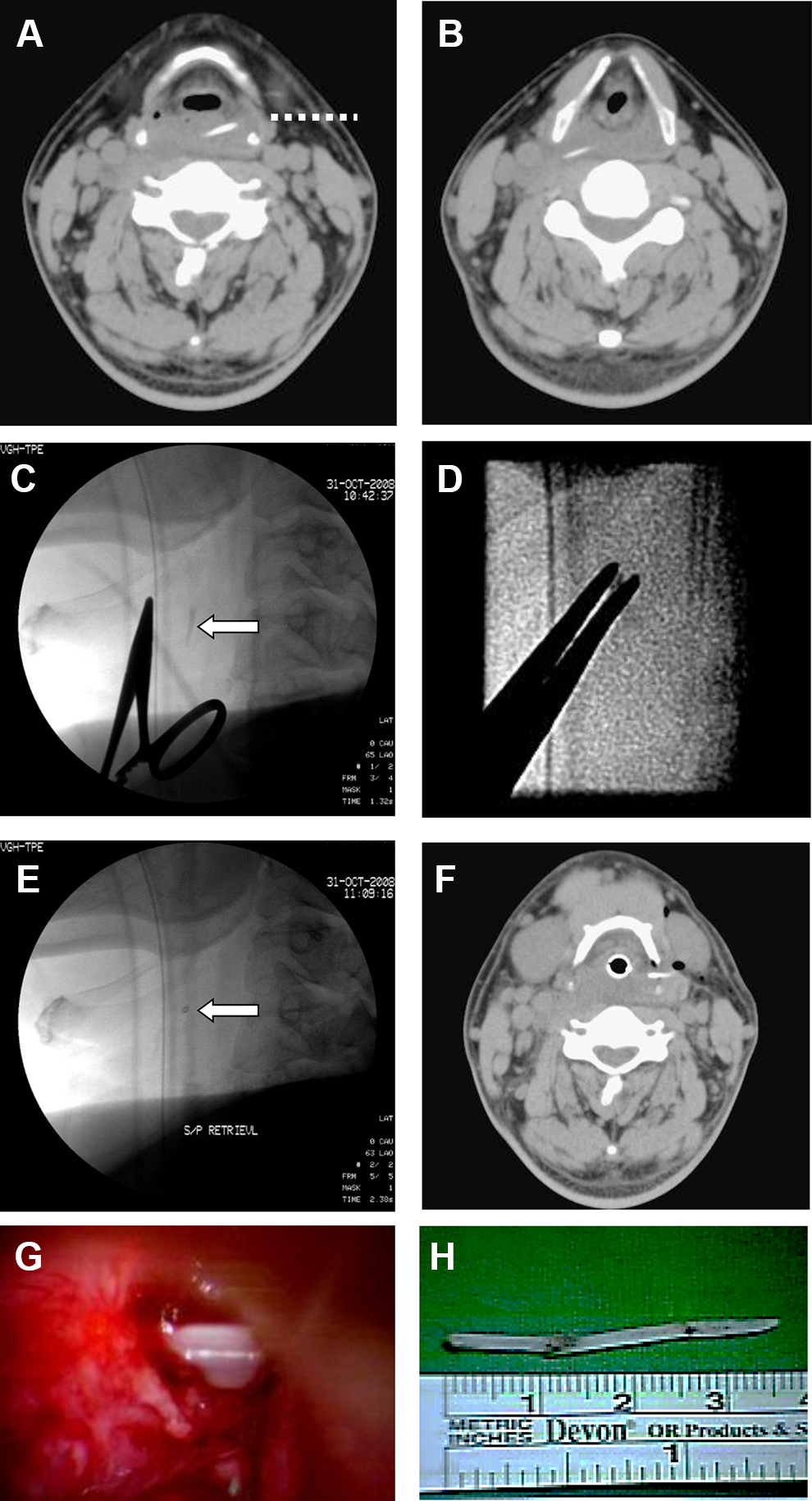
Case 1. A and B, The computed tomography (CT) scan shows a linear, horizontally oriented fish bone in the hypopharynx, covered with granulation. Both ends pierce through the buccopharyngeal mucosa. The right end is in the retropharyngeal space. A percutaneous extraction route through the left thyrohyoid membrane is planned (dotted line). C, We located the fish bone (arrow) with a pair of hemostatic forceps under fluoroscopy after percutaneous puncture of the left neck. D, The fish bone is removed. E and F, The fish bone (arrow) fractured during the first procedure. The residual part of the fish bone is retained in the left thyrohyoid membrane. G, The rest of the bone is completely extracted under direct rigid laryngoscope. The retained granulation is removed with CO2 laser. H, The fish bone is approximately 4 cm in length, with sharp tips on both ends.
Case 2
A 60-year-old woman presented with a painful enlarging mass over the left lower neck for 1 month. A 2.5-cm hypoechoic mass with linear calcification over the left lower neck was found on ultrasonography (Figure 2A and B). No lesion was seen on flexible pharyngolaryngoscopy. The CT scan showed a rod-shaped opacity lying vertically in the left sternocleidomastoid (SCM) muscle (Figure 2C and D). The superior end was in close proximity to the left thyroid gland and left internal jugular vein. The patient could not recall any history of foreign body ingestion. A 2-cm incision was made over the left lower neck and a fish bone of 2 cm was found deep to the SCM muscle. We en bloc removed the fish bone along with the adjacent granulations and fibrotic tissues (Figure 2E and F) without any damage to the thyroid gland and internal jugular vein.
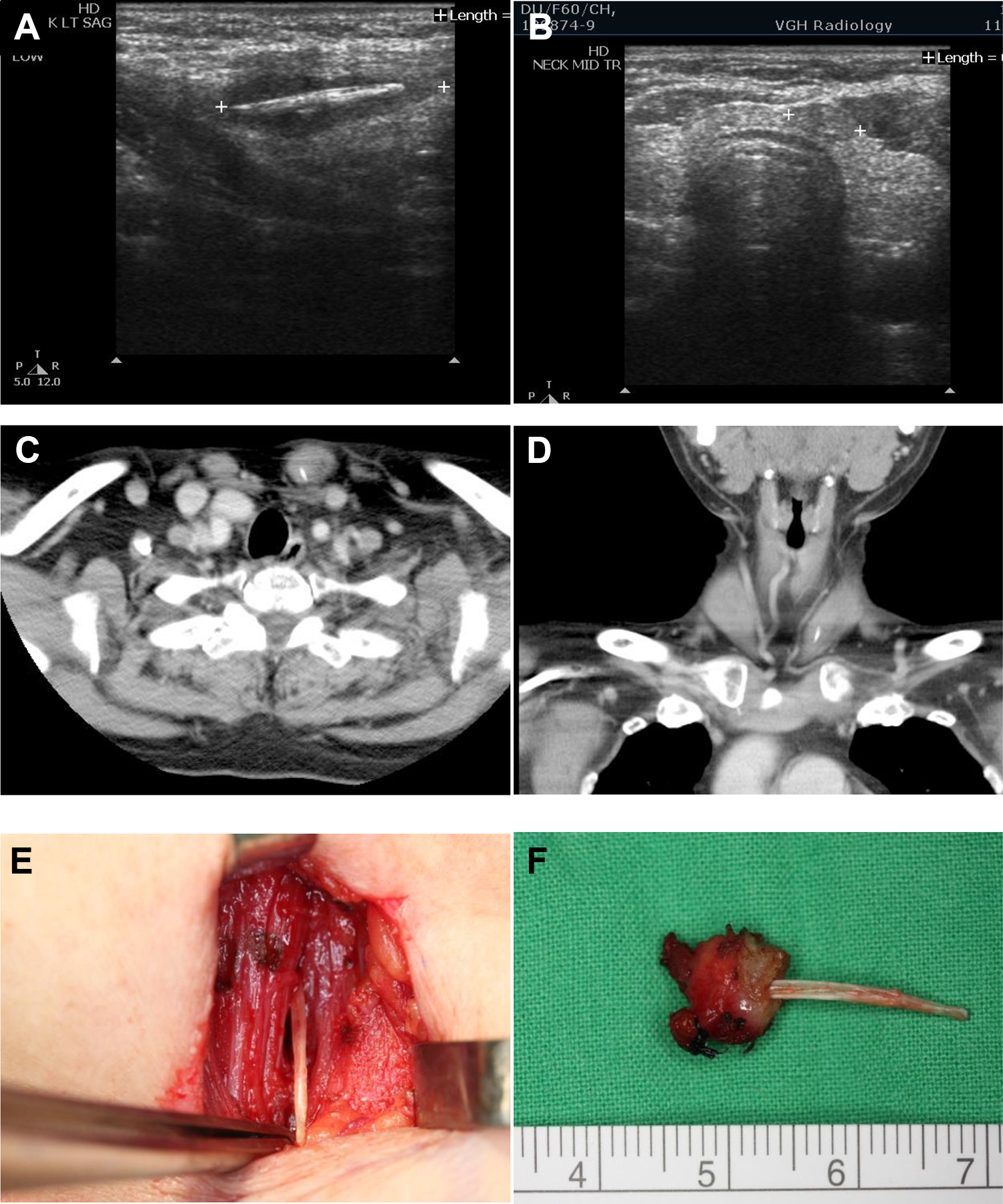
Case 2. A, Sagittal view of ultrasonography reveals a 2.5 cm hypoechoic mass with linear calcification over the left lower neck. B, Axial view of ultrasonography shows the relationship between the mass and thyroid gland. C and D, A rod-shaped opacity vertically lying in the posterior and inferior portions of the left sternocleidomastoid muscle is identified on the computed tomography (CT) scan. The superior end is close to the left thyroid gland and left internal jugular vein. E and F, A 2-cm incision is made over the left lower neck. A 2-cm fish bone deep into the sternocleidomastoid muscle is noticed, along with surrounding granulation over the superior end. The fish bone and inflammatory tissues are carefully removed from the sternocleidomastoid muscle, clavicle, and vasculature. Some pus is drained from the wound.
Discussion
Our surgical managements are illustrated in the algorithm (Figure 3). The CT scan is essential to evaluate the status of the foreign body and nearby structures before any surgical attempt.1,3,4,6,8,10,11,13-15,18,19 For foreign bodies with complications or that are close to great vessels and vital organs, an external approach is preferred. Consultation of cardiothoracic and/or cardiovascular surgeons is recommended in cases of mediastinitis and pulmonary and cardiovascular penetration. Transcervical exploration remains the last resort when the endoscopic and fluoroscopic approaches fail. 20
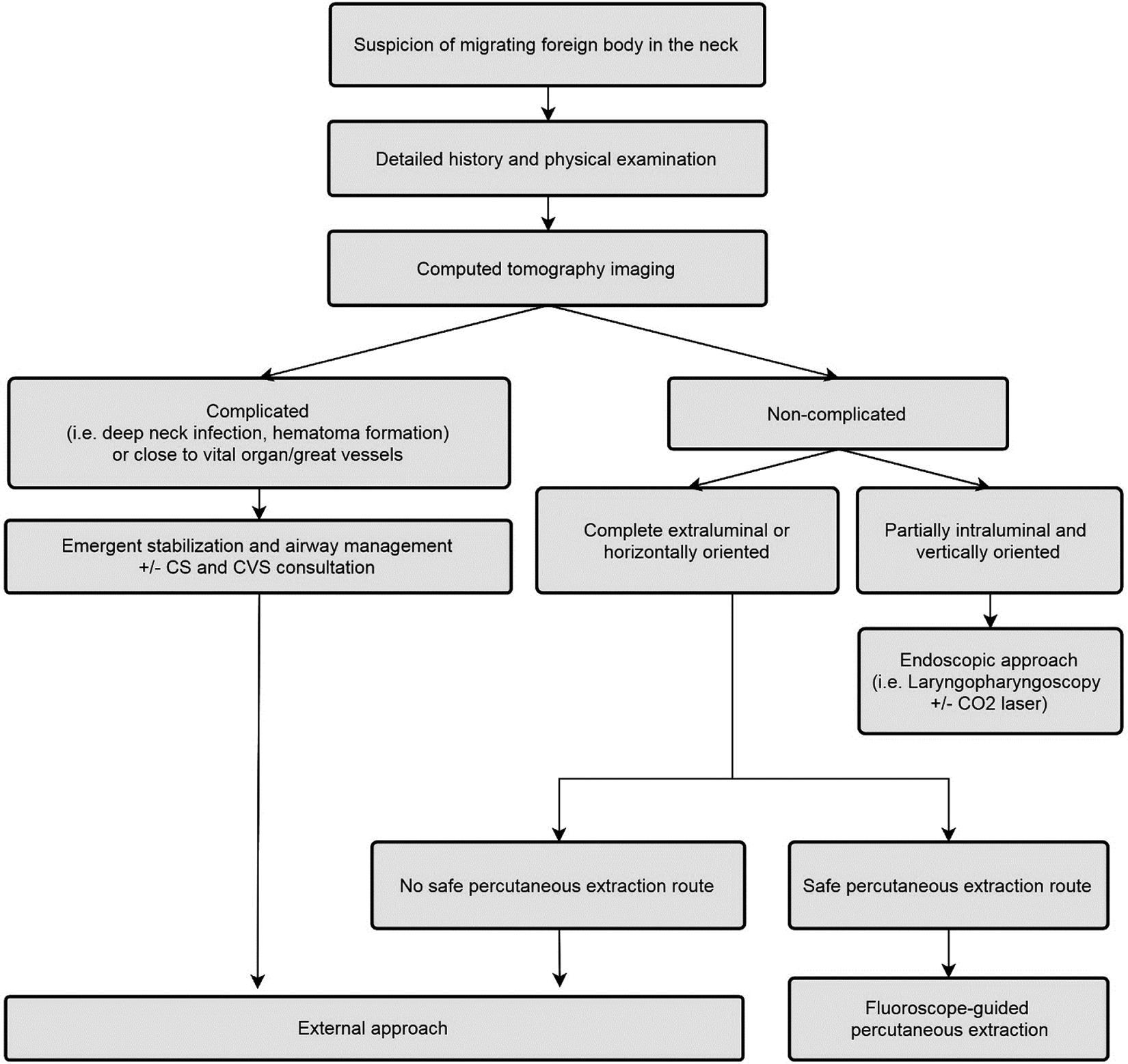
The proposed initial surgical management algorithm for patients with migrating ingested foreign body in the neck. The patient should be reevaluated with computed tomography (CT) scan in case the failure of any procedure or there is a significant change in clinical presentation. All cases should be managed with systemic antibiotics, with or without tube feeding. Cardiothoracic consultation and/or cardiovascular surgeons are recommended in cases with mediastinitis, pulmonary, and cardiovascular penetration.
Fluoroscopy is a minimally invasive, widely available, but relatively underused technique. Till date, only one case report has addressed the use of fluoroscopy in fish bone removal. 4 It provides a real-time and precise intraoperative assessment of the foreign body. However, the target should be radiopaque and the surgeon should be familiar with the neck anatomy so that a safe extraction pathway can be planned in advance. The fluoroscopic approach is especially helpful for horizontally oriented foreign bodies and those with large extraluminal parts, both of which could be very challenging via an endoscopic approach wherein massive mucosal damage is hardly avoidable.
Removal by flexible pharyngolaryngoscopy or UGI endoscopy is possible when the intraluminal portion of a vertically placed foreign body is long enough to be seen under an endoscopy. Rigid pharyngolaryngoscopy or esophagoscopy are preferred for those who could not tolerate removal under local anesthesia. Limited dissection with a CO2 laser is safe and helpful in cases with edematous mucosa and granulation formation that obscure the foreign body.
During the retrieval, multiple techniques may be used in combination.4,12,17,20 In the first case, considering the submucosal location and horizontal orientation of the fish bone, fluoroscopy-guided removal was attempted initially. Retrieval through the left thyrohyoid membrane was planned because it was the shortest percutaneous extraction route without any pivotal structures in between. Due to residual intraluminal fish bone, a rigid pharyngolaryngoscope with a CO2 laser was injected. In such a condition, the CT scan should be repeated, especially when one procedure fails or the clinical presentation changes. 15
In the second case, the foreign body had probably penetrated the mucosa of the cervical esophagus, migrated through the space between the pretracheal fascia and carotid sheath at the level below the thyroid isthmus, and ended up in the left SCM. In a systemic review, 18 cases were identified with the migrating foreign bodies loaded in the thyroid gland, mostly treated with hemithyroidectomy. 5 To avoid damage to the thyroid gland and internal jugular vein, we removed the foreign body with a transcervical exploration. Furthermore, massive fibrosis and granulation formation were expected along the migrating tract, so we precluded the fluoroscopy as an option.
To the best of our knowledge, this is the second report of fluoroscopy-guided ingested foreign body retrieval and the first one with a proposed algorithm for the management of migrating ingested foreign body in the neck. This algorithm should be validated by future studies, and more individualized management should be provided to these clinically diverse patients.
Conclusion
The location and orientation of migrating ingested foreign bodies as well as their relation to structures in the neck are important factors in determining the surgical approach.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.