
Abstract
Person-specific three-dimensional computational modelling plays a vital role in modern-day research of cochlear implants to assist in understanding the neural interface of the cochlea and implanted electrode array. Further improvements are made to these models as more parameters are included. Landmark assessment provides information and is frequently used to register coordinates for model generation as it captures small variations.
Objectives
The objective of this study is to identify and define landmarks to adequately describe the internal auditory canal for inclusion in three-dimensional computational models of the cochlea and its surrounding structures.
Participants
Computer tomography scans of live human cochleae were collected in the retrospective period. Descriptive and comparative statistics were used to describe the data obtained from the scans.
Results
The mean anterior-posterior (AP) diameter at the base of the basal turn, the diameter of the AP at the midpoint of the IAC, and the anterior and posterior length of the internal acoustic canal were measured. 57.14% of the internal acoustic canals observed presented with a cylindrical, 40.48% was funnel-shaped and 2.38 % were bud-shaped. A statistically significant differences were found between the diameters of male and female internal acoustic meatus.
Conclusions
This paper serves as a reference that provides a set of references for the description of the internal acoustic canal for inclusion in three-dimensional computational reconstruction of the cochlea and surrounding structures.
Keywords
Succinct key points
Three-dimensional computational modelling of the cochlea, inclusion of IAC parameters; IAC shapes; Dimensions of the IAC; Deriving landmarks from CT scanning.
Introduction
The use of 3D computational modelling allows for the prediction of current spread through the cochlea, resulting in a better understanding of the functioning of the implanted cochlea. 1 The anatomical description of the cochlea is constantly being developed to incorporate more detail that may improve the accuracy with which the outcomes of cochlear implantation may be predicted. 2 There are few studies in which the morphology of the internal acoustic canal (IAC) is included in the construction of 3D computational models of the cochlea. 2,3 In the present 3D computational models of the cochlea, the nerve has frequently been modelled as a smooth straight volume exiting the cochlea. 1
The rounded and smooth IAC is said to be on average 8.5 mm (5.5–10 mm) in length and about 4 mm in diameter. 3,4 Researchers found that there are variations in the length, width and shape of the IAC.
The IAC can be classified into one of three shapes, that is, funnel-shaped, cylindrical and bud-shaped. 4 The shape of the IAC is usually noted by direct inspection of CT images. In a recent study by Marques et al., the shapes were metrically by taking the following measurements: (1) opening diameter of the IAC, which was measured from the concave part of the posterior lip of the IAC wall to the more medial border of its anterior border, (2) length of the IAC, measured from the midpoint of the IAC to the extremity of the canal in its concave portion, (3) diameter anterior-posterior (AP), measured perpendicular to the straight line drawn from the midpoint of the IAC length uniting the anterior and posterior wall of the IAC and (4) distance from the IAC to the vestibular aqueduct, which is the distance between the most concave wall of the posterior lip of the IAC and the medial border of the vestibular aqueduct. 4 The IAC is said to be funnel-shaped if the opening diameter is larger in relation to the AP diameter, cylindrical if the opening diameter and the AP diameter are relatively similar in size, and lastly bud-shaped if the AP diameter is relatively larger than the opening diameter. The shape classifications (funnel, bud and cylindrical) remains subjective. 5,6 In practice, most IAC are funnel-shaped if one view a slice inferior to the equator of the IAC. While many are bud-shaped if the IAC is viewed directly at an equator slice. Reconstruction of the IAC in the present study was done using mid-modiolar slices thereby avoiding the subjectivity of the shape determination. In clinical practice, the reader is limited to the slices given by the radiology centre. 7 A truly bud-shaped IAC can easily be interpreted as funnel-shaped if your cut happens to be at the bottom of the IAC. Mid-modiolar sectioning of the cochlea and the IAC eliminates this bias. 8
Knowledge about the relationship between IAC and CoN is particularly important when considering CI surgery, as CoN plays a vital role in the success of cochlear implantation. According to the existing literature, there is a positive correlation between the size of the IAC and the size of the CoN. 3,9 Hypoplastic IAC has been found to be associated with CoN aplasia, while CoN hypoplasia has been described in studies of human temporal bones in association with inner ear malformation and IAC stenosis. 9,10 Congenital sensorineural hearing loss has been shown to be well correlated with IAC stenosis. 3,11,12 The stenosis of the IAC has been reported to be associated with the stenosis of the bony cochlear nerve canal. The IAC and the bony cochlear nerve canal are said to be complementary structures and are commonly associated with cochlear nerve deficiency. 9 The most common cause of sensorineural hearing loss is said to be a lack of development of CNVIII. 11 Tahir et al. reported that the presence of IAC stenosis on CT images is indicative of CoN aplasia and poor performance with CI surgeries and recommended that the presence of IAC stenosis contraindicate cochlear implantation. 9 This relationship between the CoN and the IAC supports the concept of using the IAC as a determinate of the path of the CoN since the size, shape and curvature of the IAC inform the shape and path of the CoN.
Analysis of the IAC to determine the shape of the CoN is of significance for 3D computational reconstruction of the auditory system. The location of the CoN fibres within the IAC may affect the way in which the current spread is predicted. 13 -15
No landmark set describing the shape of the IAC has yet been established. CT images are well suited to obtain the morphology of the IAC in live CI recipients. 1 Therefore, it was a precedent for this study to establish a set of landmarks to capture anatomical knowledge of the IAC using CT images. This knowledge will be applied to refine the description of the morphology of CoN exiting the cochlea in user-specific 3D computational models and may benefit CI researchers and clinicians in understanding and predicting the outcomes of implantation.
Objectives
The objectives of the study were to identify and define landmarks to be used to define the parameters of the IAC for inclusion in 3D computational models.
Materials and methods
Setting
Retrospectively collected CT scans of 42 live cochleae were analysed (21 males and 21 females).
Design
Participants
All scans were taken at the same facility using a Siemens Sensation 64 CT scanner (Siemens, Munich, Germany). The scanning parameters for the live cochleae were acquisition 12 × 0.6 mm, rotation time 1s, pitch 0.8 and 120 kV tube voltage. The reconstruction parameters were increment of 0.3 mm reconstruction, 90 mm reconstruction FOV and U90u kernel.
Ethical considerations
This study was approved by the Ethics Committee of the Faculty of Health Science Research of the University of Pretoria, which granted a waiver of informed consent since this retrospective study was conducted with anonymised data (Ethics number 477/2021).
Landmarks
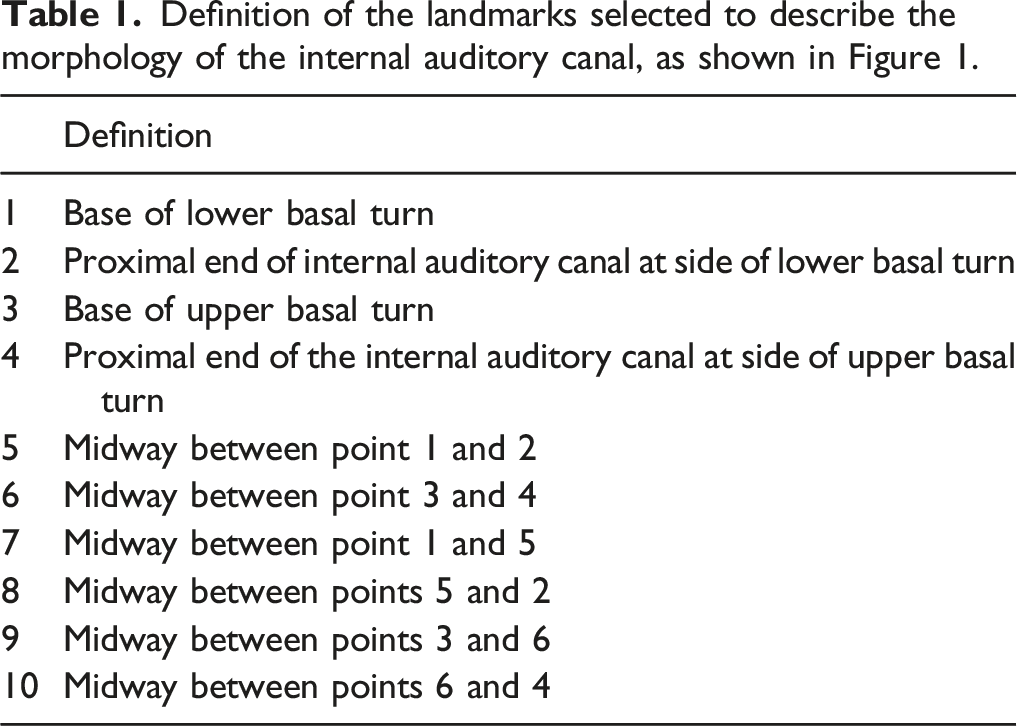
Landmarks were selected and defined to register coordinates for 3D computational modelling and the description of the dimensions (i.e. length and width) and the shape (i.e. curvature) of the IAC. The landmarks were numbered from landmark 1–10 starting at the cochlear inlet as illustrated in Figure 1 and defined in Table 1. Landmarks 1 and 2, 3 and 4 give the lengths of the IAC walls, while landmarks 5 and 6 give the width at the midpoint of the IAC. Landmarks 7–10 were not used to calculate any of the dimensions however they are important coordinates as they inform the curvature of the IAC. The landmarks were selected as they would inform the shape and the curvature of the IAC and allow for dimensions to be taken. Identified landmarks of the internal auditory canal that are defined in Table 1. These landmarks were selected to record coordinates for model used to measure the diameters and lengths of the internal auditory canal in order to classify the shape of the internal auditory canal. Definition of the landmarks selected to describe the morphology of the internal auditory canal, as shown in Figure 1.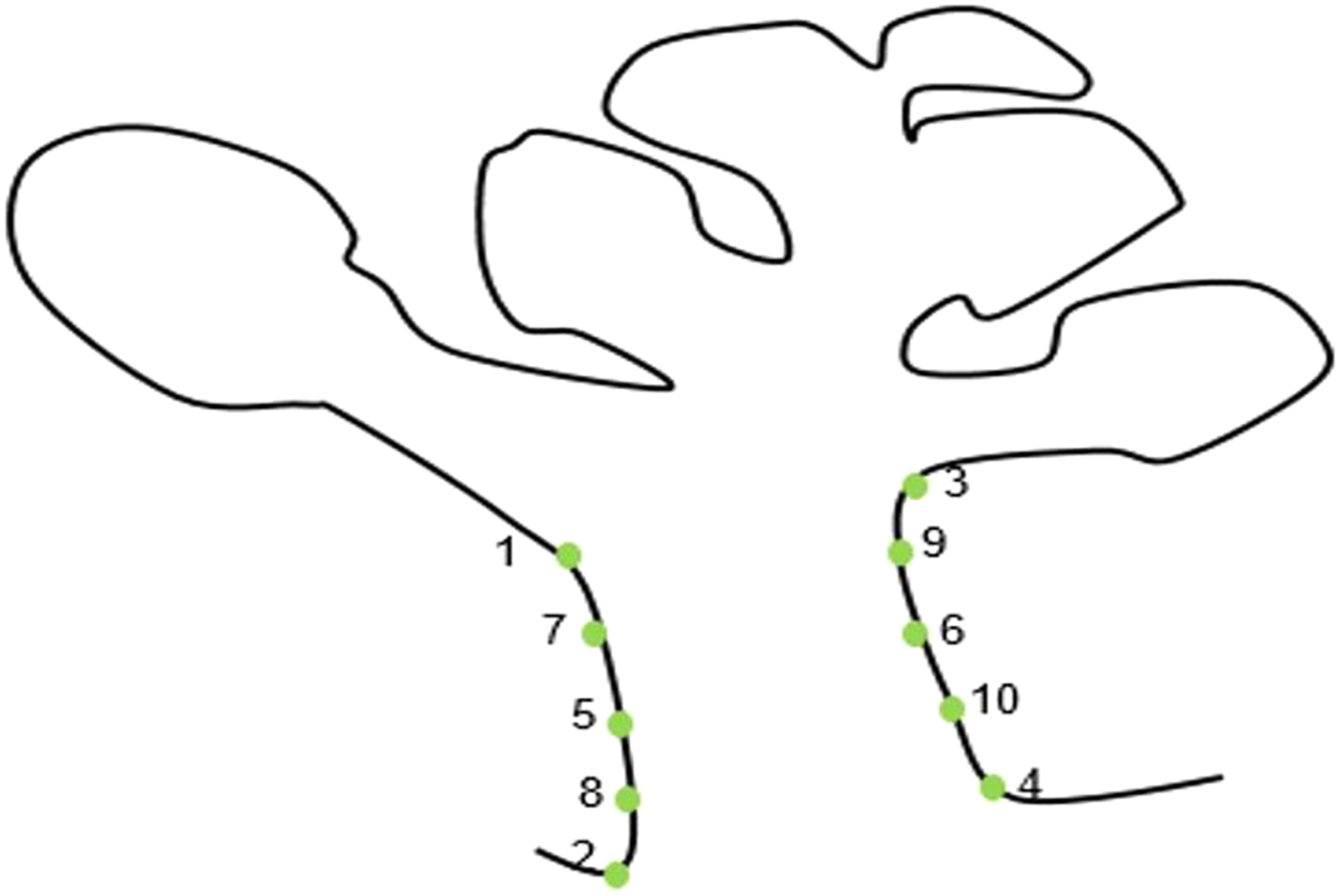
Measurement protocol
Scans were analysed using ImageJ.
1
The cochlea and IAC were located on the CT image stack, rotated and oriented in the cochlear view Figure 2.
16
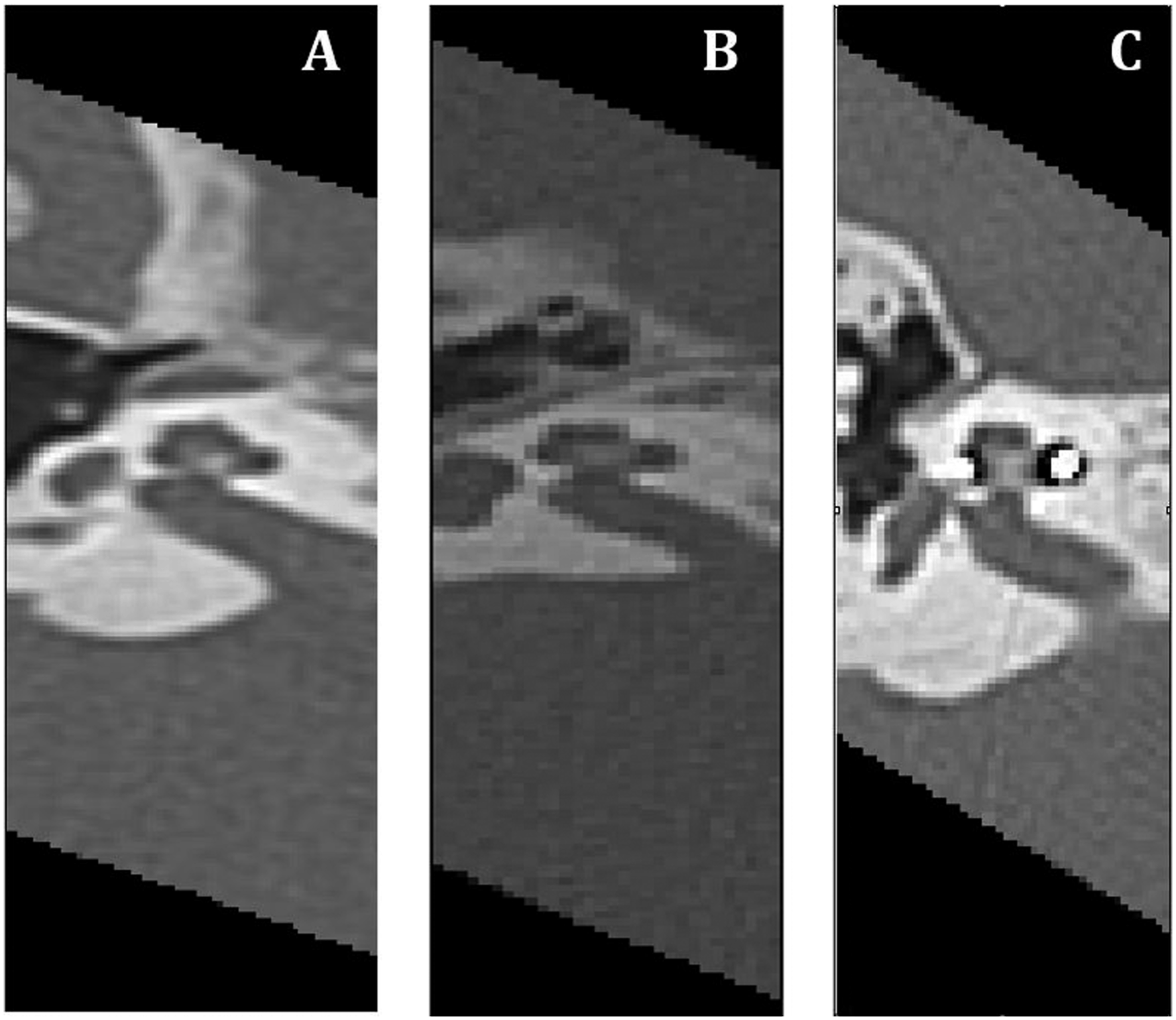
The image stack was resliced radially from the centre of the modiolus at 1° increments for 360°, resulting in a set of 360 mid-modiolar images from which the IAC dimensions could be measured. Using the round window as a zero-reference angle, the landmarks defined in Table 1 were selected and measured at 5-degree intervals Figure 3. (A) cochlea rotated into the cochlear view. Yellow line drawn through the modiolus for radial reslicing. (B) Slice 0 of 360 of cochlea and the internal auditory canal sliced through the modiolus. (C) Landmarks one to 10 plotted on the radially resliced stack. (A–C) represent examples of the three different shapes of the internal auditory canals from three different participants. Using the measurements describes these internal auditory canals were classified as (A) funnel-shaped, (B) cylindrical and (C) bud-shaped.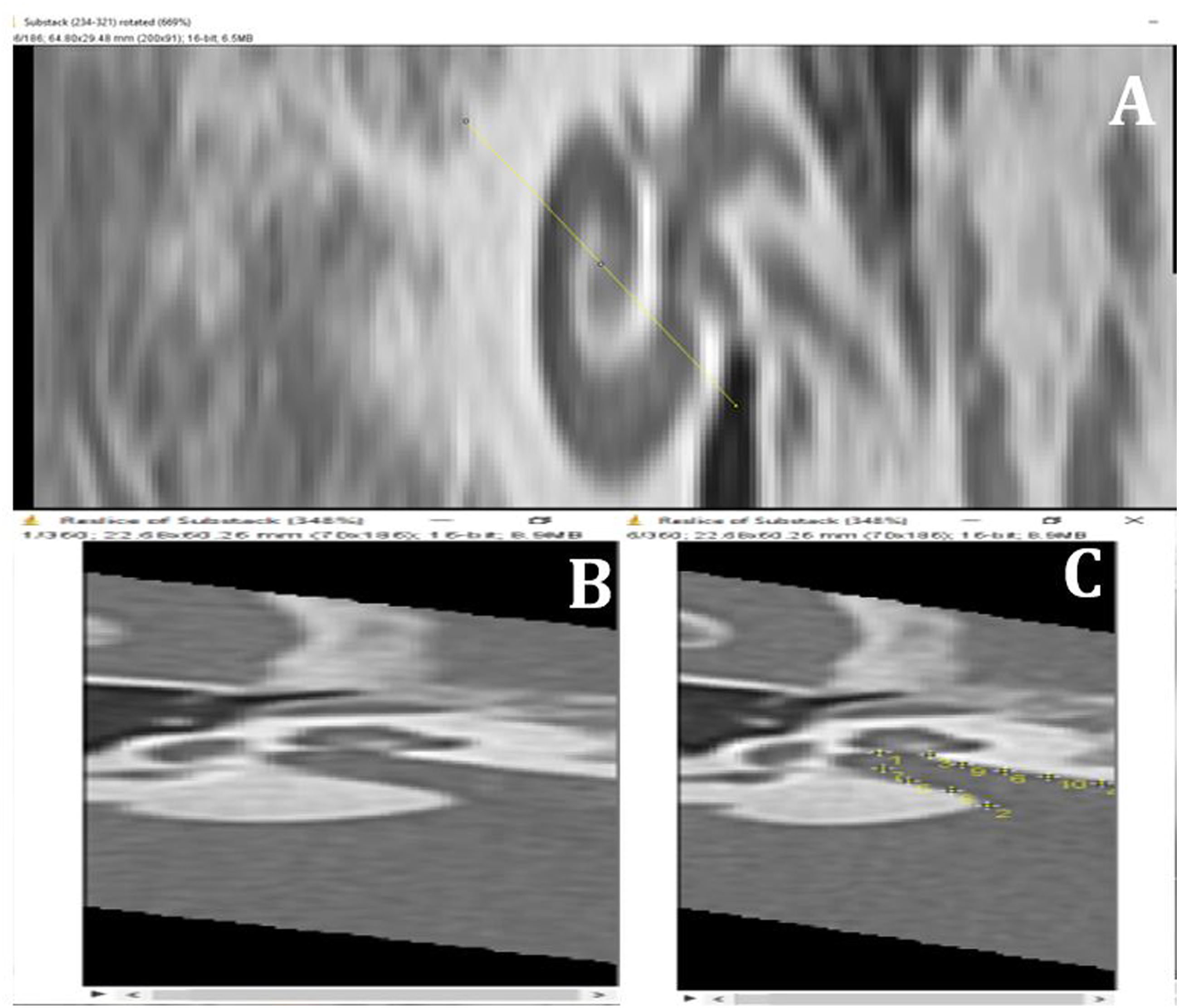
Main outcomes measurements
The following measurements were calculated to validate our data and to compare the dimensions of the IAC of a South African population to those measured in the literature: 1. AP diameter at the base of the basal turn of the cochlea (APDB), that is, the distance between landmarks 1 and 3. 2. AP diameter at the midpoint of the IAC (APDM), that is, the distance between landmarks 5 and 6. 3. Opening diameter of the IAC, that is, the distance between landmarks 2 and 4. 4. The anterior length of the IAC, that is, is the distance between landmarks 1 and 2. 5. Posterior length of the IAC, that is, the distance between landmarks 3 and 4.
Landmarks 7–10 were not used to make any measurements, but they are important for defining the shape of the IAC for 3D model generation.
Statistical analysis
Descriptive statistics were reported for each defined point of reference. A paired t-test was performed to compare the dimensions of the right and left IAC. An unpaired t-test was performed to compare the dimensions of the IAC of men and women. The tests were performed with a 95% confidence interval. The significance level was established at P < 0.05. Repeatability was assessed through intra-observer and interobserver agreement with interclass correlation (ICC).
Results
Dimensions of the IAC
Resulting dimensions in mm of the internal auditory canal from 42 internal auditory canals viewed on CT scans.
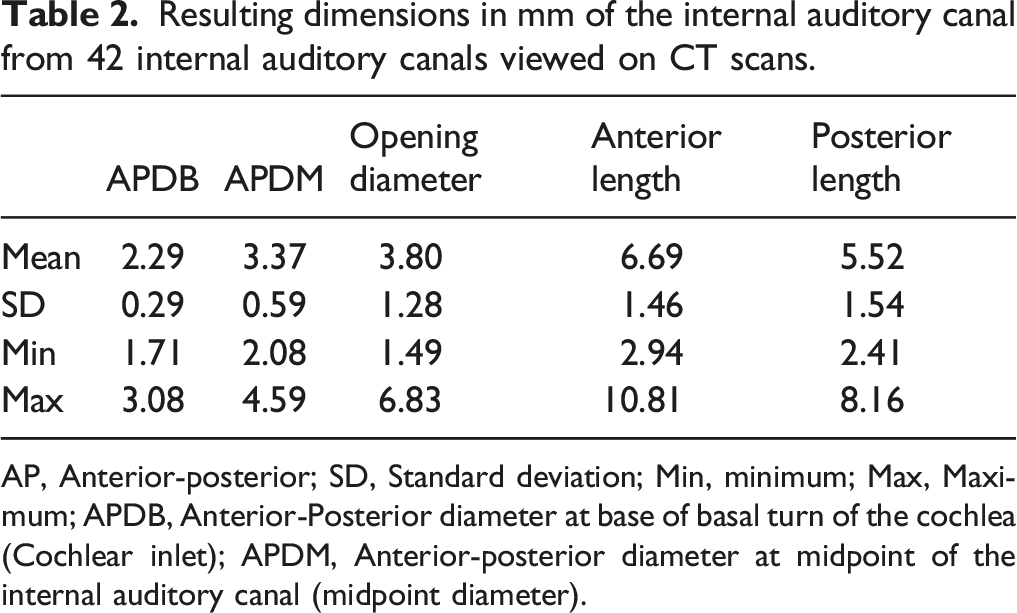
AP, Anterior-posterior; SD, Standard deviation; Min, minimum; Max, Maximum; APDB, Anterior-Posterior diameter at base of basal turn of the cochlea (Cochlear inlet); APDM, Anterior-posterior diameter at midpoint of the internal auditory canal (midpoint diameter).
Left vs right IACs
Results of the paired t-test comparing the diameters of the left and right internal auditory canals. Mean ± standard deviation and P-values are summarised in the table below.
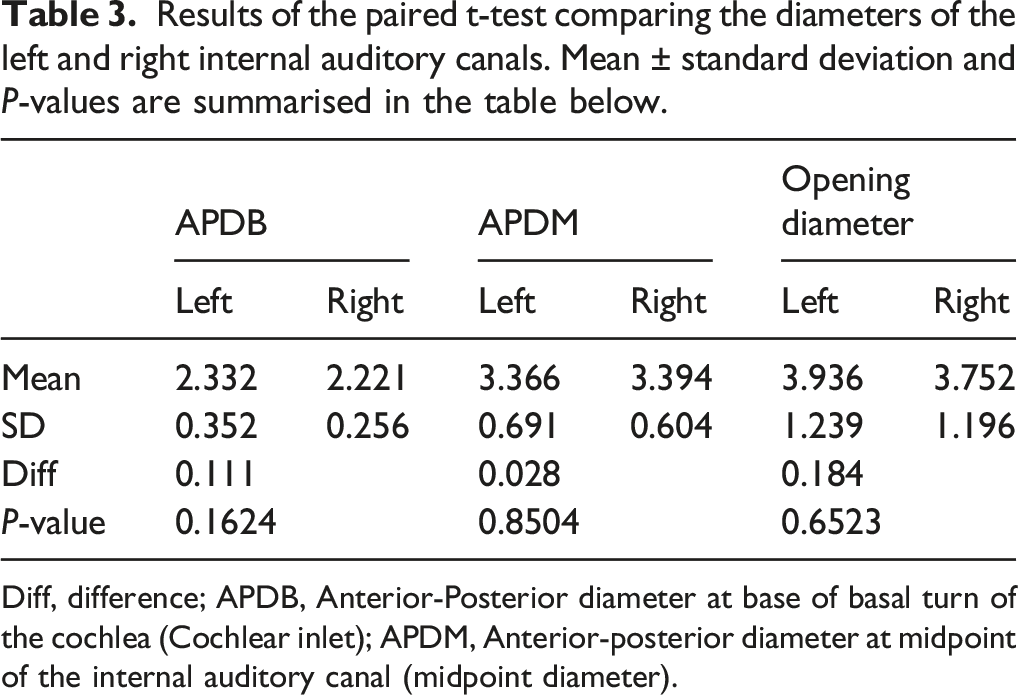
Diff, difference; APDB, Anterior-Posterior diameter at base of basal turn of the cochlea (Cochlear inlet); APDM, Anterior-posterior diameter at midpoint of the internal auditory canal (midpoint diameter).
The significance level was established at P < 0.05. All P-vales obtained were > 0.05; therefore, no statistically significant differences were found between the diameters of the left and right IACs of the sample.
Male vs female
Results of the two-sample t-test comparing the diameters and lengths of the internal auditory canal between males and females. Mean ± standard deviation and P-values of the test are summarised in the table below.
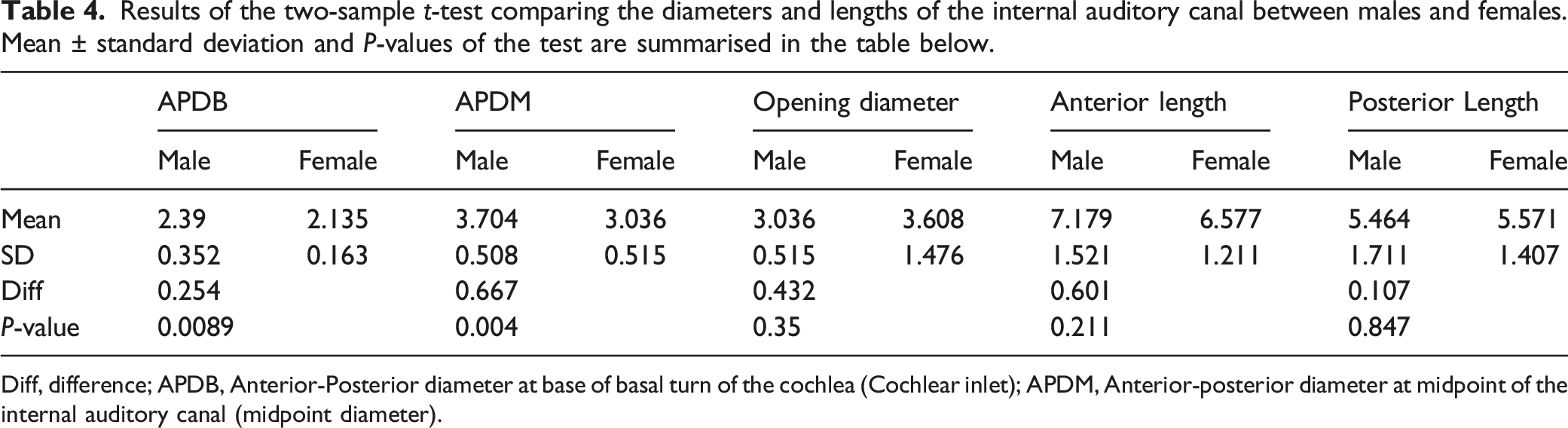
Diff, difference; APDB, Anterior-Posterior diameter at base of basal turn of the cochlea (Cochlear inlet); APDM, Anterior-posterior diameter at midpoint of the internal auditory canal (midpoint diameter).
The results show that there is a statistically significant difference between the AP diameter at the base of the basal turn of the cochlear and AP diameter at the midpoint of the IAC as the P-values are 0.0089 and 0.004, respectively, with males having a larger APDB and APDM than females. The difference in opening diameter, anterior length and posterior length was not statistically significant (P-values were 0.35, 0.211 and 0.847).
Shapes of the IAC
The most frequent shape was cylindrical at 57.14% followed by funnel shape with 40.48% and finally bud shape at 2.38%. Examples are given in Table 3.
Intra- and interobserver error
Intra-observer reliability was evaluated in 36% of the sample, and interobserver reliability was evaluated by randomly selecting five IAC to be observed by an external observer. Intra- and interclass correlation coefficients were 0.97 and 0.86, respectively. An ICC of 0.75 is considered excellent.
Discussion
Comparison to other studies
Many studied the parameters of the IAC using different modalities, such as radiographs, silicone casts, dissected and dry temporal bones, and histological sections 17 -22 and found that the dimensions and shape of the normal adult IAC vary widely. This is seen in the mean diameter of the AP at the base of the basal turn, the AP diameter at the midpoint of the IAC, and the anterior and posterior length of the IAC in this study.
The mean diameter of the AP at the midpoint of the IAC, which is known as the diameter of the IAC in most literature, was found to be 3.389 mm in the present study. In an earlier study by Valvassori and Pierce, it was reported that the mean diameter of the IAC obtained from polytomography was 4.00 mm 5 while Olivares & Schuknecht using histological sections reported a mean diameter of 3.72 mm. 23 A study of 14 male Iranian temporal bones reported a mean IAC diameter of 3.69 mm. 19 Magnetic resonance imaging was used to investigate the morphology of 7572 IAC and reported a mean diameter of 5.93 mm. 24 El Sadik and Shaaban 3 reported a mean diameter of 5.27 mm. The diameter in the present study is smaller than reported in the literature. The variation in results suggests that there is a difference in IAC dimensions between populations and highlights that existing studies cannot be used to infer or extrapolate information for a population. The difference in imaging modality, technique used to measure and the places in the canal where these measurements were taken may vary from one investigator to another. In the present study, the measurements were derived from the landmark coordinates.
Regarding the left and right IAC of an individual, there is agreement between previous studies 4,17,25 and the present study. No statistically significant differences were found between the diameters of the IAC of the right and left IACs. The difference between the right and left IAC was found to be less than 1 mm in multiple studies, a difference greater than 2 mm between the two sides of the same individual is suggestive of the presence of a vestibular schwannoma or other tumour. 19,26 The presence of a tumour causes a widening of the IAC usually at the porus which affects the opening diameter while the APDB (cochlear inlet) is rarely affected 27,28 resulting in the difference in diameters between the normal and affected IAC of an individual. In the present study, the average difference of the AP diameter at the base of the basal turn, AP diameter at the midpoint of the IAC, and the opening diameter between the right and left side did not present statistically significant differences, which is consistent with the existing literature. 29
A significant difference was found between the APDB (cochlear inlet) and APDM (midpoint diameter) of the IAC between men and women with males presenting with larger APDB and APDM; no statistical significance exists between the opening diameter anterior and posterior length of the IAC between men and women. The trend indicated that men generally have larger IAC diameters, which corresponds to the findings by previous studies, 4,5,24 while the lengths of the IAC between men and women are relatively similar. These results suggest that the diameters of the IAC could be used to differentiate between the sexes. Benson 18 found that diameter of the IAC viewed on CBCT tends to be larger and area in males; however, this difference tends to decrease with increasing age.
The factors that influence the differences in dimensions are indicative of the person-specificity of the IAC. This is significant for 3D computational cochlea modelling as well as for surgery. 29 Most of the literature agrees on the following:
1) An IAC with a diameter that is less than 2 mm is small. 3,5
2) An enlarged IAC is one with a diameter greater than 8 mm. 3,24
3) There are no significant differences between the right and left IAC exist. 20,24
4) The dimensions of the IAC differ between different population groups and sexes. 4,19,20,29,30
The IAC changes throughout development as it adapts to cranial growth and the final shape of the IAC is reached in adulthood. 25 Recently, the terms used to describe IAC shapes are funnel-shaped, cylindrical and bud-shaped. 4 The shape of the IAC is usually determined by direct inspection, 4,29 which means that it is subjective and is greatly influenced by the view and level at which the IAC is being viewed when determining the shape. However, in the present study the shape of the IAC was quantified by numerical parameters. The measurements taken, mainly the APDB and the opening diameter of the IAC, were used to classify each IAC into one of the three shapes. The IAC is said to be funnel-shaped if the opening diameter is larger in relation to the AP diameter with a difference larger than 1.5 mm, cylindrical if the opening diameter and the AP diameter are relatively similar in size with the cut-off difference of less than 1.5 mm, and lastly bud-shaped if the AP diameter is relatively larger than the opening diameter with a difference larger than 1.5 mm.
A study by Kobayashi and Zusho (1987) investigated 300 IAC and reported 4.5% funnel-shaped IAC, 72.7% cylindrical and 22.8% bud-shaped IAC. Marques, Ajzen 4 reported 58.3% of 110 IAC were funnel-shaped, 30.9% were cylindrical and only 10.8% were bud-shaped IAC. In the present study, the most common shape was the cylindrical shape with 57.14%, 40.48% being funnel-shaped, and only 2.38% being bud-shaped. This difference in proportions can possibly be explained by the difference in the populations studied and the age distribution of the sample.
Clinical applicability and generalisability
The shape of the IAC may have implications for 3D computational modelling of the cochlea, as the predictions of the current spread may be influenced by the morphology of the IAC. The trajectory of the nerve in the IAC affects neural excitation. 2
Conclusions
The study quantifies the shape and morphology of the IAC from landmark measurements on CT images. Inter-person variations observed imply that the dimensions and shape of the IAC cannot be generalised. The information from this study could help researchers reconstruct 3D computational cochlear models that include the IAC. As the shapes of the IAC have been linked to some malformations and diseases, it can be used as a diagnostic tool for otorhinologists.
Footnotes
Author contributions
NM, RH-B and TH contributed equally to the following 4 IJCME criteria: Substantial contributions to the conception or design of the work; or the acquisition, analysis or interpretation of data for the work; and Drafting the work or revising it critically for important intellectual content; and Final approval of the version to be published; and Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.