
Abstract
Approximately 7–10% of temporal bone fractures result in facial nerve paralysis. Treatment is dependent upon the severity of the nerve trauma and can range from conservative medical management to surgical intervention. A study by Hato et al. detailed the relationship between surgical timing and recovery rate for patients with facial nerve palsy secondary to temporal bone trauma. The rates of complete recovery and good recovery decline that the longer surgical intervention is delayed. We present the case of a 14-year-old male with a temporal bone fracture and delayed onset right-sided facial paralysis. This patient was treated with a transmastoid middle cranial fossa (MCF) approach with intraoperative electrical stimulation of the perigeniculate portion of the facial nerve. Despite a 53-day delay between trauma and surgical intervention, the patient’s facial function improved from House Brackmann (HB) grade VI to grade II within 6 months. Intraoperative facial nerve stimulation, which we have previously used for unresolved Bell’s palsy, may be useful for patients with post-traumatic, persistent facial paralysis.
Introduction
We present a case of persistent, post-traumatic facial paralysis treated with facial nerve intraoperative electrical stimulation, performed through a transmastoid, internal middle fossa approach.
Case presentation
A 14-year-old male presented to us after an ATV accident in which he sustained severe blunt head trauma, bilateral temporal bone fractures, and delayed onset right-sided facial paralysis. The patient was initially informed that the facial function would return to normal after 3 months. A subsequent neurosurgical consultation suggested that the paralysis may instead be permanent, and a more complex facial reanimation procedure was recommended. After a lack of improvement in his facial paralysis 45 days after initial injury, the patient presented to our clinic and was offered intraoperative electrical stimulation of the facial nerve.
Physical examination demonstrated a HB grade VI right-sided facial paralysis and normal left facial function. Microscopic otoscopy showed an anteriorly displaced malleus in the right ear. The audiogram from 6 days after the accident showed bilateral symmetric conductive hearing loss with normal sensorineural function. MRI showed swelling of the facial nerve in the region of the geniculate ganglion on the right, but no true fracture line.
Fifty-three days after initial trauma, the patient underwent a transmastoid MCF approach for facial nerve intraoperative electrical stimulation with incus interposition ossiculoplasty. Positive findings at time of surgery included a superficial aneurysmal wall of the sigmoid sinus, old blood in the mastoid cavity, and disarticulation of the ossicular chain with the malleus being anteriorly dislocated and separated from the incus. The patient also had a hypermobile stapes that was not attached to the ligamentous annulus of the oval window. The facial nerve was exposed near the cochleariform process with a right-angle hook. It was edematous and there was blood deep to the perineurium with microscopic fragments of bone embedded in the nerve. The perineurium was incised and irrigated.
Stimulation was introduced initially at 0.1 mA, increased by 0.2 mA increments, until a definitive response was obtained at 0.9 mA (Figure 1). The intraoperative electrical stimulation was then delivered for 30 seconds. There were no perioperative complications. Intraoperative electrical stimulation of the facial nerve (arrow, stimulation probe).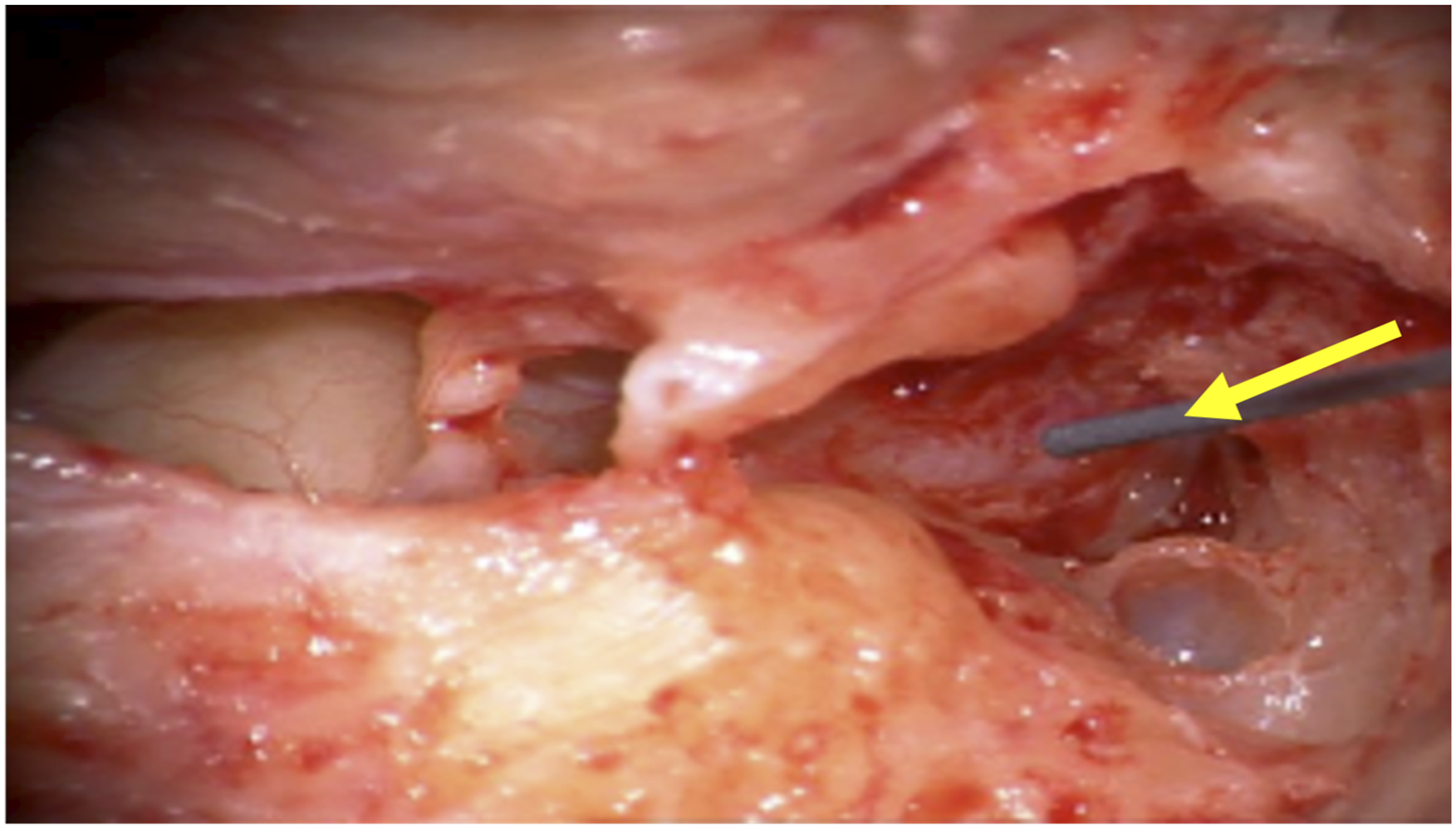
The patient had normal wound healing with an excellent initial outcome. His face at rest was very symmetric, midface movement improved with smiling, and near-complete eye closure at 1 month with HB grade III function. The patient then initiated facial retraining physical therapy, and today has HB grade II function with minimal synkinesis (Figure 2). Patient preoperatively (right) and 4 months postoperatively (left).
Discussion
Approximately 7–10% of temporal bone fractures lead to facial nerve paralysis, likely secondary to nerve edema, compression by hematoma, or delayed arterial spasm.1‐4 The current standard of care for facial palsy secondary to blunt traumatic nerve injury is conservative medical management or surgical decompression depending on the severity of the nerve injury. 5 If electroneurography (ENoG) demonstrates greater than 90% degeneration of nerve fibers within the first 2–3 weeks after paralysis or EMG shows no regeneration signs after 3 weeks, surgical intervention may be indicated.4,6,7 In patients with serviceable hearing, most surgeons will use the middle cranial fossa (MCF) approach, which allows access for decompression of the facial nerve from the cisternal to the proximal tympanic segments while preserving auditory and vestibular function. 5 It has also been well-established that edema and subsequent degenerative and fibrotic damage after severe injury significantly impact the labyrinthine segment. 8 A study by Hato et al. detailed the relationship between surgical timing and recovery rate for patients with facial nerve palsy secondary to temporal bone trauma. 9 The longer the delay between onset of paralysis and surgical intervention, the possibility for complete or good recovery becomes increasingly less likely. As related to our patient, the rates of complete recovery and good recovery were 35.3% and 70.6%, respectively, when decompression surgery was performed at 1–2 months after trauma.
As detailed in the literature, facial nerve decompression alone may result in poor functional recovery. Additional therapies should therefore be considered. While this has not been specifically studied in the facial nerve in a trauma setting, intraoperative electrical stimulation has been shown to accelerate motor nerve regeneration after peripheral nerve injury requiring surgical intervention.10,11 Electrical stimulation increases neuronal cyclic adenosine monophosphate and subsequently expression of neurotrophic factors and growth genes leading to nerve recovery and restoration of muscle function. 10 Electrical stimulation has also been detailed in the case of Bell’s palsy. Tuncay et al. studied stimulation in addition to physical therapy and found improved facial movement and electrophysiological outcome at 3 months. 12 A study by Kim and Choi found subthreshold stimulation in addition to medical therapy compared to medical therapy alone significantly improved recovery in patients with Bell’s palsy. 13
Our alternative approach combines a modified version of the current standard surgical technique with additional intraoperative electrical stimulation. In our experience, a transmastoid approach for facial nerve decompression is adequate to obtain access to the facial nerve from stylomastoid foramen to the perigeniculate region. The operative procedure performed for this patient involved identifying the facial nerve with only 1 mm of bone removal, proximal to the cochleariform process. This is all that is needed to allow placement of a facial nerve stimulator. The facial recess is opened so the stapedial tendon can be visualized. The nerve is stimulated until a definitive response is seen with stapedial contraction and heard by the monitoring unit. The nerve is then stimulated for 30 seconds at that level. The wound is closed in the usual fashion.
There is no need for extensive decompression of the nerve because the end result is related to electrical stimulation near the geniculate ganglion, not decompression. After utilization of this technique, our patient recovered remarkably well in contrast to both the initial outside predicted prognosis and what has been detailed in the literature.
Conclusion
Patients with severe facial nerve paralysis secondary to temporal bone fracture may benefit from intraoperative electrical stimulation through a transmastoid approach. The senior author, Dr. Leonetti, has shown significantly improved facial function with less synkinesis in patients who underwent electrical stimulation (2012–present) versus bony decompression alone (1988–2011) for Bell’s palsy. 14 Perhaps a similar study can be devised as a multi-institutional study for persistent, post-traumatic facial paralysis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The Loyola University Chicago Health Sciences Campus Institutional Review Board does not require review for case reports that involve a single patient. The patient and legal guardian consent to the patient’s information being published in this manuscript.