
Abstract
Objectives
To investigate the prognosis and quality of life for primary malignant maxillary sinus tumors.
Methods
This was a retrospective analysis. 164 patients diagnosed with primary malignant maxillary sinus tumors between 2005 and 2018 were recruited. Patients were treated according to the pathological type and the lesion range. Prognostic differences of different pathological types, surgical resection methods, repair methods, treatment methods, and different local recurrence sites were analyzed. Survival analysis and prognostic factors analysis were performed.
Results
Overall survival (OS) rate was 74.7% at 3 years, 60.5% at 5 years, and 45.8% at 10 years. Disease-free survival (DFS) rate was 67.2% at 3 years, 45.6% at 5 years, and 30.8% at 10 years. There was significant difference in OS rate among different pathological types (χ2 = 14.18, P < 0.05). The order of 5-year OS rate was as follows: malignant transformation of inverted Papilloma (77.7%) > adenoid cystic carcinoma (74.1%) > squamous cell carcinoma (48.4%) > sarcoma (22.1%). The order of disease-free survival was as follows: total maxillary resection > subtotal maxillary resection > endoscopic nasal tumor resection ≥enlarged maxillary resection, the 5-year DFS rate were 68.6%, 53.5%, 46.2%, and 42.9%, respectively. The OS of postoperative radiotherapy was significantly better than that of preoperative radiotherapy (χ2 = 7.16, P < 0.05). There was significant difference in OS between recurrent and non-recurrent patients (χ2 = 68.57, P < 0.05).
Conclusions
The pathological type and the timing of radiotherapy are independent prognostic factors for primary malignant tumor of maxillary sinus. In addition, different local surgical resection methods are independent factors affecting the recurrence rate.
Introduction
Malignant tumors of the nasal cavity and paranasal sinuses are the most common malignant tumors at the base of the nasal skull. They account for 0.2%–0.8% of all malignant tumors, 1 and they are most commonly found in the maxillary sinus, accounting for 60%–70% of tumors in this area. Due to the concealed location, they are often missed in the early stage. 2 Moreover, they often invade the eye socket, skull, and other important structures in the late stage, making complete resection difficult, and resulting in poor long-term survival rate.3,4 The 5-year overall survival rate is 52–57.5%. 5 Surgery combined with radiotherapy can reduce the recurrence and metastasis of maxillary sinus carcinomas and is currently accepted as the standard treatment method. 6 Patients who received adjuvant radiotherapy, adjuvant chemotherapy, or neoadjuvant therapy had improved overall survival compared with surgery alone. 7 There were also many ways to reconstruct the maxillary, which include pedicled flaps such as temporal muscle flap, 8 free flaps including lateral femoral circumflex flap, 9 fibular flap, 10 composite flaps.11,12 As the diverse pathological types and different range of lesions of the tumor, 2 as well as the difference regarding the patients’ physical conditions, economic status, requirements for quality of life. Prior to treatment, an individualized comprehensive treatment plan should be made by a multidisciplinary team (MDT). 13 Based on the above factors to design individualized comprehensive treatment regimens, we have established a system of MDT discussion for sinonasal malignancies since 2005. To investigate the prognostic impact of individualized treatment of primary malignant neoplasm of the maxillary sinus, we retrospectively reviewed the clinical data of 164 patients diagnosed from January 2005 to December 2018, so as to provide reference for the treatment of maxillary sinus malignant tumor.
Patients and Methods
Patients and Study Design
Case inclusion criteria: This retrospective study used data of patients with primary malignant tumors originated from the maxillary sinus underwent surgical interventions in Otolaryngology Head and Neck Surgery Department of Beijing Tongren Hospital between January 2005 and December 2018. Among 175 cases of malignant tumors, 11 cases were lost to follow-up within three months after operation, and 164 cases were effective cases, all of which had complete clinical data. All patients were evaluated with CT and MRI of the paranasal sinuses before surgery, and those whose lesions protruded into the nasal cavity underwent preoperative local anesthesia to obtain biopsies to clarify the pathological nature, and cTNM staging was diagnosed according to the AJCC 8th edition staging manual. The diagnosis was made in terms of individualized diagnosis and surgical intervention has been performed according to discussion of MDT in otolaryngology head and neck surgery group, the adjuvant treatments included radiotherapy and chemotherapy. The exclusion criteria involved the following items. 1) pathologically, patients with malignant melanoma (due to its significant difference in degree of malignancy and prognosis from that of other tumor types); 2) patients with simultaneous presence of systemic distant metastasis; and 3) patients who dropped out immediately after treatment and failed to complete the preset treatment plan.
Surgical Procedures
Prior to treatment, treatment plans were designed by a MDT for all 164 patients. Surgeries were performed in our department. Surgical modalities included: subtotal maxillary condylectomy, total maxillary condylectomy, extended maxillary condylectomy, and endonasal surgery. Reconstruction modalities included temporalis flap repair, anterolateral femoral flap, peroneal flap, septal flap, submental flap, rectus abdominis flap, and frontal flap.
Adjuvant Treatments
Adjuvant therapies, such as radiotherapy, chemotherapy, targeted therapy, and concurrent chemoradiotherapy, were recommended postoperatively according to patient’s pathological classification and TNM staging. The preoperative radiotherapy dose was 60–65 Gy, the postoperative radiotherapy dose was 60–70 Gy, and the chemotherapy regimen included TPF, TPI, that is, EP and regimen and the targeted therapy included Endo and Nimotuzumab. For patients with postoperative local recurrence, an extended tumor resection combined with flap surgery and / or lymph node dissection was performed according to the site of recurrence, and then radiotherapy or concurrent chemoradiotherapy was performed. For patients with distant metastasis, chemotherapy or concurrent chemoradiotherapy were performed according to the patient’s physical conditions and willingness.
Prognostic Assessments
Overall, 94% of the 164 patients were followed up by the end of treatment to December 2018 or to the time of death or loss to follow-up. The total number of patients with follow-up for 3, 5, and 10 years was 86, 56, and 13, respectively. After treatment, the patients were reviewed every three months within one year, every six months within five years, and every year after five years. Computed tomography (CT) and magnetic resonance imaging (MRI) and nasopharyngoscopy were performed during the follow-up period. The patients were followed up for 12 to 156 months, with a median of 50.4 months, with 80 patients (48.8%) having more than 5 years and 111 patients (67.7%) having more than 3 years. The prognosis evaluation indicators mainly used OS and DFS and other indicators. OS was calculated as the period from the date of diagnosis to the date of death from any cause or the date of last follow-up. Disease-free survival (DFS) was defined as progression from the date of diagnosis to the date of recurrence or death due to cancer progression
Statistical Analysis
IBM SPSS Statistics software was used for data analysis. Chi square test was used to compare the categorical variables. Kaplan Meier and log rank tests were used to evaluate OS and DFS rates. Cox regression models were used to evaluate the relationship between treatment and survival. P values < 0.05 were considered statistical significance.
Results
Demographics of the Study Population
Demographic, clinical characteristics, patients receiving local and flap surgeries of 164 patients with primary malignant tumors of the maxillary sinus.
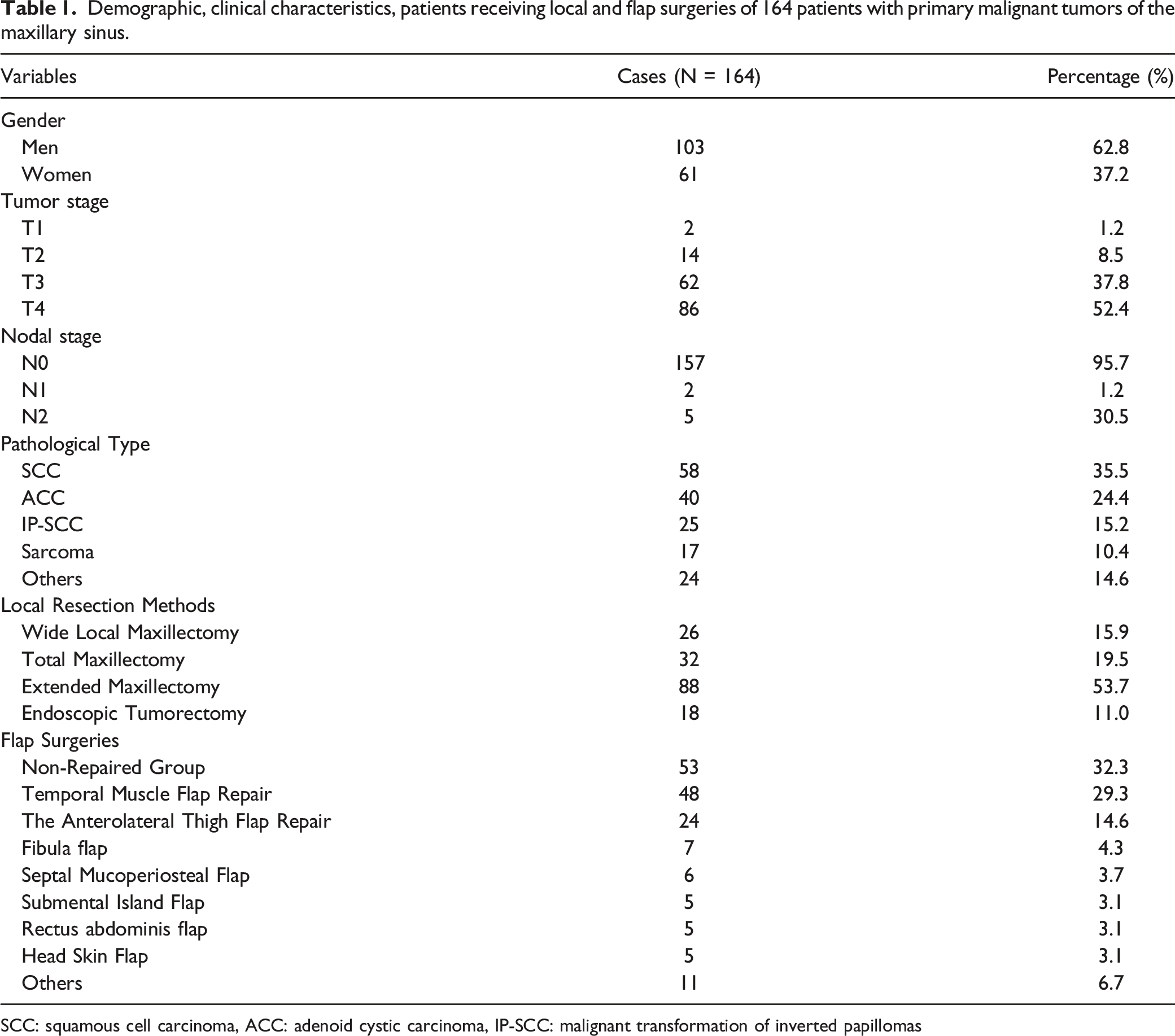
SCC: squamous cell carcinoma, ACC: adenoid cystic carcinoma, IP‐SCC: malignant transformation of inverted papillomas
Prior to treatment, treatment plans were designed by a MDT for all 164 patients. Surgeries were performed in our department; the follow-up rate was 94%. 18 (11.0%) patients received surgery alone; 142 (86.6%) received adjuvant radiotherapy, of which, 13 (7.9%) received radiotherapy preoperatively, 124 (75.6%) received radiotherapy postoperatively, and 5 (3.0%) received repeated radiotherapies both pre- and postoperatively; 64 (39.0%) received adjuvant chemotherapy and 13 (7.9%) received concurrent chemoradiotherapy. Among the 164 patients, 107 (65.2%) received the initiated surgery in our hospital, and 57 (34.8%) received the reoperation in our hospital. The surgical approaches are shown in Table 1.
The Entire Prognosis Status
As regarding the results of survival analysis: Overall, 61 (37.2%) patients died during the follow-up period, among which, 27 (16.5%) died from local recurrence. 28 (17.1%) died from distant metastasis (4 patients with bone metastasis, 8 patients with lung metastasis, 5 patients with brain metastasis, and 11 patients with multiple systemic metastases), and 6 patients (3.7%) died from causes other than maxillary sinus tumors. The 3-year, 5-year, and 10-year cumulative survival rates were 74.7%, 60.5%, and 45.8%, respectively (Figure 1A). Survival curve of 164 patients with primary malignant tumors of maxillary sinus. A: Cumulative survival curve; B: Disease-free survival curve; C: Comparison of the cumulative survival rates of 164 patients with different pathological types of primary malignant tumors of the maxillary sinus showed statistical significance (χ2 = 14.18, P < 0.05); D: Comparison in disease-free survival rates of patients who underwent different local resection methods showed statistical significance (χ2 = 8.64, P = 0.02); E: Comparison of the cumulative survival rates of patients who underwent different local resection methods showed no statistical significance; F: Comparison of the cumulative survival rates of patients who received either preoperative or postoperative radiotherapy showed statistical significance( χ2 = 7.17, P < 0.05)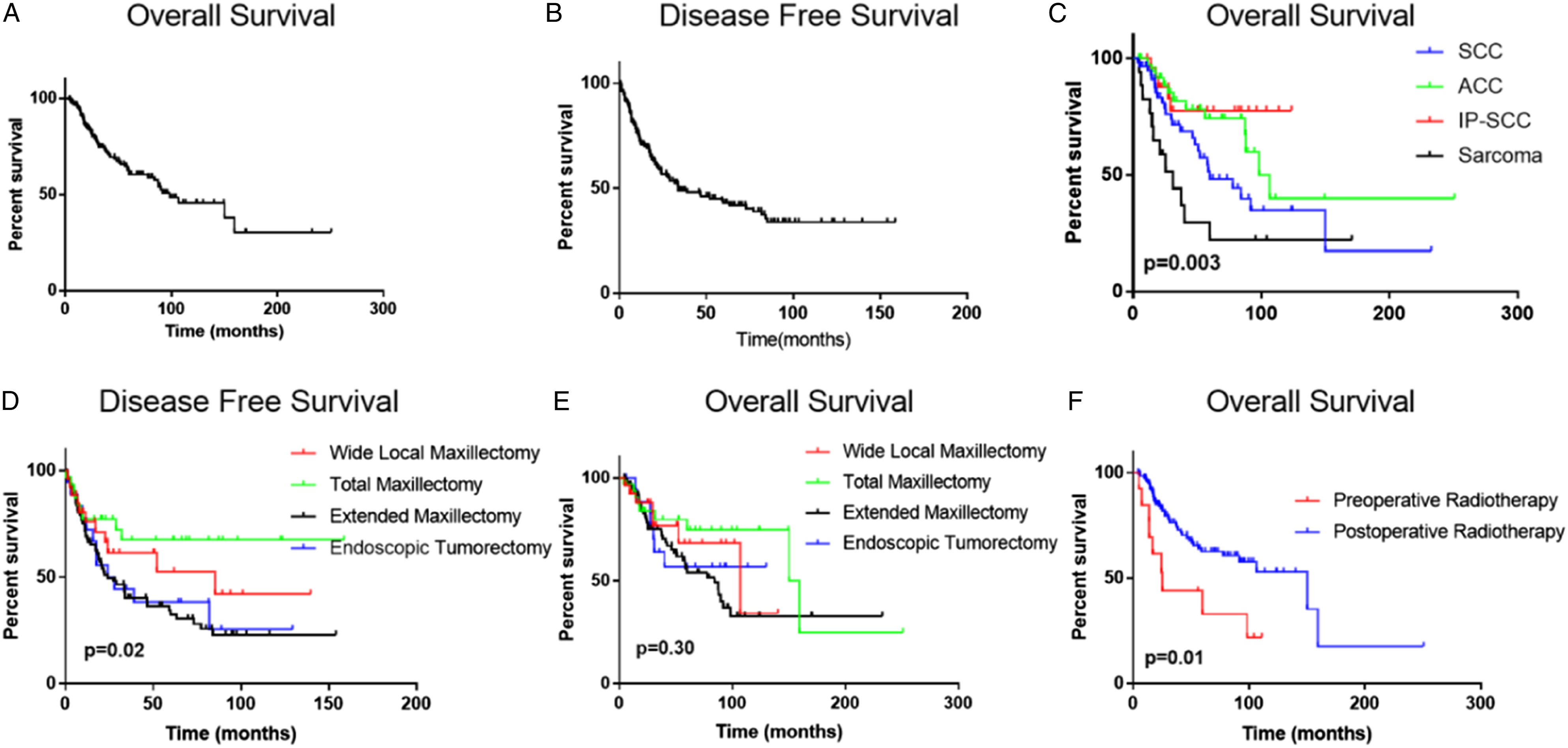
Concerning the recurrence and disease-free survival rate, recurrence was observed in 84 (51.2%) cases. Among the 84 cases, 42 (25.6%) had local recurrence, 9 (5.5%) had lymph node recurrence, and 33 (20.1%) had distant metastasis. The 3-year, 5-year, and 10-year cumulative disease-free survival rates were 67.2%, 45.6%, and 30.8%, respectively (Figure 1B).
Comparison between the survival rates of patients who underwent first surgery in our hospital and those who were operated at other hospitals: Of all the patients, 107 underwent the first surgery in our hospital, 57 underwent the initiated surgery in other hospitals and the reoperation in our hospital. The differences in the cumulative survival and disease-free survival rates between the two groups were not statistically significant (P > 0.05).
Comparison of Prognosis Based on the Characters of Tumor
Pathological type and prognosis analysis: Among all the patients, differences in cumulative survival rates of patients with the first four pathological types were statistically significant (χ2 = 14.18, P < 0.05). The survival rate in a decreasing order was as follows: IP-SCC> ACC > SCC > sarcoma (Figure 1C). OS rate were 77.7%, 74.1%, 48.4%, and 22.1%, respectively, at 5 years. The differences in disease-free survival rates among different pathological types were not statistically significant (P > 0.05).
Comparison of Prognosis Experienced Individualized Treatments
Comparison of the cumulative survival and disease-free survival rates of patients who underwent different local resection methods for primary malignant tumors of the maxillary sinus
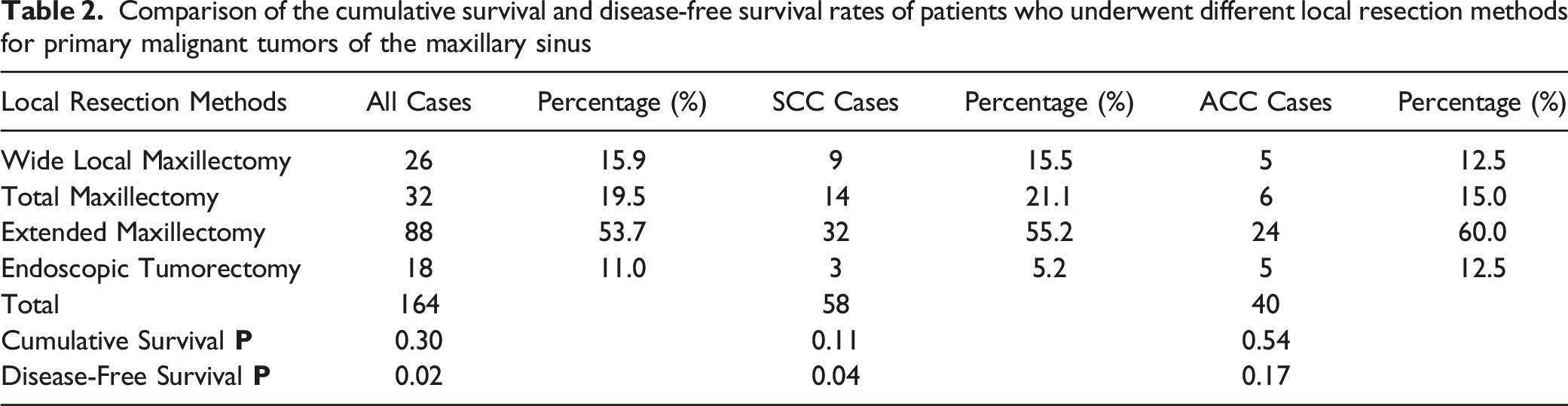
The disease-free survival was total maxillectomy > wide local maxillectomy > endoscopic tumorectomy ≥ extended maxillectomy. In the whole cohort of cases, DFS rate were 68.6%, 53.5%, 46.2%, and 42.9%, respectively, at 5 years. However, the difference between the cumulative survival rates of patients who underwent different local resection methods was not statistically significant (χ2 = 1.20, P > 0.05; Figure 1E). Moreover, no significant difference was found among different pathological types in the T3T4 group.
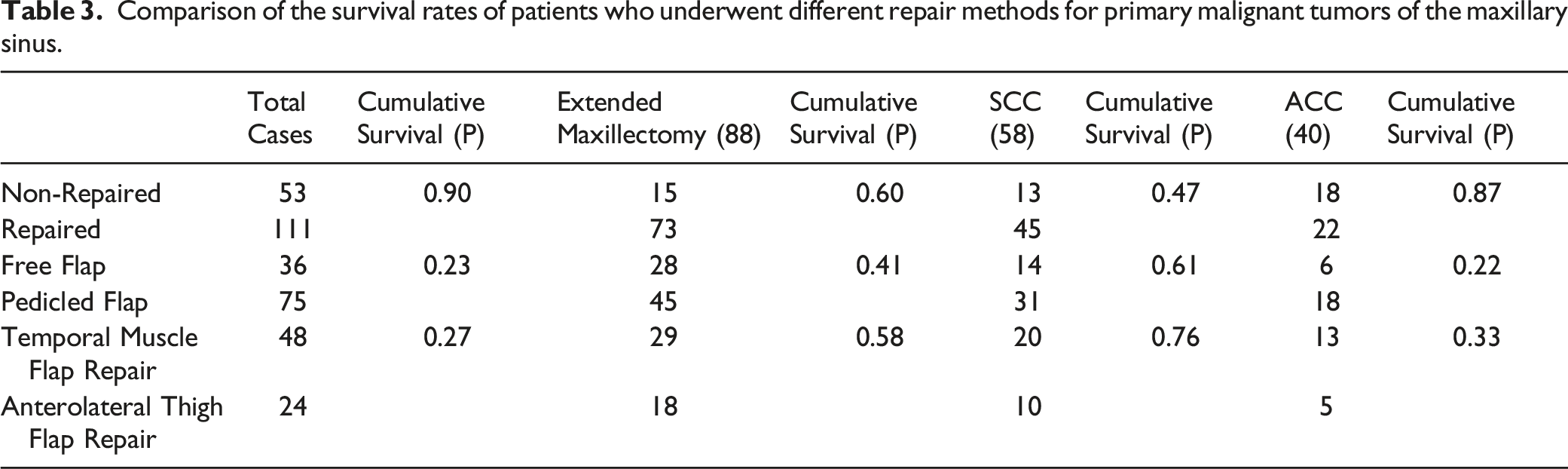
Comparison of the survival rates of patients who underwent different repair methods for primary malignant tumors of the maxillary sinus.
Prognosis analysis of surgery alone and combined therapy: The postoperative radiotherapy group (124 cases, 75.6%) had a statistically significant overall survival rate (χ2 = 7.17, P < 0.05) than the preoperative radiotherapy group (13 cases, 7.9%). In squamous cell carcinoma patients, the survival rate of post-operation radiotherapy is significantly better than that of pre-operation radiotherapy (χ2 = 6.36, P = 0.01; Figure 1F). The surgery-alone group (18 cases, 11.0%) had no statistically significant differences in overall survival and disease-free survival rates compared with the combined surgery and radiotherapy group (129 cases, 78.7%) and the combined surgery and concurrent chemoradiotherapy group (13 cases, 7.9%).
Site of local recurrence and prognosis analysis: Except for two patients with unknown recurrence, significant differences were noted between the cumulative survival rate of patients without recurrence (78 cases, 45.7%) and of those with recurrence (84 cases, 51.2%; χ2 = 68.57, P < 0.05). However, according to the site of recurrence, no significant differences were noted between the cumulative survival rates of patients with local recurrence, lymph node metastasis and distant metastasis.
Multivariate Analysis of Factors Affecting Prognosis
Cox proportional hazards model.
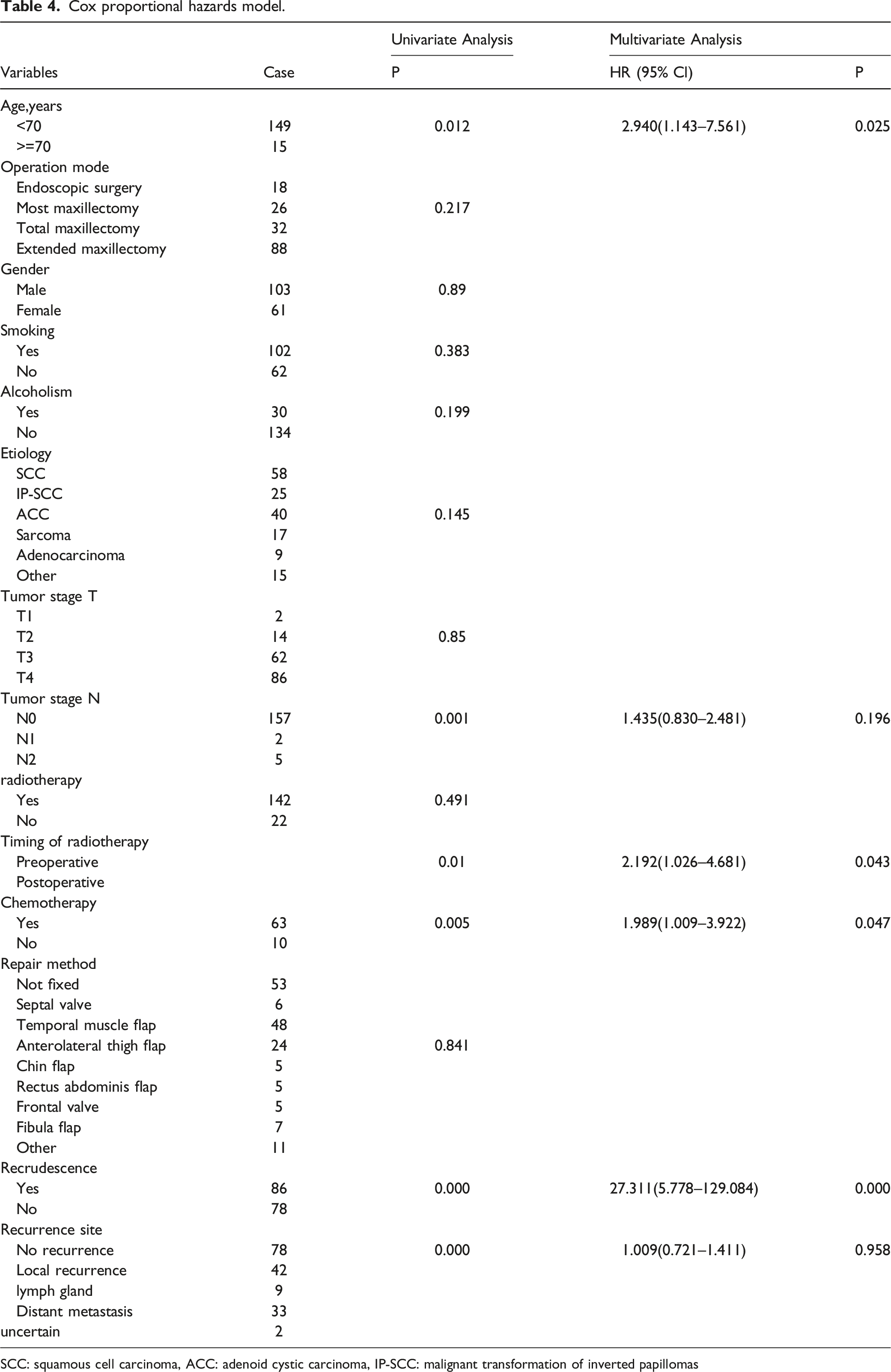
SCC: squamous cell carcinoma, ACC: adenoid cystic carcinoma, IP‐SCC: malignant transformation of inverted papillomas
Discussion
Malignant tumors of the paranasal sinus are uncommon with an annual incidence of 1 per 10000 persons. 14 They account for 0.2%–0.8% of all malignant tumors and mainly occur in the maxillary sinus (60%–70%). 1 Most patients with obvious symptoms are already in the middle and advanced disease stages. The invasion of surrounding tissues such as the nasal cavity, eye socket, and the brain is often observed in patients at advanced stages, making treatment difficult, and resulting in poor and unsatisfactory long-term effects.3,4 Up to 90.3% (148 cases) of the enrolled patients were in stage III or IV. With improved microsurgical techniques, the surgery and reconstruction methods for malignant tumors of the maxillary region, as well as the adjuvant therapies have become more individualized. Discussions were made from the following aspects, in order to explore the effect of a different treatment plan, designed with respect to pathological type, lesion range, and patient’s willingness, on survival rate.
Pathological Type and Prognosis of Maxillary Sinus Carcinoma
Although more than 90% of the enrolled patients were in advanced stages (III and IV), the overall 5-year survival rate still reached 60.5%, slightly higher than that reported in the literature 5 . It is suggested that designing individualized treatment plan through MDT discussion before treatment is helpful to improve the survival rate.
Squamous cell carcinoma is the most common pathological type of malignant tumors of the nasal cavity and paranasal sinus and accounts for 54% of all malignant tumors 7 . Characterized by slow growth and local invasion, ACC stands second among malignant tumors of the salivary glands of the head and neck. There were few lymphatic metastases cases, 15 but an easy invasion of adjacent tissues and invasive growth along nerve fibers. In advanced stages, it has high rates of local recurrence and distant metastasis (common in the lungs), and poor long-term prognosis. 16 In all enrolled patients, SCC and ACC were the main pathological types, followed by malignant transformation of inverted papillomas (15.3%), sarcoma, etc. This study showed significant differences between the cumulative survival rates of patients with different pathological types of malignant tumors of the maxillary sinus. The survival rate in a decreasing order: the malignant transformation inverted papillomas (IP-SCC) > ACC > SCC > sarcoma. Compared to the other pathological types, malignant transformation of inverted papilloma has the best prognosis. The 5-year survival rate varies from 39.6% to 72.5%.17-20 In this study, inverted papilloma malignancy of the maxillary sinus was observed in 25 cases, and their 5-year cumulative survival rate was 77.7%. ACC has a relatively good prognosis and a high 5-year survival rate. The 5-year cumulative survival rate for ACC of the nasal cavity and paranasal sinus is reported to be 61.7%–68.8%.21,22 In this study, ACC of the maxillary sinus was noted in 40 cases, and their 5-year cumulative survival rate was 74.1%. However, distant metastasis often occurs at 5–7 years after the treatment, and is most common in the lungs, resulting in low long-term survival rates. In this study, the 10-year cumulative survival rate was 40.4%.
Squamous cell carcinoma has a poor prognosis. The 5-year overall survival rate of patients with SCC of the maxillary sinus is reported to be 35%–66%.5,23 In this study, SCC was noted in 58 cases, and their 5-year survival rate was 48.4%. Due to the frequent occurrence of systemic metastasis, sarcomas have the worst prognosis. The 5-year overall survival rate for sarcomas of the head and neck is reported to be 25.6%, 24 and varies from 21% to 70% for sarcomas of the nasal cavity and paranasal sinuses.25,26 In this study, sarcomas were found in 17 patients, all in the middle and advanced stages with a 5-year survival rate of only 22.1%.
In the literature, prognoses according to pathological types are also compared. Poeschl 27 found that SCCs of the maxillary sinus had a better prognosis than non-SCC at equivalent stages (except for ACC). Tyler 7 compared the survival rates of 11160 patients and concluded that the survival rate in a decreasing order was adenocarcinoma > ACC > SCC > undifferentiated carcinoma. The results of our study were basically consistent with the literature.
Treatment Method and Prognosis of Maxillary Sinus Carcinoma
Most investigators believe that complete surgical resection should be the first choice for maxillary sinus carcinoma, assisted by combined therapies, such as radiotherapy and chemotherapy. Comparisons were made in the local resection method, repair method, and adjuvant radiotherapy.
Comparison in Resection Method:
The data from Weizman et al. 28 showed that radical ophthalmectomy had satisfactory effect for patients with cancer tissues invading the periorbital fat, extraocular muscles, optic nerve, eyeball, and eyelid skin, and preservation of eyeballs did not increase the rate of local recurrence in patients with the tumor only invading the orbital wall but not the orbital fasciae; however, preservation of eyeballs had a certain risk of recurrence in patients with the tumor only invading the orbital bone in a limited range. In this group's comparison of local surgical modalities, none of the cumulative survival rates were significantly different. However, significant differences (P < 0.05) were found in disease-free survival rates of all enrolled patients, middle-advanced stage group, and SCC group. The results suggested that the disease-free survival rate in a decreasing order was total maxillectomy > wide local maxillectomy > endoscopic tumorectomy ≥ extended maxillectomy. Therefore, the local resection method of maxillary sinus carcinoma should be based on complete tumor excision. If local resection is optional, the highly conservative range of surgical resection is unnecessary. Nasal endoscopic surgery had poor efficacy and was not preferred. Therefore, total maxillectomy should still to be the basic surgical method for maxillary sinus carcinoma.
Comparison in Repair Method and the Survival Rate
The reconstruction of maxillary defects mainly aims as soon as possible to restore the natural barrier between the oral cavity and nasal cavity, as well as the support of the eye socket and face. Thanks to the maturation of reconstruction technology, postoperative immediate repair and reconstruction have become more dominant.8-10 In repair methods, we compared the cumulative survival rates between the non-repaired group and the repair group; the free flap group and the pedicled flap group; and the temporal muscle flap repair group and the anterolateral thigh flap repair group. No statistically significant differences were found, confirming that immediate repair and reconstruction will not affect the review and prognosis of malignant tumors of the maxillary sinus. The flap repair method is not an independent factor of cumulative survival rate and disease-free survival rate for maxillary sinus carcinoma.
Comparison of the Surgery Alone and the Combined Therapy
The literature shows that surgery combined with radiotherapy can reduce the recurrence and metastasis of maxillary sinus carcinomas and is currently accepted as the best treatment method. 6 According to the analysis made by Tyler 7 on malignant tumors of the nasal cavity and paranasal sinus in 11160 cases, the overall survival rate was higher in patients receiving adjuvant radiotherapy, adjuvant chemotherapy or neoadjuvant therapy than in patients receiving surgery alone. In this study, no significant differences in overall survival and disease-free survival rates were found between the surgery-alone group (18 cases, 11.0%) and the combined surgery and radiotherapy group (129 cases, 78.7%).
This may be due to the small number of patients receiving surgery alone. However, further analysis showed that the difference in the cumulative survival rate between postoperative radiotherapy and preoperative radiotherapy was statistically significant (P < 0.05). Su et al. 29 reported that for advanced SCC of the maxillary sinus, preoperative radiotherapy yielded a lower 5-year survival rate than postoperative radiotherapy. Their analysis showed that the sensitivity of tumor tissues to radiotherapy may be enhanced by a decrease in tumor volume and hypoxia load of tissue cells, opening of the bone window, and increase in oxygenation of tissue cells postoperatively.
Sites of Recurrence and Metastasis and Prognosis of Maxillary Sinus Carcinoma
In this study, the difference in the cumulative survival rate of patients without recurrence and patients with recurrence was statistically significant (P < 0.05). However, in the sites of recurrence, the difference in the cumulative survival rate between the local recurrence and lymph node metastasis group and the distant metastasis group was not statistically significant. This suggests that tumor recurrence is a significant prognostic factor for survival rate, but different sites of recurrence have no obvious impacts on survival rates. Many studies indicated that the surgical margin is one of the important factors for recurrence. The postoperative recurrence rate is higher in patients with positive surgical margins than in patients with negative surgical margins. 30
At present, this study still has certain limitations. First, the sample size is limited, and especially after grouping, the sample size will be further reduced. Due to the limitation of the number of cases, it is impossible to further analyze the degree of tumor differentiation and the pathological types of rare tumors, and the sample size still needs to be increased in the future. At the same time, only 13 people were followed up for ten years in this group, and the number of long-term effective follow-up cases still needs to be further increased.
Conclusions
The survival rate and prognosis of maxillary sinus carcinoma are determined by multiple factors. The individualized comprehensive treatment plan designed during the MDT discussion prior to treatment can help improve the survival rate; pathological type of malignant tumor of the maxillary sinus is the main factor that affects the treatment plan and prognosis. Open total maxillectomy should be the main surgical method. Immediate repair and reconstruction can help improve the quality of life without affecting the survival rate. Sites of recurrence and metastasis after tumor treatment have little effect on prognosis. Surgery combined with postoperative radiotherapy is still the best therapeutic option for maxillary sinus carcinoma. Due to the numerous prognostic factors of maxillary sinus carcinoma, methods of formulating individualized comprehensive treatment plans according to tumor stage, pathological type, and biological characteristic warrants further discussions and studies.
Footnotes
Acknowledgements
We would like to acknowledge the reviewers for their helpful comments on this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Beijing Municipal Administration of Hospitals’ Ascent Plan [grant numbers DFL20180202], Capital Health Development Research Project [grant numbers S2018-2-2054], Beijing Natural Science Foundation Program and Scientific Research Key Program of Beijing Municipal Commission of Education [grant numbers KZ201910025034], and National Key Research and Development Program of China [grant numbers 2020YFB1312805].