
Abstract
Attempts to analyze clinical unexpected cases of laryngeal fractures based on mild symptoms and physical findings. Even though a laryngeal fracture is rare in a living patient and when happens it is related to severe airways emergency, this case reported seems important to offer a possible differential diagnosis in patients who present with the same symptoms, if no other causes have been detected, like another one benign laryngeal disease.
A laryngeal fracture (LF) can occur following external laryngeal trauma (ELT) and it could be considered an ENT emergency.1,2
Jewette identifies 392 patients showing ELT 3 during five years. Biller reports ELT 1/14,000-42,000 emergency department visits. 4 Furham describes less than 1% of all blunt traumas. 5
Generally, laryngeal injury could be more frequent in women with longer necks, especially of the supraglottis larynx. The highest percentage of ELT in males (77% vs 33%) could be usually secondary to play body contact sports, such as fighting. 6
Symptoms of ELTs are usually typical; Schaefer’s classification is useful to describe the grading of the main clinical findings.
The thyroid cartilage often hardens into bone in adult-older patients. Due to that, the thyroid cartilage loses its elasticity and cannot tolerate any trauma. 7 The main clinical signs of a laryngeal fracture are stridor, intraluminal bleeding, laryngeal edema, and vocal cord immobility. These signs could be associated with different symptoms like dyspnea, dysphagia, and pain during swallowing and dysphonia. Therefore, if a LF began with a mild clinical onset, other benign laryngeal diseases would be considered, such as Zenker’s diverticulum, laryngeal lipoma, thyroglossal duct cyst, laryngocele, and Eagle’s Syndrome.
Above all laryngocele and Eagle’s Syndrome could be related to mild clinical findings, such as foreign body in oropharynx, especially during swallowing. The first one is the laryngeal saccule filled by air, while the Eagle’s Syndrome shows an ossification of stylohyoid ligament or an abnormal elongation of styloid process.
Laryngoscopy is the gold standard to define the extent and the location of injuries. Computerized tomography (CT) scan helps to assess laryngeal anatomy and guide to the conclusive diagnosis.8-18
We report about a 56-year-old male patient with a fracture of the right superior horn of the thyroid cartilage due to sports trauma. In particular, he used to play judo and he did not remember when the trauma could happen (probably due to some strangulation techniques).
The patient had asked for an ENT examination because he felt a slight discomfort at the right lateral cervical level, without dyspnea, dysphagia, and dysphonia. The external surface of the neck had not shown any swelling or tenderness during palpation.
The first diagnostic step was laryngoscopy. Looking at oropharynx and larynx had found a mobile mucosal bulge vary in size during swallowing on the right lateral wall of larynx (Figure 1). Meanwhile, the examiner had tried to move separately hyoid bone and thyroid cartilage with manual maneuver. This maneuver usually confirms a displacement of a hyoid bone with a “bursa” at the level of the injury, but in that clinical case the bulge had not had any relationship with some hyoid bone abnormalities.
19
Laryngoscopy images: (A) a bulge of the lateral right laryngeal wall is sporadically evaluable (B).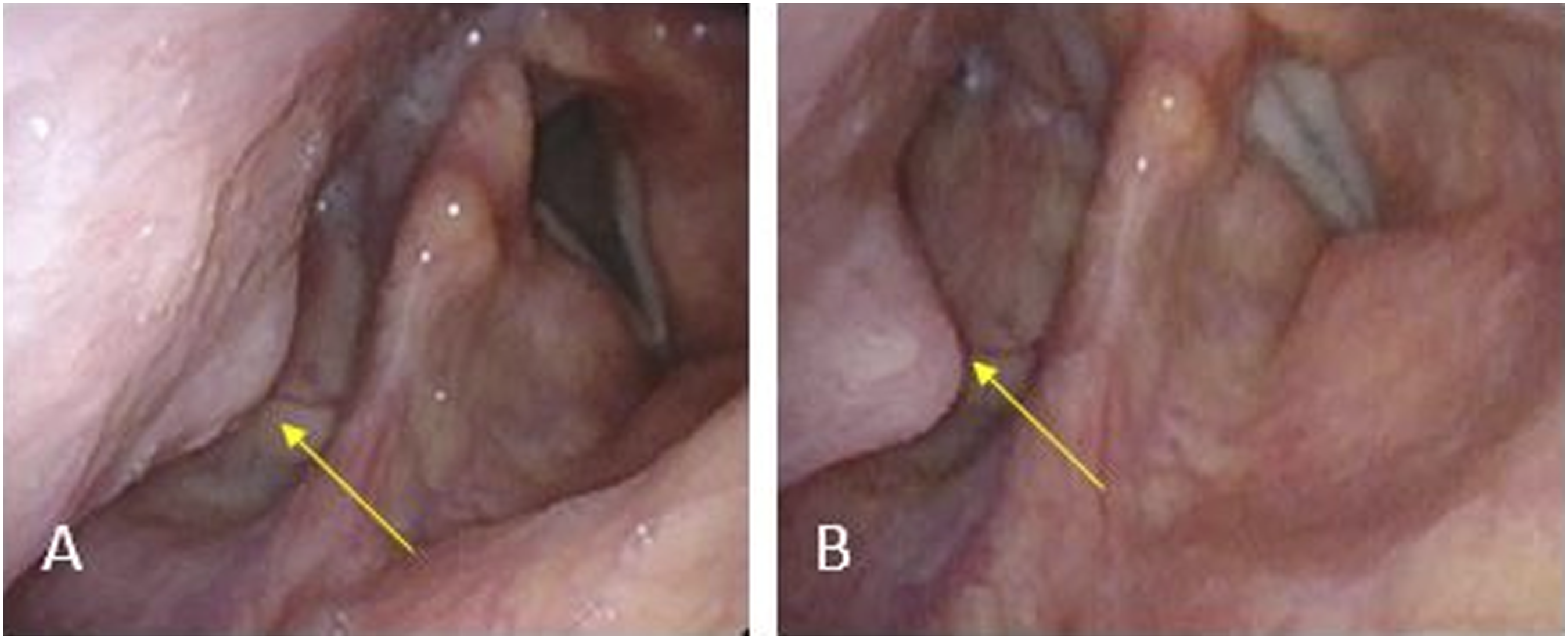
Only after a basic and a three-dimensional CT, we could unbelievably identify a fracture of the superior horn of the thyroid cartilage (Figure 2). CT-scan imaging. Both on the 3D reconstruction (A) and on the basal CT scans (B–C) a displacement of right great horn of the thyroid cartilage is evaluable.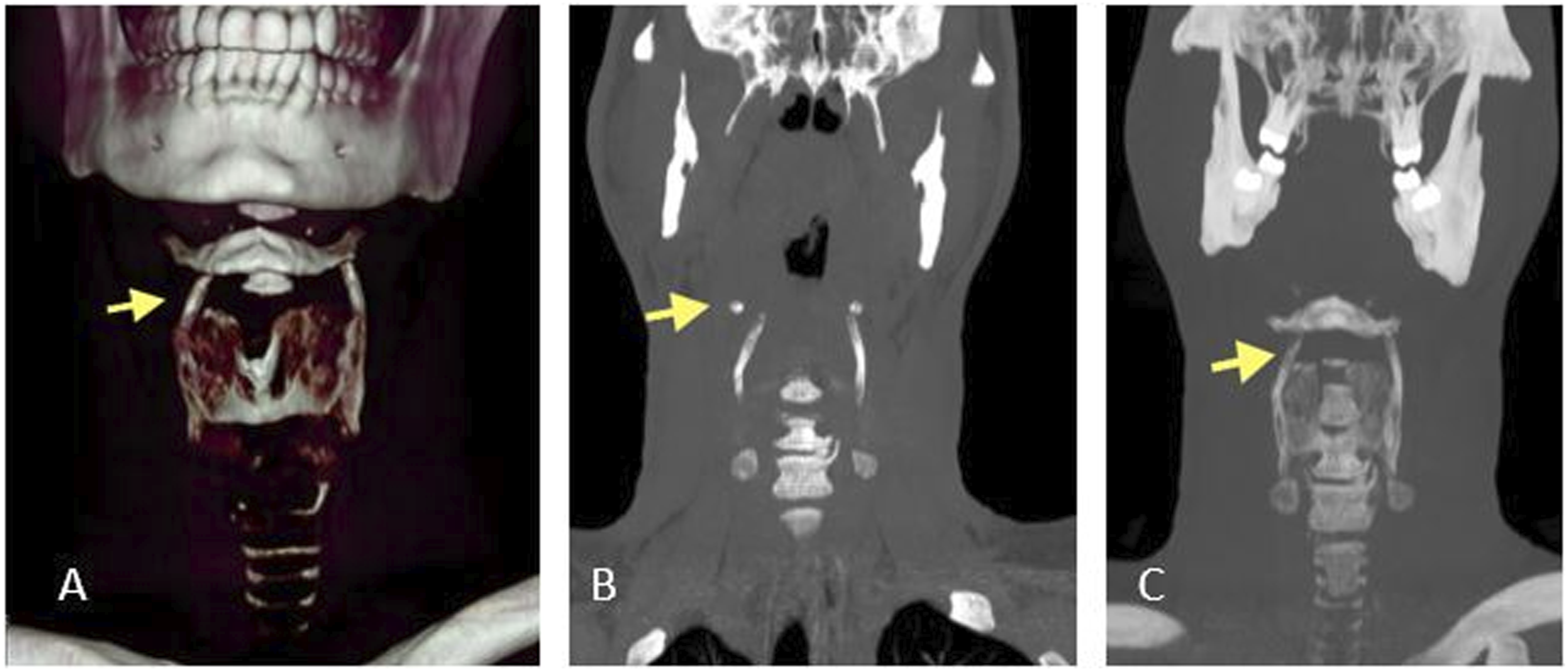
Laryngeal fracture is usually related to severe clinical cases and generally needs to surgical treatment to manage the upper airways, such as lateral cervicotomy and maybe tracheotomy. Our clinical case was mimicking only an occasional discomfort solved with some medical treatment, such as nonsteroidal antiinflammatory drugs, which is why we have proposed the “Watch and wait” follow-up strategy. If symptomatology worsened, we would propose to the patient an appropriate therapy.
Although a laryngeal fracture is rare in alive patients and when happens it must be managed in the emergency room, this case reported seems important to offer a possible differential diagnosis in patients who could show the same symptoms, if no other cause have been detected, like another one benign laryngeal disease.
Footnotes
Authors’ note
All the clinicopathologic investigations detailed in the manuscript have been conducted in accordance with the Declaration of Helsinki and its later amendments or comparable ethical standards.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent for publication of data and images was obtained from the patient.