
Abstract
Tracheal hemangioma is a very rare benign vascular tumor. Few cases of tracheal hemangioma in children are reported in the literature. Chronic cough is the main symptom of the disease; however, hemoptysis is rarely reported as a symptom of tracheal hemangioma in children. Here, we report a case of tracheal hemangioma in an eight-year-old girl admitted to our pediatric department for recurrent hemoptysis. Routine biological and radiological investigations were normal. Diagnosis was made using computed tomography and bronchoscopy. Beta-blocker therapy was not efficient. Bronchoscopic treatment by electrical excision enables complete recovery. Tracheal hemangioma should be considered a cause of recurrent hemoptysis when routine biological and radiological investigations are negative.
Introduction
Hemangioma are benign tumors that are frequently seen in children. They are generally found on the mucosal and skin surfaces. 1 The usual sites are the tongue, lips, nose, and oral cavity. 1 Primary tumors of the trachea are more frequently malignant in adults. 1 Tracheal hemangioma is a rare disease in adults and is exceptional in children. Chronic cough is the main symptom of the disease; however, hemoptysis is rarely reported as a symptom of tracheal hemangioma in children 2
We report here a case of tracheal hemangioma in an eight-year-old girl, to specify the signs of clinical orientation, the exploratory investigations to be requested, and the treatment of this pathology.
Case Presentation
An eight-year-old girl was admitted to our pediatric department for recurrent hemoptysis that evolved for a year. She mentioned that hemoptysis occurs after coughing and that a small amount of bleeding occurred whenever she had a respiratory infection. She had no medical history, such as trauma of the upper airways, tuberculosis, or recurrent lower respiratory tract infections. She had no other symptoms such as fever, weight loss, rash, chest pain, or dyspnea. The physical examination was without abnormalities. Hematologic parameters were as follows prothrombin time at 100%, activated thromboplastin time at 32/30, platelet count at 168x10³, and hemoglobin at 10.8 g/dL. The chest radiograph was without abnormalities. The intra-dermal tuberculin reaction and the spitting Lowenstein-Jensen cultures were negative. The chest CT showed a polypoid lesion on the right anterolateral wall of the proximal trachea. Bronchoscopy revealed a reddish polypoid lesion with a smooth surface attached to the tracheal wall with a short pedicle (Figure 1A). Two diagnoses were suspected: hemangioma or malignant process. Histological examination of the bronchoalveolar lavage did not find malignant cells. During the waiting period for drastic treatment, the patient received beta-blockers to stop bleeding, but she continued to have recurrent hemoptysis. The second bronchoscopy, performed 2 months after beta-blocker treatment, showed the same aspect of hemangioma (Figure 1B). The tumor was removed later by electrical excision with no complications. Histological examination revealed a benign vascular proliferation of 9 millimeters, made up of capillaries. So, the diagnosis of hemangioma was confirmed. At 24 months of follow-up, no hemoptysis episodes were observed and no bronchoscopic control was performed. (A): Tracheal polypoid lesion. (B): Appearance after 2 months of treatment with beta-blockers.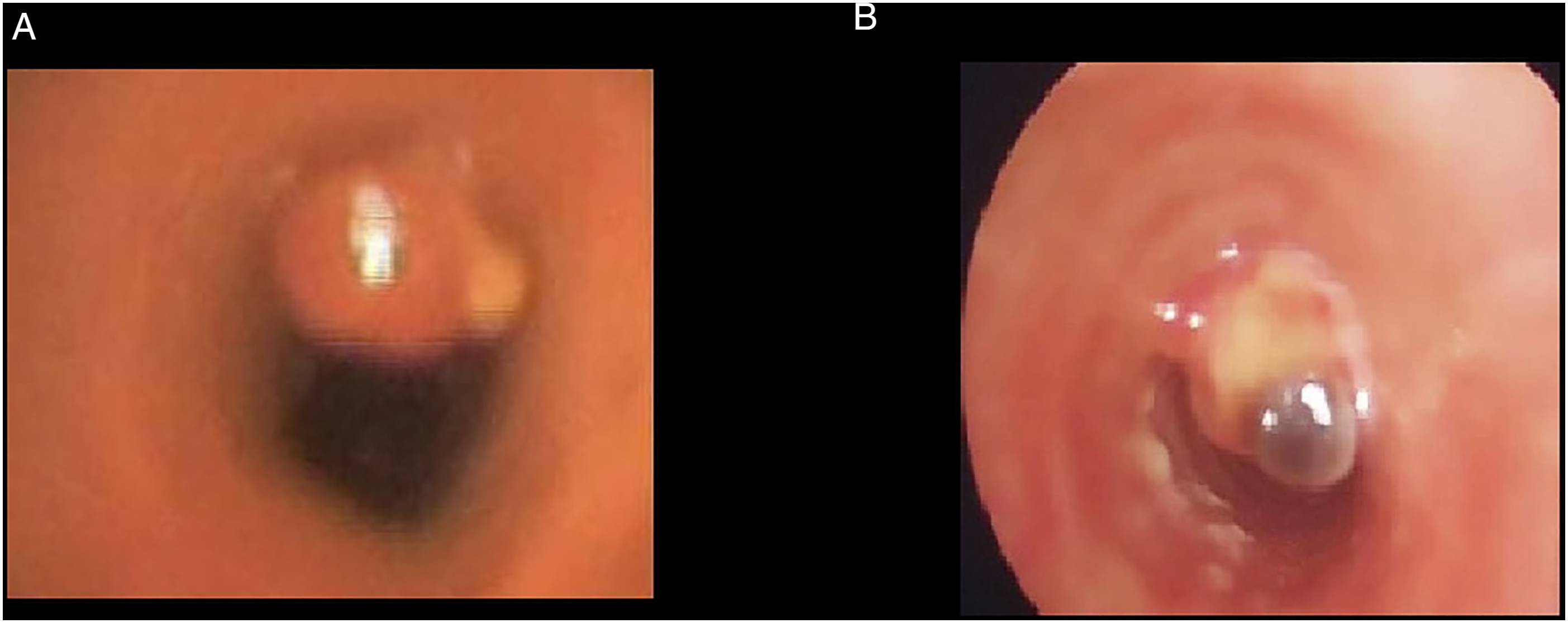
Discussion
Hemoptysis is a rare condition in children with a frequency of 0.35%. 3 Mean causes are lower pulmonary tract infections, tracheobronchitis, cystic fibrosis, tuberculosis, and foreign body aspiration. 4 Although hemoptysis is more common in adults, the principal etiology is tracheal neoplasms that occur in 25% of patients. 5 Certain drugs can cause this symptom, such as retinoid therapy. 6 However, hemoptysis is rarely associated with hemangioma in both children and adults; especially in the upper respiratory tract.
Few cases of tracheal hemangioma in children and adolescents have been reported in the literature. To our knowledge, only four cases have been reported until now. Recurrent cough and hemoptysis were the main symptoms that orient the diagnosis.2,7,8 The age of discovery was 10, 12, 14, and 17 years.2,7-9 Our patient was 8 years old. She is the youngest to present with tracheal hemangioma. One reason why symptoms (particularly hemoptysis and chronic cough) occur at that later age could be the poor potential of hemangioma growth in the tracheal localization. The explanation could be the low vascularization of the trachea. So, hemoptysis as a symptom of tracheal hemangioma can occur even in adult age.10-16 Small recurrent hemoptysis is more frequently reported in children, but massive hemorrhage can complicate tracheal hemangioma in adults.15,16
The chest radiograph is usually normal. Hemangioma is well diagnosed with thorax CT and bronchoscopy. The bronchoscopic appearance is not specific and mimics malignant tumors or other benign ones. Bronchoscopic biopsy and histological examination are the keys to a definitive diagnosis. The chest radiographic findings were perfectly normal in our patient, but she had a tracheal lesion on chest CT. Malignant causes were first eliminated by histological examination of the bronchoalveolar lavage in the initial bronchoscopy.
There is no standard treatment for these lesions. It depends on the age of discovery, comorbidities, the extent, and the size of the tumor. The use of propranolol has become an emerging treatment of hemangioma 17 however, it is mostly used for cutaneous, oral, and subglottic hemangioma 18 and could not be as successful on tracheal ones. Our patient was first treated for 2 months with a beta-blocker (Propranolol) due to the nonspecific appearance of the bronchoscopy and in order to avoid invasive treatment. But she continued to have bleeding and a bronchoscopic intervention was needed. Furthermore, the use of beta-blockers is well known in superficial sites, but none of the reported cases of tracheal hemangioma were treated with beta-blockers. So, it seems to be clear that beta-blockers are probably not the best way to treat tracheal hemangioma and delay radical treatment without any benefit.
The different bronchoscopic techniques reported in the literature were successful in the treatment of tracheal hemangioma.8,9 Our patient also did not show any complications and is currently symptom-free after 2 years of evolution.
Conclusions
Tracheal hemangioma is an extremely rare localization of hemangioma in adults and exceptional in children. Hemoptysis is a very rare symptom of the disease. Standard radiological findings may be normal; therefore, chest CT and bronchoscopy give the right diagnosis. These tumors can be successfully and safely treated with interventional bronchoscopic methods.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Research is approved by our hospital ethics committee. Oral consent has been provided from the parents of the child to publish the case anonymously.
Informed Consent
Informed consent was obtained from the parents.