
Abstract
It is very rare for extracranial carotid artery dissection to present as a carotid pseudoaneurysm. A delayed diagnosis and delayed treatment will lead to rupture of carotid pseudoaneurysm and massive hemorrhage and death. In this paper, we reviewed the progress of the disease in one patient and reviewed the relevant literature reports to understand the characteristics of the disease. The patient had two consultations within the otolaryngology department. The patient later showed signs of infection in the parapharyngeal space and then died of an aneurysmal rupture and massive hemorrhage.
Keywords
Introduction
Carotid artery dissection (CAD) is a condition in which the carotid artery is torn for various reasons, resulting in blood entering the vascular wall due to the arterial pressure. The intima is usually separated from the middle vascular layer along the direction of the blood flow. Subintimal separation can lead to lumen stenosis or even occlusion, resulting in cerebral ischemia. 1 The incidence of cerebrovascular events caused by carotid artery dissection is approximately 2.97/100,000 people/year, and the incidence of internal CAD is 1.21/100,000 people/year. 2 Carotid artery dissection may also present with subadventitial separation, which can lead to the appearance of a pseudoaneurysm. 1 Such patients do not have lumen stenosis and do not show symptoms of cerebral ischemia, which is more likely to delay the diagnosis and treatment. Carotid dissection can be divided into traumatic carotid dissection and spontaneous carotid dissection according to the etiology. Doctors pay more attention to vascular conditions in patients with a history of trauma, and these conditions are not prone to a missed diagnosis or a misdiagnosis. Spontaneous carotid dissection, especially pseudoaneurysm, is more prone to delayed diagnosis in clinical practice. We review a patient with a final presentation of parapharyngeal space infection.
The patient was admitted to the Department of Neurology due to suspected trigeminal neuralgia and had a consultation by the Department of Otorhinolaryngology to determine whether the patient had otogenic pain due to facial pain. After imaging examinations, a parapharyngeal space infection was considered, and the patient had another consultation with the department of Otorhinolaryngology. In this case, the patient had no obvious cranial nerve palsy or central nervous system defect at the onset, and the neurologist and otolaryngologist had insufficient understanding of the disease, which lead to delayed diagnosis.
Case report
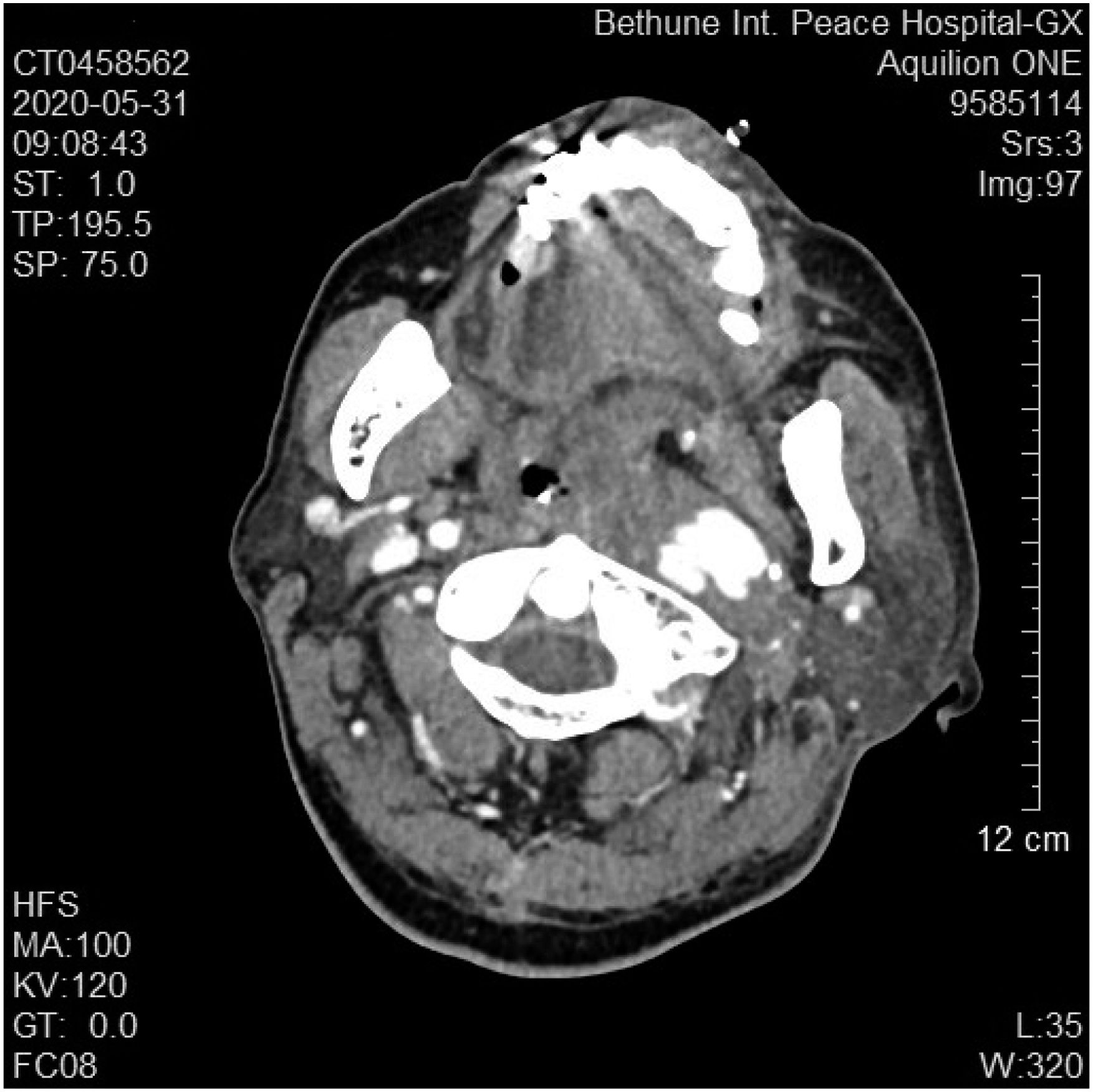
A 64-year-old male patient was admitted to the Department of Neurology due to “discontinuous left anterior auricular and facial pain for 10 days”. The pain began in front of the left ear and radiated toward the forehead and face. The pain was intermittent, and the patient had severe nausea and vomiting. Brain CT examination showed no positive findings. Admission examination: the patient’s vital signs were normal. Neurological tests showed no abnormalities. The diagnosis at admission included trigeminal neuralgia and the patient received oral carbamazepine, a routine admission examination, a trigeminal nerve magnetic resonance imaging (MRI) and a brain MRA examination. No abnormalities were found on the MRI examination. Routine blood examination included the following findings: the white blood cell count was 12.37 g/L (3.5-9.5 g/L), the absolute value of neutrophils was 8.60 g/L (1.8-6.3 g/L), and the erythrocyte sedimentation rate was 33 mm/within 1 hour (0-20 mm). On the third day of admission, the patient complained of having only a slight improvement in his facial pain. Physical examination showed that the diameter of the right pupil was 3 mm, and the diameter of the left pupil was 2.5 mm. A consultation with the department of otolaryngology showed that there was no herpes in the left external auditory canal and auricular cavity, and the tympanic membrane was intact. The patient’s facial expression was symmetrical, and the patient’s hearing examination was symmetrical. Therefore, Hunt syndrome was ruled out. On the sixth day, the patient developed a fever, and the patient’s body temperature was 37.6°C. Lumbar puncture was performed, and the results were normal. On day 10, the patient had a slight maxillofacial swelling, hoarseness, and intermittent coughing when drinking water and the tip of the patient’s tongue was noted to be tilting to the left when the patient extended his tongue out of his mouth. The facial pain was relieved, but the patient developed fever and chills reappeared. Magnetic resonance imaging examination revealed irregular cystic lesions in the left parapharyngeal space and extensive soft tissue edema in the left nasopharynx, oropharynx and lateral wall of the laryngeal pharynx. The left sternocleidomastoid muscle, parotid gland, posterior ear, and anterior neck had extensive soft tissue edema (see Figure 1). The next ENT consultation showed that the left tonsil was pushed to the midline, and the palatal and lingual arches were obviously raised. A parapharyngeal space infection was considered after evaluating the MRI findings. On the 11th day, an enhanced oropharyngeal CT examination was performed (Figure 2). Extensive space-occupying lesions were found in the left nasopharynx, oropharynx, left parapharyngeal soft tissue, space around the carotid sheath, posterior margin of the left sternocleidomastoid muscle, supravian fossa, and anterior neck. A soft tissue infection accompanied by abscess formation was considered to be highly likely. The cystic enhancement in the soft tissue of the left parapharynx was considered to possibly be a pseudoaneurysm of the internal carotid artery. After consulting with the vascular surgery department, their opinion was that the patient had a pseudoaneurysm formation of the left internal carotid artery, but because of the severe local infection, the stent implantation could not be completed. The patient continued to receive anti-infective therapy. On the night of the 13th day of admission, the patient suffered a sudden massive hematemesis, and his blood pressure dropped rapidly, which resulted in death. ■■■. ■■■.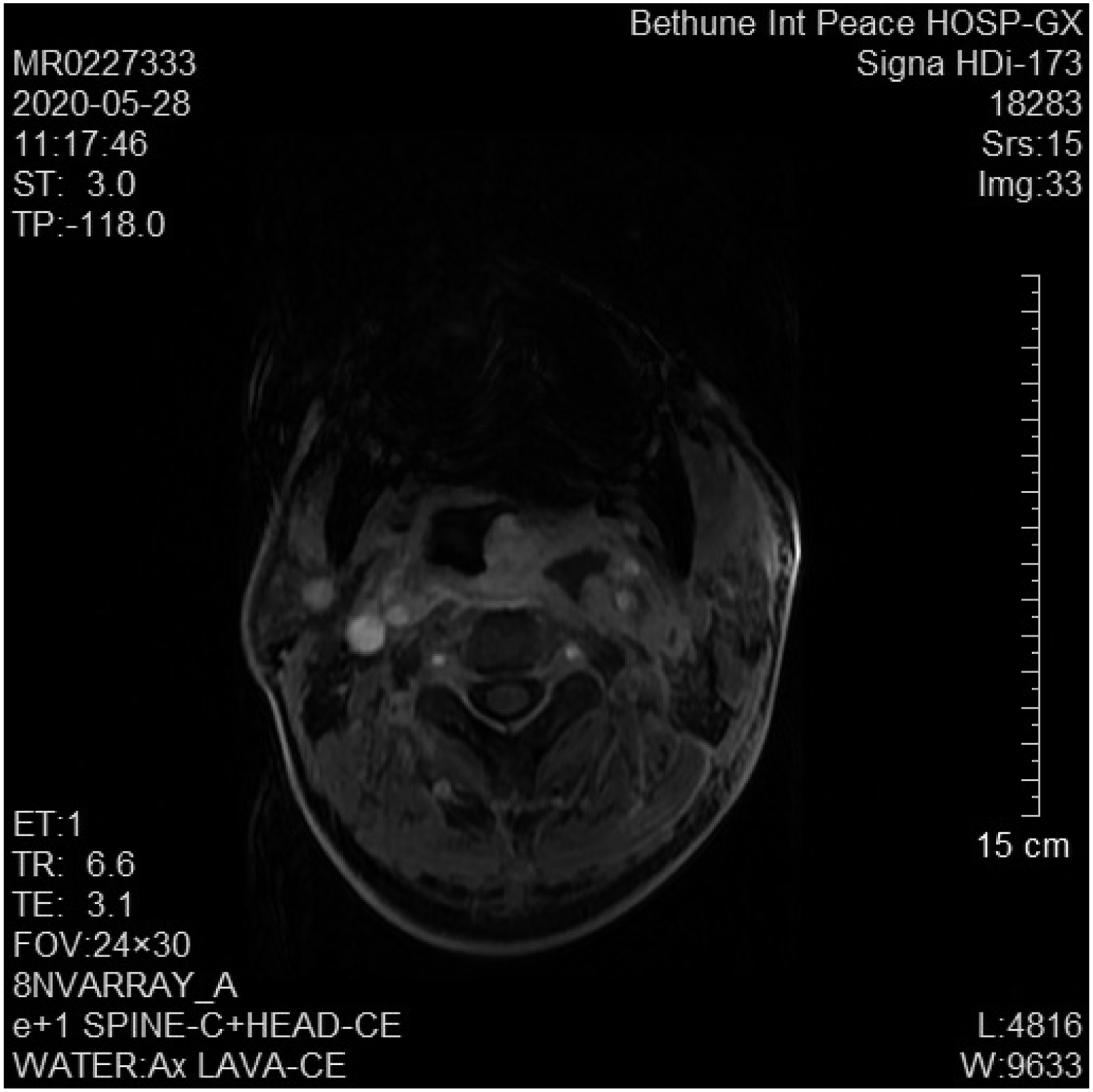
Discussion
Carotid artery dissection refers to the avulsion of the intima of blood vessels and the formation of an intramural hematoma when blood flows into the vascular wall. When the hematoma affects the intima and media, it can cause vascular stenosis. When blood flows below the adventitia, it can form an aneurysmal dilation, namely, a pseudoaneurysm. The patient was admitted with severe left facial pain for 10 days. We did not inquire about the characteristics of the patient’s pain in detail during the consultation, and the diagnosis was trigeminal neuralgia, which has a high incidence. Unfortunately, we neglected the most important information that the history inquiry can give us. There were some differences in the patient’s pain characteristics. Trigeminal neuralgia is associated with definite intervals, where the patient is affected, in between completely normal intervals. However, pain associated with CAD is persistent, intermittent, and aggravating. Headache and neck pain occur in 50%–80% of carotid dissection patients and may be the only warning or symptom of dissection.3-5 Therefore, a sudden unilateral, sharp headache or neck pain may signal the onset of arterial dissection. At this point, patients are likely to seek help from an otolaryngologist, so the otolaryngologists’ awareness of the disease is important. Routine blood results on the second day of admission showed a higher than normal number of white blood cells. Carotid dissection patients have been reported to have a higher white blood cell count than noncarotid dissection patients. 6 Leukocytosis may reflect a preexisting inflammatory state that is independent of potential factors, such as the patient’s body mass index, diabetes, smoking, or coronary heart disease, and that are associated with infections. 6 Recent infection is given priority over respiratory tract infection and has a significant relationship with CAD. 1 On high-resolution MRI of the neck, patients with spontaneous CAD often had arterial edema, and they can also have increased C-reactive protein or an increased erythrocyte sedimentation rate, which supports the hypothesis that inflammation plays a role in CAD but not in traumatic CAD. 7 The results of the routine blood tests on the day after admission showed that the patient had a higher than normal WBC count, which was considered a neuroinflammatory change, and antiviral therapy was given. The patient did not undergo a neck vascular imaging examination; thus, the opportunity for an early diagnosis was missed. On the third day of admission, the patient’s facial pain was relieved, and a physical examination showed that the pupil of the affected side was narrowed, which was due to Horner syndrome. It was considered that the laceration of the carotid dissection was enlarged and that the pressure in the carotid pseudoaneurysm was reduced, so the pain was relieved. Horner syndrome occurs when a pseudoaneurysm of the carotid artery becomes enlarged and compresses the cervical sympathetic ganglion. The clinical presentation of CAD is not specific, and the symptoms are typical of a triad: pain on one side of the head, face, or neck, incomplete Horner syndrome, and cerebral or retinal ischemia several hours to several days later. Clinically, less than 1/3 of CAD patients have the typical triad, and any 2 manifestations of the triad strongly suggest CAD. 8 The pathophysiological features of CAD are mainly intramural hematoma, where mural blood can accumulate under the outer membrane, which may lead to symptoms of local compression, 9 such as Horner syndrome, or in the case of arterial rupture, intracranial arterial rupture bleeding can cause subarachnoid hemorrhage. However, the patient in this case had a ruptured pseudoaneurysm of the internal carotid artery in the extracranial segment and had bleeding into the parapharyngeal space. The clinical signs were similar to a parapharyngeal space infection or a parapharyngeal abscess, as previously reported.10,11 The patients with this condition will develop fresh hemorrhage if the areas around the tonsils are punctured. 10 If incision and drainage is performed, fatal effects may occur. On the tenth day after admission, the symptoms and signs of a parapharyngeal space infection had appeared. A physical examination showed that the tonsil was pushed to the midline and that the palatal and lingual arches were obviously elevated. Magnetic resonance imaging examination showed manifestations of a parapharyngeal space soft tissue infection. A pseudoaneurysm rupture and bleeding into the parapharyngeal space were considered. A parapharyngeal space infection and an abscess around the tonsil, especially around the tonsil abscess, are common diseases in otorhinolaryngology, and incision and drainage are routine treatments. The space infection was suspected to be caused by the rupture and bleeding of the internal carotid aneurysm. If incision and drainage is performed, the pressure in the space will significantly decrease, resulting in massive internal carotid artery hemorrhage and death. Therefore, otolaryngologists should be careful in the treatment of such common diseases. Puncture must be carried out first. If the extracted fluid is bloody fluid, incision, and drainage must not be performed. At this stage of disease development, the patient died of pseudoaneurysm rupture and massive hemorrhage on the 13th day after admission due to the inability for the patient to have a mulched stent implantation.
Conclusions
The main clinical symptoms of CAD are head and neck pain, partial Horner's sign, pulsing tinnitus, and cranial nerve palsy. Clinicians must pay close attention to the changes in the symptoms and signs of patients. Patients suspected of CAD need to be repeatedly asked about their medical history, and relevant imaging examinations should be conducted. Regarding the diagnosis, the diagnostic gold standard for carotid artery injury is traditional digital subtraction angiography, and MRI/MR angiography (MRA) and computed tomography (CT)/CT angiography (CTA) are commonly used as alternatives. 12 In the two imaging modalities of CT and MRI, the results and radiological characteristics of CAD are highly consistent, and CT/CTA and MRI/MRA have the same information value for CAD detection. 12
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Self-funded project of key R&D plan in Hebei Province (No.182777203).
Data availability
The data that support the findings of this study are available from the corresponding author upon request.