
Abstract
Nasopharyngeal Hodgkin’s lymphoma is a rare disorder. We describe a case of a 24-year-old male with Hodgkin’s lymphoma (HL) primarily originating from the nasopharynx. He presented with symptoms including snoring and bilateral nasal congestion. After evaluation, endoscopic surgery was performed. Surprisingly, the pathological result proved to be classic HL. Postoperative MRI showed that the tumor was completely resected, and PET-CT was further examined. No lesions were found in other places. Shortly thereafter, the patient was transferred to the hematology department for chemotherapy, and the patient was followed up for 5 months without tumor recurrence. As new problems have been detected in medical management, it is vital to put the HL of the nasopharynx into a new perspective.
Introduction
Waldeyer’s ring (WR) is a common area of lymphoid involvement in non-Hodgkin lymphoma (NHL), particularly in adults. On the other hand, involvement of WR, especially the nasopharynx, in Hodgkin lymphoma (HL) is extremely rare and is reported almost exclusively in the adult population1,2. Although diagnostic approaches for determining WR involvement have evolved over time, a consensus for what constitutes involvement has not been formally established. Historically, diagnosis of WR involvement has been limited to direct observation through a physical exam or nasopharyngoscopy, with or without the use of biopsies. 3
Of note, biopsy results may yield false positives, and whether to operate directly is a matter for further discussion. While positron emission tomography-computed tomography (PET-CT) has gained in popularity, the timing of PET-CT needs to be further clarified. Preliminary exploration of the tumor microenvironment in the field of NHL has been done. In contrast, the tumor microenvironment of HL has not been studied in detail. Furthermore, it is not known whether there is an association between various lymphocyte-derived diseases. These issues will be discussed in this paper.
Here, we report a case of HL in the nasopharynx in a male patient who presented with a 5-year complaint of snoring and bilateral nasal congestion. Furthermore, we reviewed the literature to determine the incidence of HL in the nasopharynx, focusing on the tumor microenvironment, diagnostic approaches, PET-CT, and its association with Jessner lymphocytic infiltration of the skin (JLIS).
Case Report
A 24-year-old man presented to his primary care physician with a 5-year complaint of snoring and bilateral nasal congestion. The nasal congestion was constant. He also reported post-nasal drainage which was constant and present year-round. He denied any history of headaches, facial pressures, or rhinorrhea. Symptoms did not respond to allergy medications, antibiotics, or steroids. The patient had undergone excision of a facial mass in the dermatology department 4 years ago, and the post-surgical pathology showed JLIS. A physical examination revealed no evidence of cervical lymphadenopathy or other masses.
Routine hematologic testing was largely unremarkable. The values of neutrophils, lymphocytes, platelets, and monocytes were normal, and the neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), and lymphocyte to monocyte ratio (LMR) did not provide a clue as to the origin of the symptoms.
Next, a diagnostic nasal endoscopic examination was performed, demonstrating a large nasopharyngeal mass, occupying roughly 80% of the nasopharynx with near complete nasopharyngeal airway obstruction. The surface of the lesion was smooth. A contrast-enhanced magnetic resonance imaging (MRI) scan of the nasopharynx confirmed a nasopharyngeal mass with iso-intense signals on T1WI and T2WI and a clear boundary. The lesions showed a significantly homogenous enhancement (Figure 1). Preoperative MRI scan. Abnormal mass-like signal with clear borders was seen in the posterior wall of the nasopharyngeal apex, with a size of about 4.3cm×2.7cm×3.9 cm.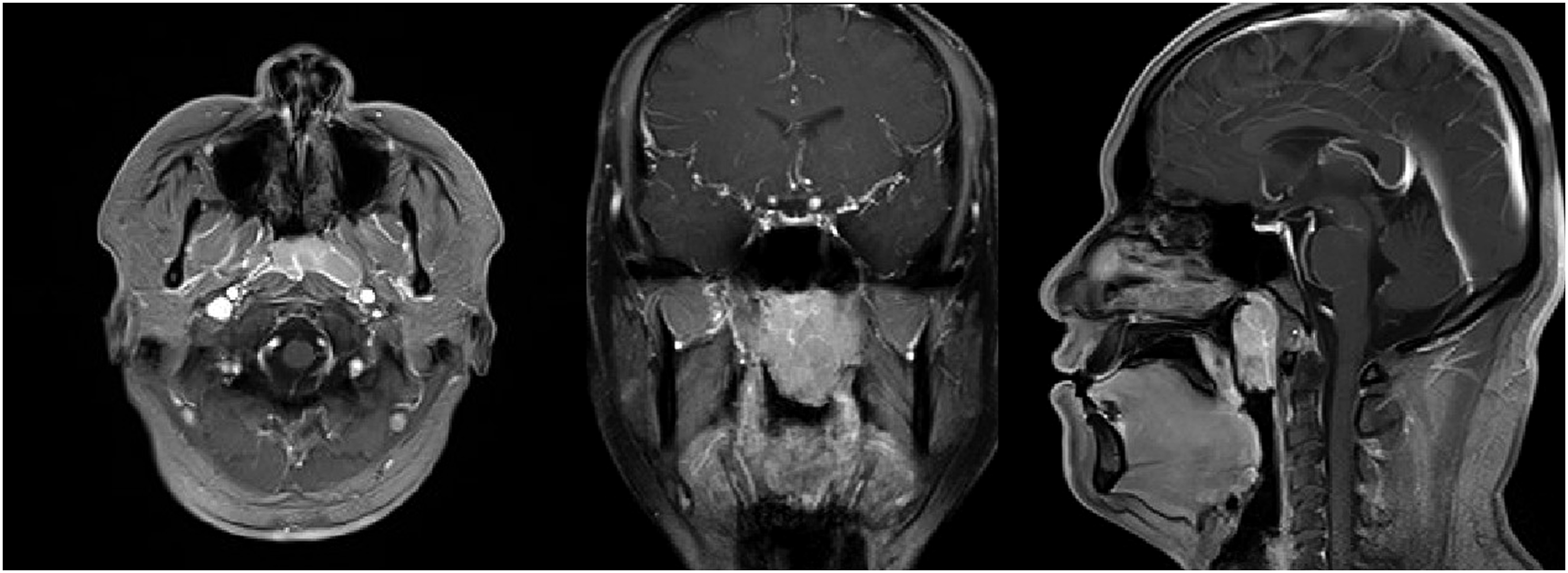
Since complete resection was easy to achieve and obtaining a whole specimen reduces the possibility of false negatives upon pathological examination, endoscopic surgery was performed. The entire mass was submitted to the pathology department for examination in a timely fashion. After 7 days, the immunohistochemical analysis showed diffuse growth of lymphoid tissue below the mucosa. There were distinct atypical mononucleated, binucleated, and multinucleated cells, many of which were characteristic of Reed-Sternberg (R-S) cells and Hodgkin cells (R-S variants) (Figure 2). Pathological findings. Mass revealed Hodgkin lymphoma, lymphocyte rich subtype (H&E ×400). Red squares point to Reed-Sternberg cells.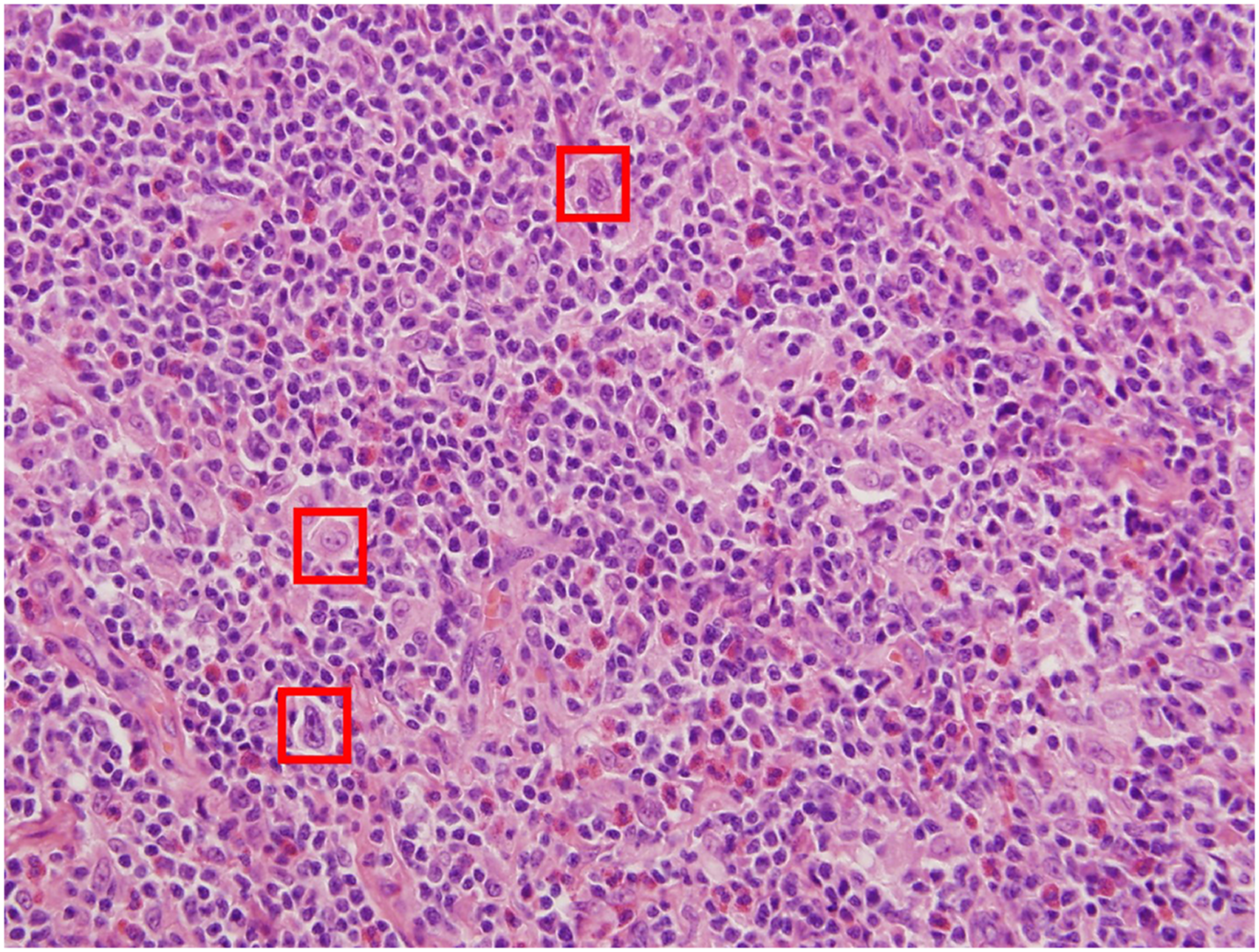
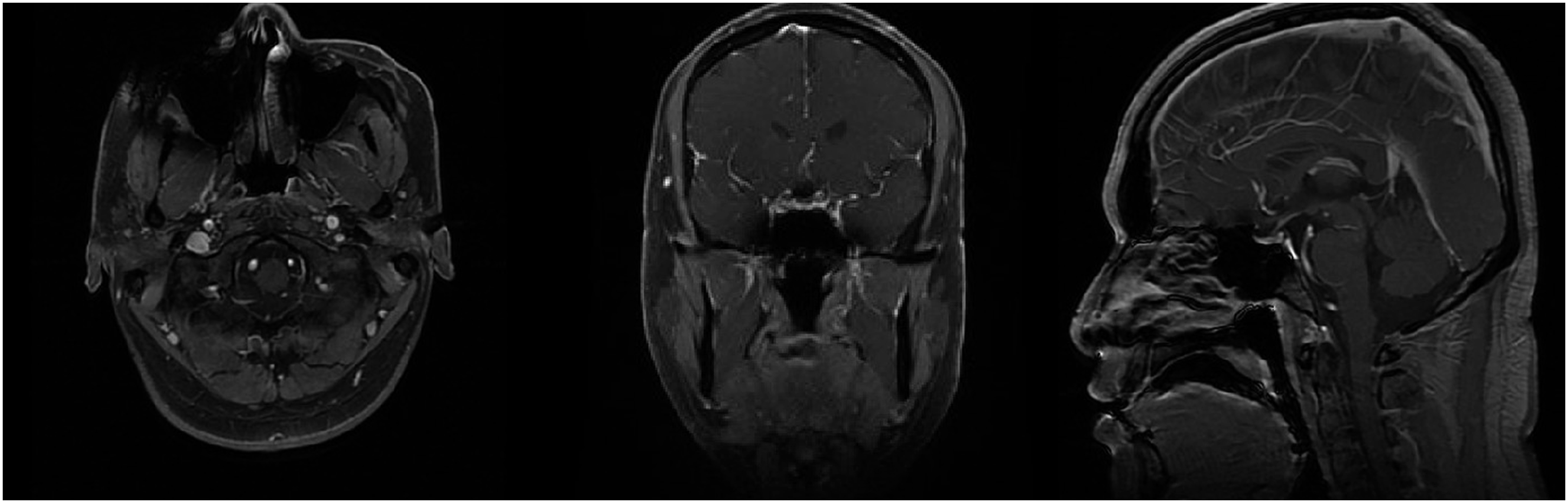
Subsequently, PET-CT was performed to assess the patient’s systemic tumor metastasis. PET-CT shows increased radiation uptake in the nasopharynx, especially in the parietal and left posterior wall, at a maximum standard uptake value (SUVmax) of 10.45. Delayed imaging displayed a slightly lower radiation uptake than before, with a SUVmax of 7.57, which was considered to be a postoperative change (Figure 3A). Postoperative MRI showed complete removal of the nasopharyngeal mass (Figure 4). The tumor was only involved at the primary site, without metastasis to other sites or to the lymph nodes as confirmed by whole-body PET-CT. The patient showed no symptoms of group B such as fever, night sweats, or weight loss. The patient was transferred to the hematology department for further treatment, and a bone marrow puncture was performed. No abnormalities were found, and the final diagnosis was typical HL stage IA, and a chemotherapy regimen including adriamycin, bleomycin, vinblastine, and dacarbazine (ABVD) was given. There was no obvious recurrence at the 6-month follow-up visit and the second PET-CT showed that the SUV values in the operative area and surrounding area had been reduced to a normal range (Figure 3B). PET-CT scan. The green circles point to areas of fluorodeoxyglucose avidity in the nasopharynx. Postoperative MRI scan. No clear abnormal signal was shown in the nasopharynx. The Rosenmullar fossa was slightly broaden on both sides, and linear enhancement was seen at the edge of the operated area.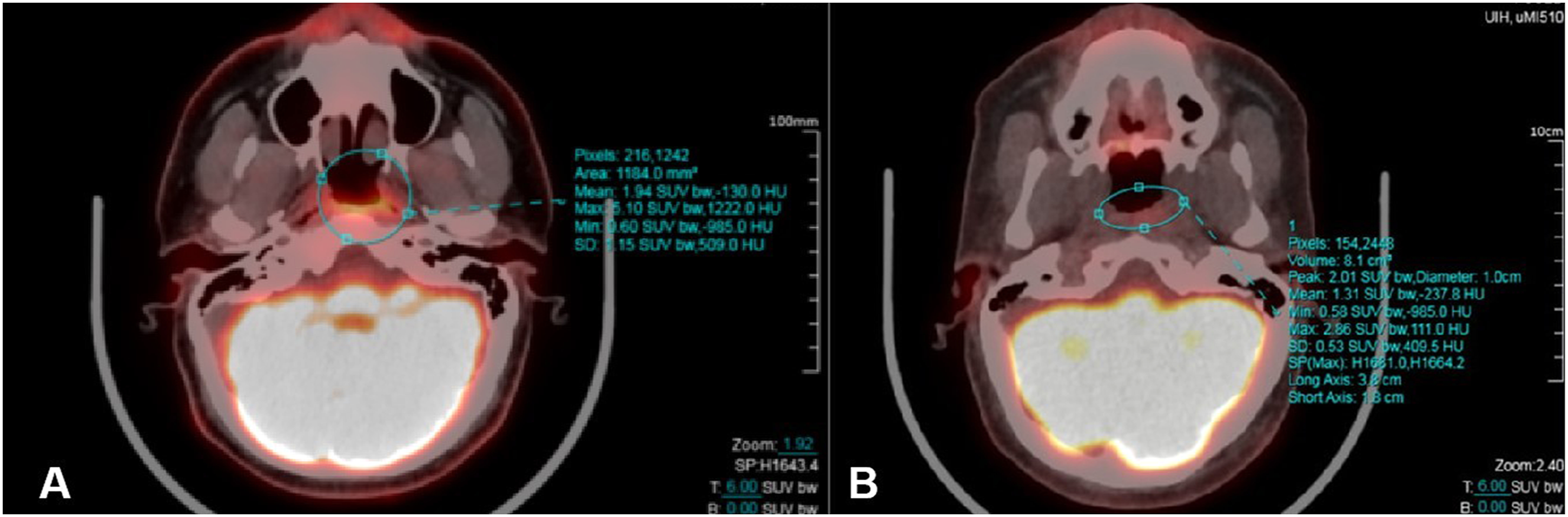
Discussion
The current work describes a rare case of HL originating from the nasopharynx. WR, also known as the pharyngeal lymphatic ring, consists of the bilateral palatine tonsils, adenoids, and lingual tonsils. It is the most common site of head and neck lymphoma. Previous studies have shown that 5% to 10% of all cases of NHL originate from the WR. 4 On the other hand, HL originating from the WR is very rare and HL of the nasopharynx accounts for only 0.32% of all cases of HL. 5 A literature review revealed less than 90 cases of HL involving the nasopharynx, and only about 20 cases of HL primarily originating in nasopharynx, indicating that some potential problems still require further research 6
Tumor Microenvironment and Blood Inflammatory Indicators of HL
Recently, the role of the tumor microenvironment in the development of lymphoma has received increasing attention. The development and progression of tumors, including lymphoma, is affected by their interaction with cells, chemokines, and adhesion molecules from the tumor microenvironment. Lymphoma–associated M2 macrophages are involved in the development of lymphoma by releasing cytokines and promoting angiogenesis and have been found to be associated with the prognosis of patients with follicular lymphoma. 7 Lymphoma evades the body’s anti-tumor immunity through regulatory T cells in the tumor microenvironment. 8 Lymphoma can also bind to T cells by expressing CD40, thereby promoting its spread and metastasis. 9 In addition, elevated levels of IL-2 receptors have been observed in the serum of patients with lymphoma, including a correlation between the levels of IL-2 receptors and the number of macrophages in the microenvironment, resulting in poor clinical outcomes in patients with lymphoma.
The relationship between peripheral inflammatory indicators, the tumor microenvironment, and nasopharyngeal lymphoma is not known. Nevertheless, a previous report 10 indicated that lymphocyte and monocyte counts could be independent prognostic factors of diffuse large B cell lymphoma (DLBCL). Although NLR and PLR are progression and prognostic markers for various solid tumors, there are few literature reports related to their possible role in lymphoma. In recent years, it has been reported that NLR and LMR have prognostic value in DLBCL patients. 11 In DLBCL, decreased lymphocyte counts were reported in relapsed patients treated with autologous peripheral blood hematopoietic stem cell transplantation,12, 11 which suggested that peripheral blood inflammation indicators not only play a predictive role before treatment, but also play a predictive role during the follow-up process. For extranodal natural killer/T-cell lymphoma (ENKTCL) originating in the head and neck, 13 ,11 low LMR indicates poor prognosis and can be used as an independent risk factor, which is consistent with the large number of CD68+ mononuclear macrophages that were found to have infiltrated the ENKTCL microenvironment. 14 In the future, the predictive ability of such indicators is expected to improve by combining them with the prognostic indicators commonly used in lymphoma. For example, the lactate dehydrogenase-lymphocyte ratio has been found to be significantly correlated with the overall survival (OS) of lymphoma patients. Meanwhile, the relationship between neutrophils, lymphocytes, NLR, LMR, PLR, and nasopharyngeal Hodgkin's lymphoma needs further exploration.
Surgery or Biopsy
Pathology is still the gold standard for HL diagnosis. However, whether to obtain the pathological specimen during surgery or via biopsy remains a problem that clinicians face. In a previous report, only 7 pathology samples were obtained during surgery, while the rest were obtained through biopsies. 15 Biopsies have the advantage of being less invasive and less risky, but they are also associated with false negatives. Biorklund et al. 16 described 45 adult HL patients who were examined in detail by otolaryngologists, followed by biopsy. Only 7 patients displayed nasopharyngeal abnormalities during endoscopic examination, while most patients did not show any abnormalities. This led to the recommendation to diagnose HL by extended biopsy, due to the number of false negative in nasopharyngeal biopsy. Oluwasanmi et al. 17 reviewed the pathology of 87 cases of tonsillectomy due to clinical tonsillectomy asymmetry without radiographic or other signs or symptoms of malignancy. Only 2 malignant tumors (1 HL and 1 NHL) were found among these 87 patients (2.3%). These studies emphasize that physical examination, direct endoscopy, or local biopsy are not reliable indicators in the absence of imaging.
The advantage of surgery is that it can completely remove individual lesions and obtain more accurate pathological results, but the disadvantage is that it is highly traumatic and has high risk. In most previous cases, the reasons to obtain a biopsy include the prediction of possible lymphoma, the presence of multiple lesions and surgical trauma, or the involvement of important neurovascular lesions and the difficulty of surgery. However, in the case reported in this paper, the clinician found that the isolated mass had a clear boundary and superficial location based on MRI, and no other lesions were found. The preoperative ultrasound results of the systemic lymph nodes showed no abnormalities so benign lesions were considered. In order to rapidly resolve the patient’s symptoms, a complete surgical resection was performed. Hence, it remains up to the clinician to balance the pros and cons of obtaining specimens during surgery vs biopsy.
Proper Time of Applying PET-CT
For otolaryngologists, clinical evaluations, including physical examination and nasopharyngoscopy, are usually performed to evaluate a nasopharyngeal mass. Nevertheless, it is difficult to differentiate malignant from benign masses in the case of a nodular mass with a smooth surface like the one reported here. Hence, clinicians should come to a diagnosis by combined methods to avoid subjectivity. Enhanced CT or MRI is usually recommended for the diagnosis and treatment of patients with nasopharyngeal masses. The use of physical examination or CT/MRI alone, without the use of PET-CT for metabolic assessment, may lead to a false-positive diagnosis of involvement of these regions in pediatric patients. When PET-CT and CT/MRI are used together, the anatomical and metabolic activity of WR can be assessed while minimizing the risk of false positives.18,19 During the initial staging of HL in the adult population, Hutchings et al. 20 found that, compared to enhancement scans alone, PET-CT had a significant sensitivity advantage. This was particularly evident in the extra-nodal region, where PET-CT showed a sensitivity of 86% compared to 37% for enhancement CT only. As a matter of fact, PET-CT is relatively expensive and is generally not used in clinical practice without clear evidence of suspected metastasis. A review of the literature showed that only 5 articles performed PET-CT evaluation of HL involving WR. 21 In our work, PET-CT was performed following pathological examination. Hence, our team believes that enhanced CT or MRI, combined with ultrasound examination of systemic lymph nodes can be carried out first. Biopsy or surgery should be performed after CT/MRI abnormality while PET-CT examination can be performed after pathologic findings.
Effects of Jessner Lymphocytic Infiltration of the Skin
JLIS 22 is a rare, benign skin disorder characterized by asymptomatic, erythematous popular rash, or plaque-like eruptions. These eruptions, usually located on the face and trunk, have an indolent course before resolving spontaneously or with medical treatment. Lesions can be solitary or numerous and recurrence is frequent, whether at the original site or previously unaffected areas. The cause of this disorder remains unknown, and there is still debate about whether this disease is a unique entity or part of a spectrum of cutaneous disorders. The case in this article shows a possible link between HL and JLIS, which may indicate a potential common mechanism for two kinds of diseases.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Funding source for the study: National Natural Science Foundation of China (Grant No. 81670904).
Data Availability
The data used to support the findings of this study are available from the corresponding author upon request.