
Abstract
We describe a case of nasal non-Hodgkin’s lymphoma in a 79-year-old Chinese patient accompany with nasal myiasis. The first 2 biopsies in this case were false negative. Subsequently, nasal maggots developed in this patient. After removing all maggots under nasal endoscopy, the patient continued to have recurrent fever and was transferred to a higher hospital for further treatment, in which he received a third biopsy. Unfortunately, several hours after the biopsy, the patient died for severe nasal bleeding. The final biopsy result indicated the neoplasm of the left nasal cavity was non-Hodgkin’s lymphoma. This case illustrates the importance of repeated biopsies for nasal non-Hodgkin’s lymphoma if necessary. Nasal myiasis is a secondary disease of nasal non-Hodgkin’s lymphoma in this case.
Background
Lymphoma is a malignant tumor of the immune system. Lymphoma arises from lymph nodes and lymphoid tissues, and its occurrence is mostly related to some malignant transformation of immune cells generated by the proliferation and differentiation of lymphocytes in the immune response process. Lymphoma is divided into Hodgkin’s lymphoma (HL) and non-Hodgkin’s lymphoma (NHL) based on histopathological characteristics. Non-Hodgkin’s lymphoma occurs in the extranodal tissues mainly, and NHL accounts for about 3% of all cancer cases in the population. 1 The head and neck region is the second common site for primary extranodal lymphoma after the gastrointestinal tract. 2
Thereinto, nasal NHL also belongs to primary extranodal lymphoma. 3 The incidence of nasal NHL accounts for 23% to 31% of nasal malignancy in Asia, 4 and it has high degree of malignancy. 5 Nasal NHL is divided into 3 subtypes according to immunohistochemistry, which include diffuse large B-cell lymphoma, peripheral T-cell lymphoma, and NK(Natural Killer )/T-cell lymphoma. NK/T cells are the most common source of nasal NHL in China, which accounts for more than 90%. 6
Nasal NK/T-cell lymphoma is common in Asia, Spain, and South America, especially in China, but it is rare elsewhere. 7 -9 Although the prevalence is not low in the above areas, we still can find some literatures 10,11 that report that nasal NK/T-cell lymphoma is difficult to diagnose at the early stage, or even misdiagnose this disease due to its nonspecific clinical manifestations. The clinical manifestations of this disease can be divided into 3 phases. Patients with nasal NHL present with a common cold or nasosinusitis with intermittent nasal obstruction and watery or bloody secretions in prodromal stage. In the active phase, nasal obstruction is aggravated in these patients, and nasal mucosa swelling, purulent and smelly nasal discharge, granuloma, erosion, ulceration, necrosis, nasal septum, or palate perforation also can be found in the nasal cavity, while the general condition is not too bad. In the terminal stage, the mucosa, cartilage, bone of the midline in the nasal cavity, and the adjacent tissues are damaged severely, which leads to local disfiguration, cachexia, and systemic failure. Indeed, the nonspecific inflammation and necrosis of nasal tissues contribute to the difficulty of early diagnosis of nasal NHL. Now, we present a case of nasal NHL accompany with nasal myiasis, which fails to make an accurate diagnosis in early stage.
Case Report
A 79-year-old man presented to the outpatient department of Otolaryngology in Luoding People’s Hospital in September 2020 complaining of persistent nasal obstruction, purulent discharge, and weight loss for about 6 months. We found much purulent and bloody secretions and a gray-red neoplasm which was anabrotic on the surface and easy to bleed when being touched in the left nasal cavity by endoscopy. The mucosa of the nasopharynx was smooth in this patient (Figure 1). And then nasal and sinus computed tomography (CT) scan and biopsy were carried on this patient. Computed tomography showed a slight thickening of the left nasopharyngeal wall, and unknown dense shadow in the left nasal cavity, and bilateral nasosinusitis (Figure 2). The subsequent biopsy result suggested that the specimen was a small amount of necrotic tissue. After anti-infective therapy of 9 days in the outpatient department, the patient still showed no improvement and then was hospitalized in the Department of Otolaryngology in Luoding People’s Hospital.
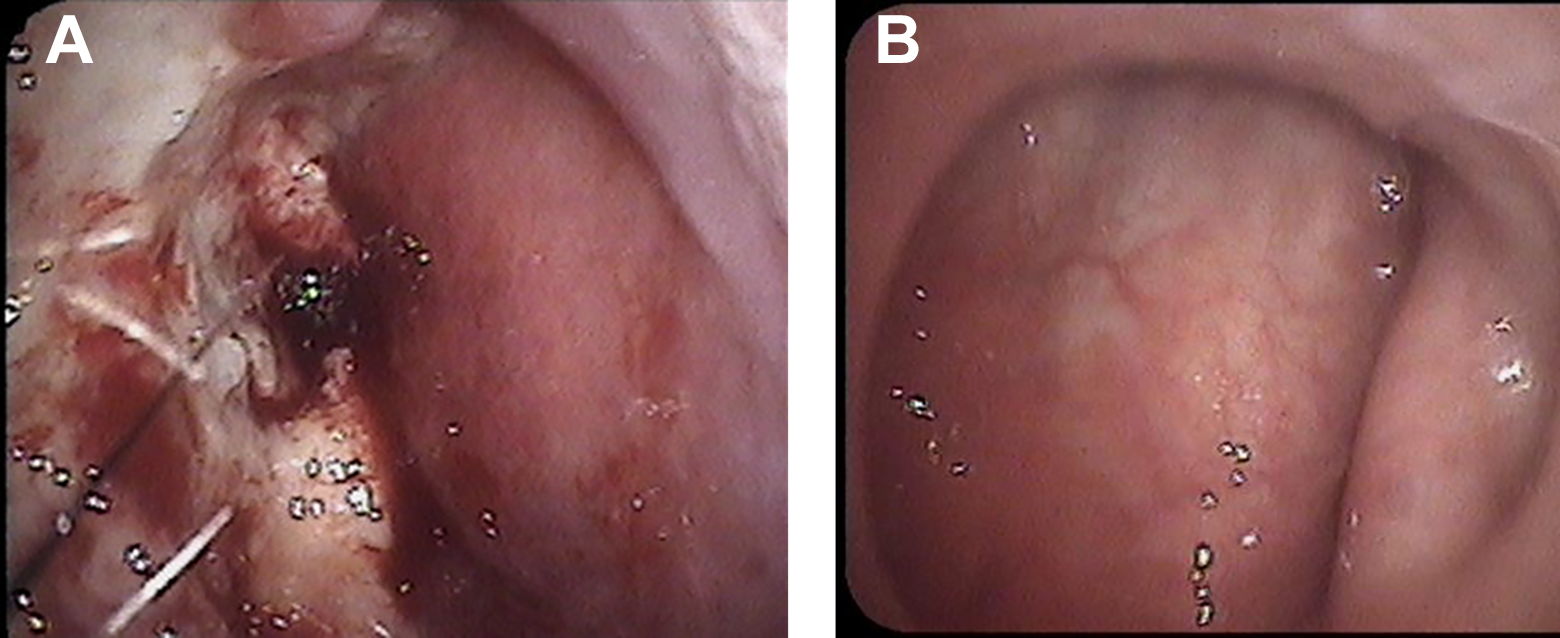
(A) A gray-red neoplasm that was anabrotic on the surface and easy to bleed when being touched in the left nasal cavity. (B) The mucosa of nasopharynx was smooth.
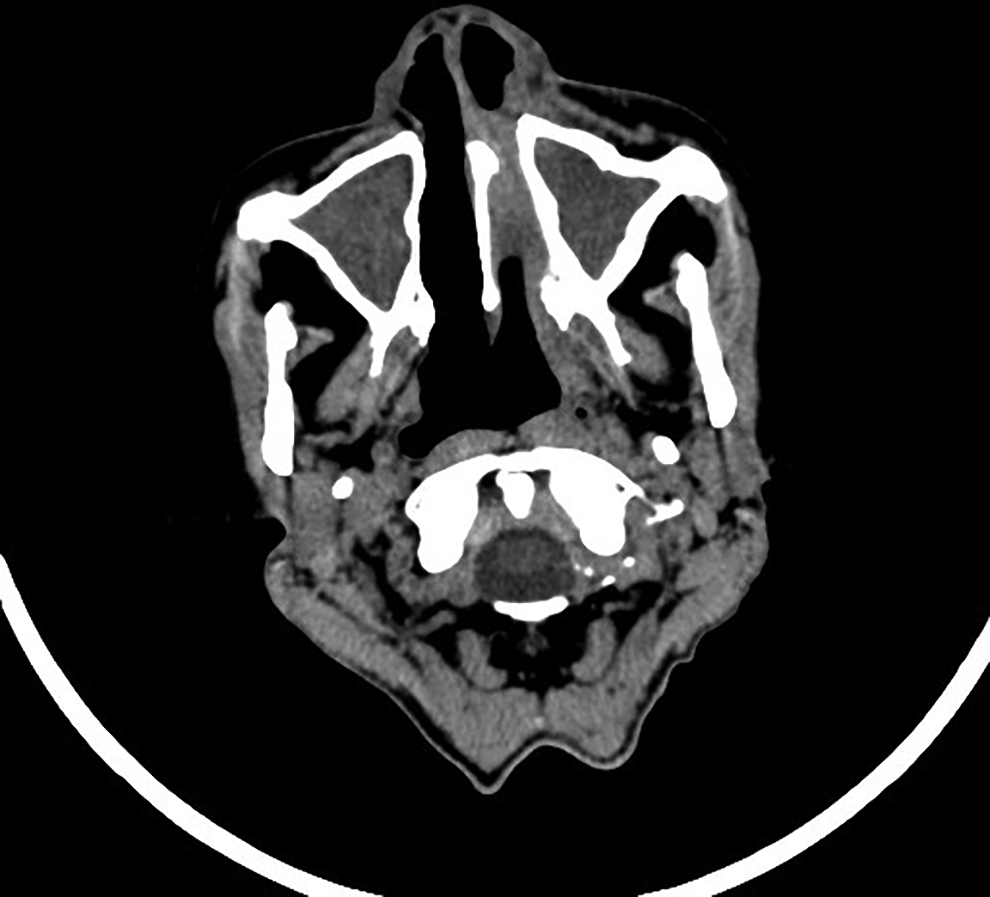
Slight thickening of the left nasopharyngeal wall, and unknown dense shadow in the left nasal cavity, and bilateral nasosinusitis.
Physical examination showed no significant lymphadenectasis in the whole body. Chest CT scan and ultrasound of heart and abdomen also showed no significant lymphadenectasis. HIV test showed negative. And Enterobacter cloacae was found in the left nasal cavity. Bilateral sinus opening operation under nasal endoscope was performed in this patient after the contraindications to surgery were excluded. During the operation, we performed a biopsy of the neoplasm deeply in the left nasal cavity again. But the pathological examination result showed necrotic tissues once again. After anti-infective therapy and intravenous dripping of glucocorticoids for 3 days, this patient was discharged after improvement of nasal obstruction, but the symptoms of bloody and purulent rhinorrhea could not be alleviated very well. Postoperatively, the patient returned to the hospital regularly for nasal endoscopy examination and regular medication that included oral antibiotic, prednisone, eucalyptol enteric-coated tablets, and intranasal glucocorticoid.
About one month after surgery, this patient came to our hospital for reexamination due to high fever. By nasal endoscopy examination, the patient presented with a nasal myiasis infestation (Figure 3) and was immediately hospitalized again. The removal of crawling maggots was performed with the help of forceps under nasal endoscopy. More than 100 larvae were withdrawn. And another bacteria Escherichia coli was found in the left nasal cavity. The level of LDH(lactate dehydrogenase) was 440 U/L, while the normal level was 114 to 240 U/L. Systemic treatment using intravenous dripping ceftriaxone (1000 mg bid), metronidazole(0.5 g every 8 hours) and defervescence drugs for 10 days was also performed. Whereafter, the nasal myiasis infestation was completely resolved. However, the patient continued to have recurrent fever. Subsequently, the patient was transferred to Guangdong Provincial People’s Hospital for further treatment and received a third biopsy of the left nasal mucosa. About 2 hours after the biopsy, the patient had severe nasal bleeding and cardiac and respiratory arrest. Although active rescue treatments were performed, this patient still died on the day. The subsequent biopsy result showed the neoplasm of the left nasal cavity was NHL (Figure 4).
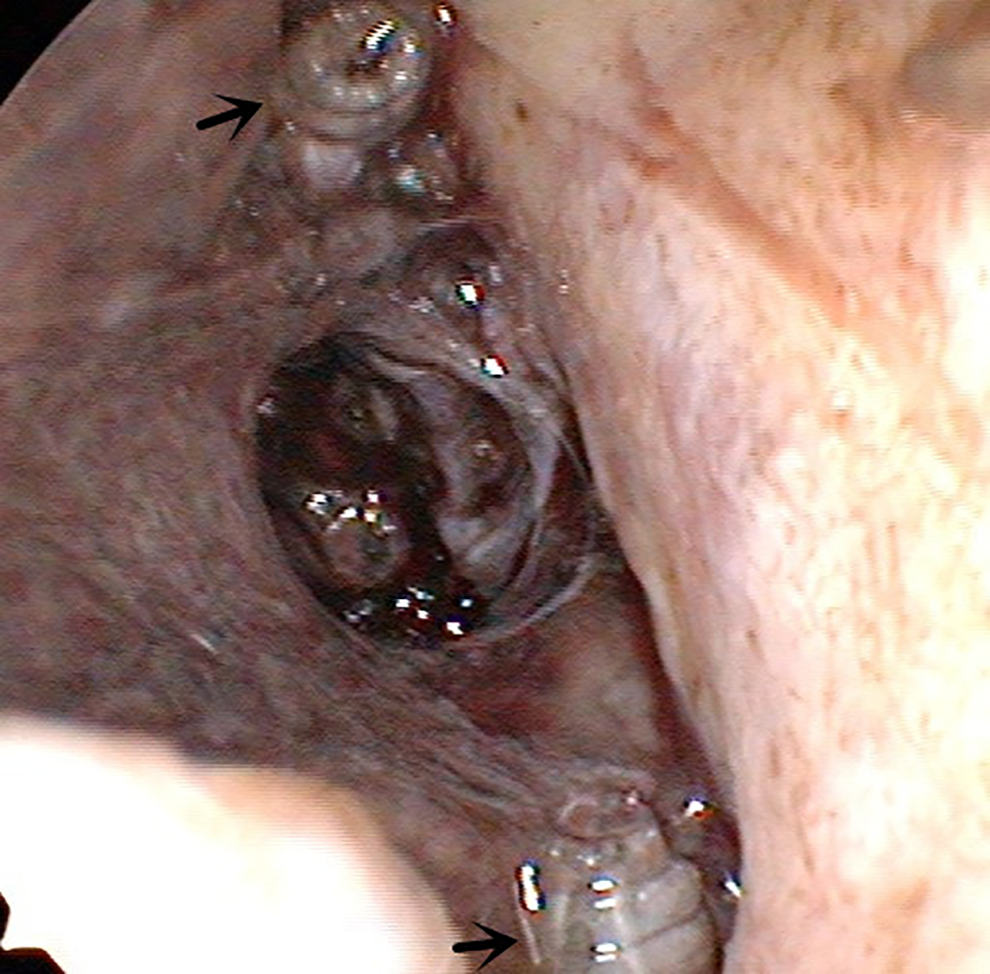
The black arrow showed the maggots in the left nasal cavity.
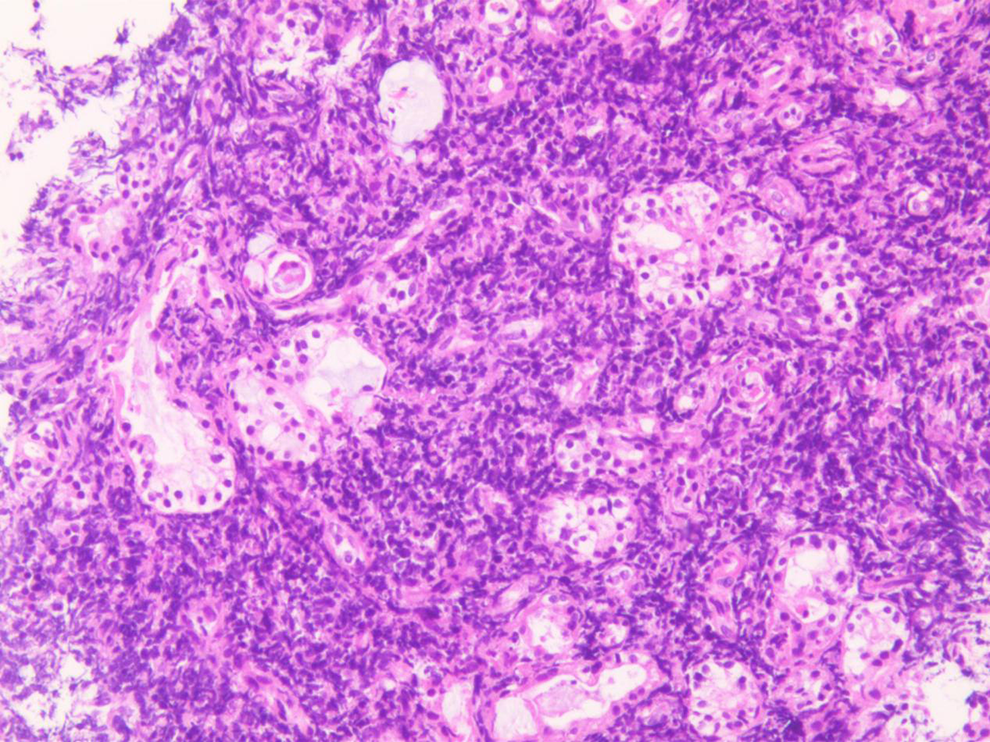
Large necrosis was observed in this neoplasm tissue. A few lymphocytes were observed locally, of which morphology was relatively simple. The chromatin of lymphocytes was deeply stained, while the nucleoli were not obvious, and the cytoplasm was small. The pathological diagnosis was considered as non-Hodgkin’s lymphoma of the left nasal cavity.
Discussion
Myiasis is a disease caused by fly larvae (maggots) parasitic on human and vertebrate host tissues or organs, which usually occurs in areas with poor sanitary conditions. 12 The common infection locations of myiasis include eye, ear, nose, vagina, urethra, colon, and so on. Although the distribution of this disease is worldwide, 13,14 nasal myiasis is rare in our country, 12 not to mention nasal NHL accompany with nasal myiasis. Nasal myiasis is not difficult to diagnose, and the basis of diagnosis is that the maggots are found in the nasal cavity or nasopharynx. The signs and symptoms of nasal myiasis include nasal and/or facial pain, bloody or mucopurulent nasal secretion, epistaxis, foul smell, and anosmia, which are usually related to the presence and movement of the larvae. 13,15 The surfaces of maggots carry some bacteria that may cause nasal and nasopharynx infection. The nasal cavity is close to the sinuses, eyeballs, meninges, and skull. Once the fly maggots migrate into and invade these position, they may lead to serious consequences such as purulent meningitis, even death. 16 Endoscopic removing maggots, nasal irrigation, anti-infective therapy, and the treatment of the primary disease are the main treatments for nasal myiasis. It’s reported that the risk factors of myiasis are open wounds, scabs, suppurative lesions, and ulcers contaminated with secretions and bloody remnants. 17 In this case, we suppose the nasal smelly secretions, which exist in this patient with nasal NHL, attract flies to drill into nasal cavity and lay eggs, and then lead to larva accidental parasitism. We can find other nasal myiasis cases with other primary diseases. 15,17,18 Therefore, chronic wasting diseases may be important risk factors for nasal myiasis.
The staging of HL and NHL (Ann Arbor Classification) are as follows. Stage I includes one node (I) or single extranodal lesion without nodal involvement (IE). Stage II includes 2 or more nodal groups on the same side of the diaphragm (II), or single extranodal lesion with adjacent nodes involvement, with or without other nodal groups on the same side of the diaphragm involvement (IIE). Stage III includes nodes groups on both sides of the diaphragm (III), or with limited related extranodal lesions involvement (IIIE), or with spleen involvement (IIIS), or with both involvements (IIIE+S). Stage IV includes diffuse extranodal lesion involvement, with or without lymphadenectasis, or single extranodal lesion involvement with distant lymphadenectasis. 19,20 According to this staging classification, this case that we report belongs to the stage IE. Although the stage IE of NHL usually has a bad prognosis, it’s reported that the median survival for the stage IE of this disease is 7 years and 9 months after active treatments. 21 However, this patient died for massive nasal bleeding about only 8 months after the onset, which was significantly lower than that of above.
One reason also the most important reason is that we fail to make an accurate diagnosis in the early stage of this disease, which results in failure to receive the appropriate treatment in time such as combination chemotherapy, and so on. It’s reported to be a diagnostic challenge for extranodal NK/T cell lymphoma. 22 Although we perform 2 biopsies in the first treatment hospital, we both get 2 negative false results. Too much necrotic tissues in this patient of nasal NHL lead to the failure of biopsies. Biopsy in non-necrotic areas after adequately removing necrotic tissue is vital to improve the diagnostic efficiency of nasal NHL. Nasal NHL cells are deemed to infiltrate along the walls of blood vessels, 23 which might be a potential cause of massive nasal bleeding afterward. And the concomitant nasal myiasis not only confuses the diagnosis but also aggravates the inflammation of nasal cavity and nasopharynx. Two different bacterial infections have been found successively in the nasal cavity of this patient. Maggots might be the intermediate host of these bacteria. As it’s mentioned in other case report, myiasis patients have bacterial infection. 24 Maggots could eat and damage tissues of nasal cavity during parasitism, which might be another reason for massive nasal bleeding of this patient.
Another reason is probably that the Ann Arbor classification system is less accurate in predicting the prognosis of patients with aggressive NHL. 25 International Prognostic Index (IPI) seems to be more suitable for identification, which is based on age, tumor stage, serum LDH level, performance status, and the number of extranodal lesions sites. The IPI identifies 4 risk groups with predicting 5-year survival rates of 73%, 51%, 43%, and 26%. 25 In this case, the patients is older than 60 years, and the serum LDH level is 1.2 times more than normal, and the performance status is classified as 2, and he has B symptoms that include temperature >38.3 °C and the loss of more than 10% of body weight recently. The IPI of this patient is 3, which is considered as a high-medium risk. It indicates this patient has a bad prognosis.
Conclusion
Any nasal inflammation of unknown etiology, especially with nasal mucosa necrosis, should not be ignored the possibility of nasal NHL. It’s very necessary to repeated biopsies for accurate diagnosis. Specific infections such as nasal myiasis might occur on basis of nasal NHL.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.