
Abstract

Significance statement
Juvenile xanthogranuloma (JXG) is a spontaneously regressing, rare, and benign lesion. 1 JXG occurs most often in infants and children, especially during the first year of life. 2 It is the most common type of non-Langerhans cell histiocytosis. 2 It appears mainly on the skin of the head, or trunk, without the involvement of major organs. 3 JXG of the auricle is an uncommon but a rapidly growing lesion. Here, we report a case of JXG affecting the auricle.
Case presentation
A 9-year-old female patient presented with a tumor in the left auricle that was detected 1 month ago. Otoscopy revealed a normal external auditory canal, tympanic membrane, and middle ear. There were no specific findings in the blood tests. Physical examination revealed a smooth-margined, soft, round, and tender tumor, measuring .3 × .4 cm, in the left crus of the helix (Figure 1A). The patient had no history of trauma or ear surgery. An excisional biopsy was recommended for the patient and discussed with her caregivers. The patient was reviewed at weekly preoperative follow-ups. The tumor showed rapid growth, accompanied by a blood clot, during this period (Figure 1B-D). Preoperative imaging (temporal bone computed tomography (CT) and magnetic resonance imaging (MRI) with gadolinium) was performed (Figure 2A and B). The CT and MRI scans showed a tumor with a well-defined boundary and heterogenous enhancement, measuring 1.6 × 1.3 × 1.3 cm, in the left auricle. There was no evidence of erosion of the adjacent bones. Under general anesthesia, excisional biopsy was performed using a microscope. The tumor originated from the crus of the helix, adjacent to the cartilage. The tumor did not adhere to the surrounding tissues and bled easily. The tumor was removed till only fresh tissue was present. Primary sutures were placed at the biopsy site. Histopathological analysis of the specimen revealed histiocytic infiltrate in the dermis and eosinophilic infiltrate mixed with multinucleated Touton giant cells (Figure 2C). Immunohistochemically, the lesion was positive for CD68, but negative for S100 and CD1a (Figure 2D). These findings are consistent with those of JXG. At the 12-month follow-up, the patient was doing well with no signs of tumor growth or recurrence. Rapidly growing juvenile xanthogranuloma at the crus of the helix. (A) First visit. (B) 1 week after the first visit. (C) 2 weeks after the first visit. (D) 3 weeks after the first visit. Mass (arrow) showing heterogenous enhancement and no erosion of adjacent bones. (A) Temporal computed tomography. (B) Temporal magnetic resonance imaging. (C) Dermal infiltrate of histiocytes and scattered multinucleated giant cells (H&E, ×200). (D) Immunohistochemical staining for CD68 (×400).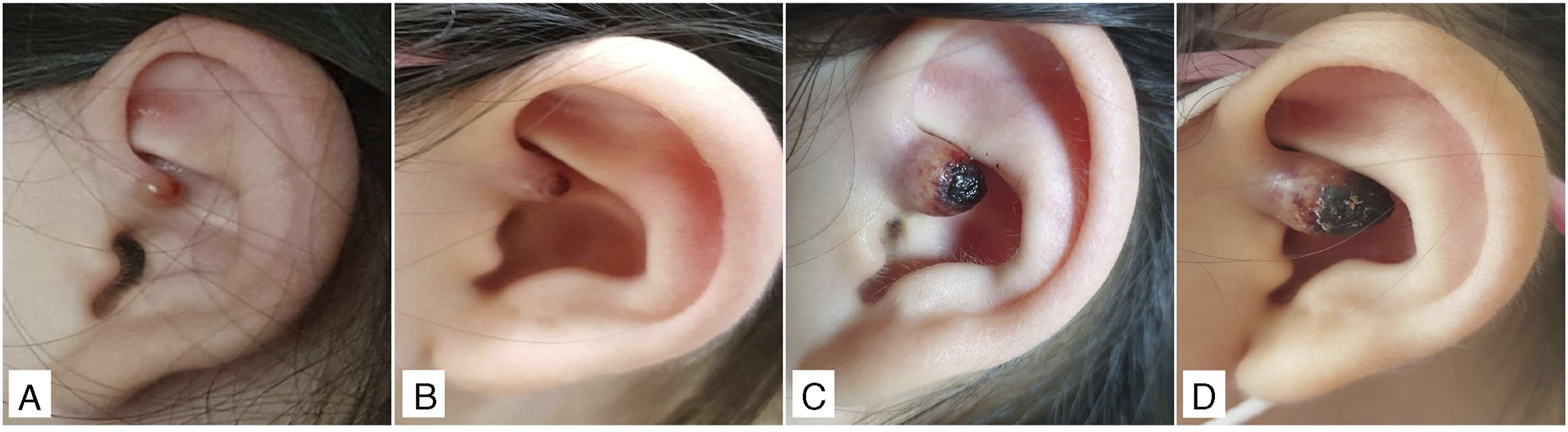

Discussion
JXG is a rare and benign non-Langerhans cell (Class II) histiocytosis. 2 Its incidence rate is unknown. Approximately 70% of JXG occur in infants under 1 year of age. Although rare, JXG can also occur in adults in their late 20s and early 30s; therefore, a bimodal distribution is evident.3,4 The most commonly affected organ is the skin. JXG of the skin tends to be round, with well-defined boundaries, and varying sizes (5–20 mm in diameter). Clinically, JXG mostly appears as a solitary lesion (60%–82%). Approximately 25–30% are multiple lesions.1,3 Multiple lesions most commonly affect the head, neck, and upper trunk; although they can occur on any skin surface, JXG of the auricle is extremely rare. 2 Its exact pathogenesis is unknown. The lesion is presumed to be due to granulomatous reactions of the macrophages and histiocytic cells to trauma or inflammation of an unknown cause. Most JXG lesions regress spontaneously without any sequelae except for atrophic scarring or altered pigmentation. Surgical resection is necessary for rapidly growing lesions and symptomatic cases. Surgery may also be indicated for diagnostic and cosmetic concerns. In most children, local recurrence after excisional biopsy is rare. In contrast, in adults, oral lesions do not resolve spontaneously and recur in approximately 20% of the patients. Therefore, complete removal is required.4,5
In conclusion, in children with lesions of the auricle, JXG should be considered a differential diagnosis, although it is rare. Moreover, if the lesion increases in size rapidly, surgical excision should be performed to ensure an accurate diagnosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.