
Abstract
Objective
To explore the clinical characteristics of patients with dizziness/vertigo who showed a dissociation between the results of the caloric test and video head impulse test (vHIT).
Methods
A total of 327 patients who complained of dizziness/vertigo were continuously included. All patients underwent both the horizontal vHIT (h-vHIT) and caloric tests. Of the 327 patients, 69 patients showed a dissociation between the results of the two tests, 4 patients were excluded because the interval between the two tests exceeded 7 days. Finally, 65 patients were included in the analysis.
Results
Among the 65 patients, 55 (84.6%) patients showed a positive caloric test (+) with a negative h-vHIT (−), and 10 (15.4%) patients showed a negative caloric test (−) with a positive h-vHIT (+). Peripheral and central lesions were identified in 50 (90.9%) and 5 (9.1%) patients, respectively, in the caloric test (+)/h-vHIT (−) group; and central lesions were found in 6 (60%) patients in caloric test (−)/h-vHIT (+) group. The etiologies were unilateral peripheral vestibular dysfunction (n = 25), Meniere’s disease (MD, n = 10), sudden hearing loss with vertigo (SHLV, n = 7), benign paroxysmal positional vertigo (n = 5), vestibular neuritis (n = 2), autoimmune inner ear disease (n = 1), vestibular migraine (VM, n = 3), multiple sclerosis (n = 1), and multiple system atrophy (n = 1) in the caloric test (+)/h-vHIT (−) group, which were SHLV (n = 3), MD (n = 1), VM (n = 1), episodic ataxia type 2 (n = 1), cerebellopontine angle tumor (N = 1), Parkinson’s disease (n = 1), Persistent postural perceptual dizziness (n = 1), and posterior circulation ischemia (n = 1) in the caloric test (−)/h-vHIT (+) group.
Conclusion
Dissociation between the results of caloric test and h-vHIT is not uncommon. A positive caloric test with a negative h-vHIT occurred more frequently, and these patients mostly had peripheral vestibular lesions; while a negative caloric test with a positive h-vHIT was unusual, these patients had both peripheral and central lesions.
Introduction
The vestibular function, especially the horizontal semicircular canal function of patients with dizziness/vertigo and instability, can be evaluated in various frequency ranges. The caloric test is a traditional tool used to evaluate the horizontal semicircular canal function. This test can produce low-frequency stimulation in the horizontal semicircular canal, which is equivalent to head movements with the frequency of approximately .003 Hz. 1 Canal paresis (CP) can be calculated by comparing the difference between caloric responses in bilateral horizontal canals, the angular vestibulo-ocular reflex (aVOR) of the horizontal semicircular canals can also be evaluated. aVOR can reflect the bilateral horizontal canal function. Researchers have devised a variety of test frequency ranges for measuring vestibular function (particularly horizontal semicircular canal function) in patients with dizziness/vertigo and instability. The caloric test is a standard tool for evaluating horizontal semicircular canal function; it generates a very low-frequency stimulation to the horizontal semicircular canal function, equating to a head movement at a frequency of about .003 Hz. 1 The aVOR is tested by calculating the CP value based on the differential in reaction to the caloric test between the two sides of the individual. On both sides, aVOR reflects the function of the horizontal semicircular canal. The caloric test has been the gold standard for aVOR of the horizontal semicircular canal in unilateral or bilateral vestibular function deficits for nearly a century.
A new device, the video head impluse test (vHIT), has been created in recent years to measure aVOR. By monitoring the subject’s eye and head movements in response to high-frequency/high-velocity stimuli, vHIT can detect the high-frequency horizontal aVOR function. vHIT is a safe and simple approach that is comparable to scleral search coils. 2 The vHIT and caloric tests are two regularly used vestibular function tests that are useful in determining the afflicted side and severity of patients with unilateral lesions. Many investigations have shown, however, that these two tests do not necessarily reveal unilateral vestibular hypofunction; in fact, the two tests might occasionally produce dissociated results. Many investigations have verified the dissociation between the outcomes of the two tests, particularly in peripheral vestibular disorders such Meniere’s disease (MD)3,4 and vestibular neuritis (VN).5-7 Many people with a dissociation between caloric and vHIT test results were observed in clinical work; however, it is still unclear whether the dissociation found in these patients is associated to specific disorders. As a result, the goal of this study was to look into the clinical characteristics and etiology of patients who had a dissociation between the findings of the two tests, in the hopes of providing useful information for the clinical diagnosis and treatment of dizziness/vertigo.
Materials and methods
Subjects
A total of 638 patients with dizziness/vertigo attending the vertigo clinic of the Department of Neurology of our hospital from January 2019 to January 2020, were continuously included. Among these patients, 327 patients completed both the horizontal vHIT (h-vHIT) and caloric tests. Of the 327 patients, 69 patients showed a dissociation between the results of the two tests. Considering that long interval between the two tests can not reflect the true horizontal semicircular canal function, so four patients were excluded because the interval between the two tests exceeded 7 days. Therefore, a total of 65 patients were finally included in analysis, including 33 males and 32 females. Written informed consent was obtained from all patients. This study was approved by the ethics committee of our hospital.
Clinical data collection
Baseline data of the patients, including sex, age, current medical history (disease duration, symptoms during onset, onset duration, onset triggers, trigger factors, and concomitant symptoms), neurological examination, and other auxiliary examinations (immune tests, head MR, CT) and clinical diagnosis (sudden hearing loss with vertigo (SHLV), VN, unilateral peripheral vestibular dysfunction (UPVD), benign paroxysmal positional vertigo (BPPV), MD, vestibular migraine (VM), vestibular paroxysmia (VP), autoimmune inner ear disease (AIED)). The diagnosis of UPVD,(8) SHLV,(5) and MD(6) were made based on patient’s medical history, audio-vestibular function assessment, neurological examination, and imaging examination; the diagnosis of VM, BPPV, VN, and persistent postural perceptual dizziness (PPPD) are made according to the diagnostic criteria of the Bárány Society and the International Headache Society.(7,9,10)
Assessment of the vestibular function
Caloric test
During the test, patients were positioned in the supine position in the semi-dark room, with their head tilted up about 30°and with goggles placed over their eyes. The right and left external auditory canals were irrigated with hot air at 50°C and cold air at 24°C, respectively, for 1 minute. The caloric irrigation was performed in the following order: right ear warm (50°C, RW), left ear warm (50°C, LW), right ear cold (24°C, RC), left ear cold (24°C, LC), the between-irrigation interval was 5 minutes. Each irrigation was only performed until the nystagmus had completely disappeared. The sides of strong and weak caloric responses were determined by the maximum slow phase velocity (SPV) values of the total responses from the left and right ears (i.e., absolute SPV values of RC + RW responses vs the absolute SPV values of LC + LW responses). 11 CP was calculated according to the following formula: CP = ((RW + RC)−(LW + LC)/(RW + RC + LW + LC)) × 100%. CP >25% was defined as horizontal semicircular dysfunction. 12 Bilateral vestibulopathy (BVL) was diagnosed if the sum of the peak SPV of nystagmus after warm and cold irrigation on each side was <6°/s, that is, the sum of the peak SPV of nystagmus of RW + RC + LW + LC was <12°/s bilaterally; there were no patients who met this criterion in this study, so the diagnosis of BVL was not made.
vHIT
vHIT (Interacoustics, Middelfart, Denmark) was used to evaluate the function of the three pairs of semicircular canals. The instrument comprises an inertial measurement unit to measure head movements and an infrared camera to record eye movements. In a brightly lit room, patients were in the sitting position and were instructed to fix their eyes on a target at eye level and at a distance of 1.5 m. The examiner stood behind each patient while holding the patient’s head between both hands. 20 head impulses were delivered in each canal plane in a brief, rapid, passive manner, the angular velocity was 150–250°/s for the horizontal canal impulses, 100–200°/s for the vertical canal impulses, and the amplitude was 10–20°. The vHIT software was used to record the average slow phase VOR gain values. VOR gain is defined as the ratio of eye velocity to head velocity at 60 s. The normal VOR gain for the horizontal semicircular canals was between .79 and 1.20, and vertical semicircular canals was between .7 and 1.2.13,14 This study was included with a horizontal semicircular canals vHIT gain of ≤.78 and vertical semicircular canals vHIT gain of ≤.7 as an abnormality criterion. CP > 25% of caloric test was recorded as caloric test (+), otherwise caloric test (−); horizontal vHIT gain ≤.78 and vertical vHIT gain <.7 was recorded as vHIT (+), otherwise vHIT (−). A covert saccade occurs before the end of the head pulse, while an overt saccade occurs after the end of the head pulse, according to the vHIT report. The definition of CS is based on earlier research, which states that abnormal CS in vHIT is defined as more than three repetitive saccade. 15 In order to eliminate artifacts such as blink waves from distorting the saccade analysis, artifacts are excluded by referring to the Mantokoudis study. 16
Statistical analyses
The continuous variables were expressed as the mean and standard deviation (mean ± SD). Categorical variables are expressed as percentages, and differences between groups were analyzed with the chi squared (χ2) test, followed by Yates' continuity correction or Fisher’s exact test if necessary. A two-sided P value <.05 was considered statistically significant. All statistical analyses were performed using SPSS version 20.0 (SPSS, Chicago, IL).
Results
Baseline data of the patients
This study included 65 patients, of whom 55 (84.6%) showed a positive caloric test (+) with a negative h-vHIT (−), and 10 (15.4%) showed a negative caloric test (−) with a positive h-vHIT (+). There were no statistical differences in the male to female ratio (1:1 vs 1:1.5) as well as age at onset (54.1 ± 15.4 vs 64.4 ± 13.7) between patients in the caloric test (+)/h-vHIT (−) group and caloric test (−)/h-vHIT (+) group (both P>.05).
Distribution characteristics of patients showing a dissociation between the results of the two tests
The CP values were 42.9 ± 16.4% and 9 ± 5.5%, respectively, in the caloric test (+)/h-vHIT (−) group and caloric test (−)/h-vHIT (+) group.
In the caloric test (+)/h-vHIT (−) group, the h-vHIT gain on the affected side was 1.0 ± .1, the asymmetry ratio of the h-vHIT gain was .04 ± .03. In the caloric test (−)/h-vHIT (+) group, 6 (60%) patients had bilateral gain reduction, the asymmetry ratio of the h-vHIT gain was .08 ± .05; 4 (40%) patients had unilateral gain reduction, h-vHIT gain was .54 ± .04, the asymmetry ratio of the h-vHIT gain was .26 ± .05.
In the caloric test (+)/h-vHIT (−) group, although all patients had normal horizontal vHIT gain, we found that 36.4% (20/55) patients had corrective saccade (CS) on the abnormal side of the caloric test, with 5% (1/20) of covert CS, 65% (13/20) of overt CS, and 30% (6/20) of covert combined with overt CS. All patients with abnormal vHIT gain in the caloric test (−)/h-vHIT (+) group had CS, including 60% (6/10) of overt CS and 40% (4/10) of overt mixed with covert CS.
In the caloric test (+)/h-vHIT (−) group, 3.6% (2/55) of patients on the abnormal side of the caloric test had ipsilateral superior or posterior semicircular canals vHIT gain abnormalities; In the caloric test (−)/h-vHIT (+) group, 30% (3/10) of patients on the abnormal side of the horizontal vHIT gain abnormalities had ipsilateral superior or posterior semicircular canals vHIT gain abnormalities, χ2 = 4.99, P =.026.
Disease duration
In the caloric test (+)/h-vHIT (−) group, disease duration was ≤1 week in 20 (36.4%) patients, 1 week–3 months in 19 (34.5%) patients, and ≥3 months in 16 (29.1%) patients. In the caloric test (−)/h-vHIT (+) group, disease duration was ≤1 week in six (60%) patients, 1 week–3 months in three patients (30%), and ≥3 months in one (10%) patient.
Etiology
In the caloric test (+)/h-vHIT (−) group, peripheral vestibular lesions were found in 50 (90.9%) patients, central lesions were found only in 5 (9.1%) patients. In the caloric test (−)/h-vHIT (+) group, central lesions were found in 6 (60%) patients. There was significant difference in the lesion location between two groups (P=.001, Fisher’s exact test).
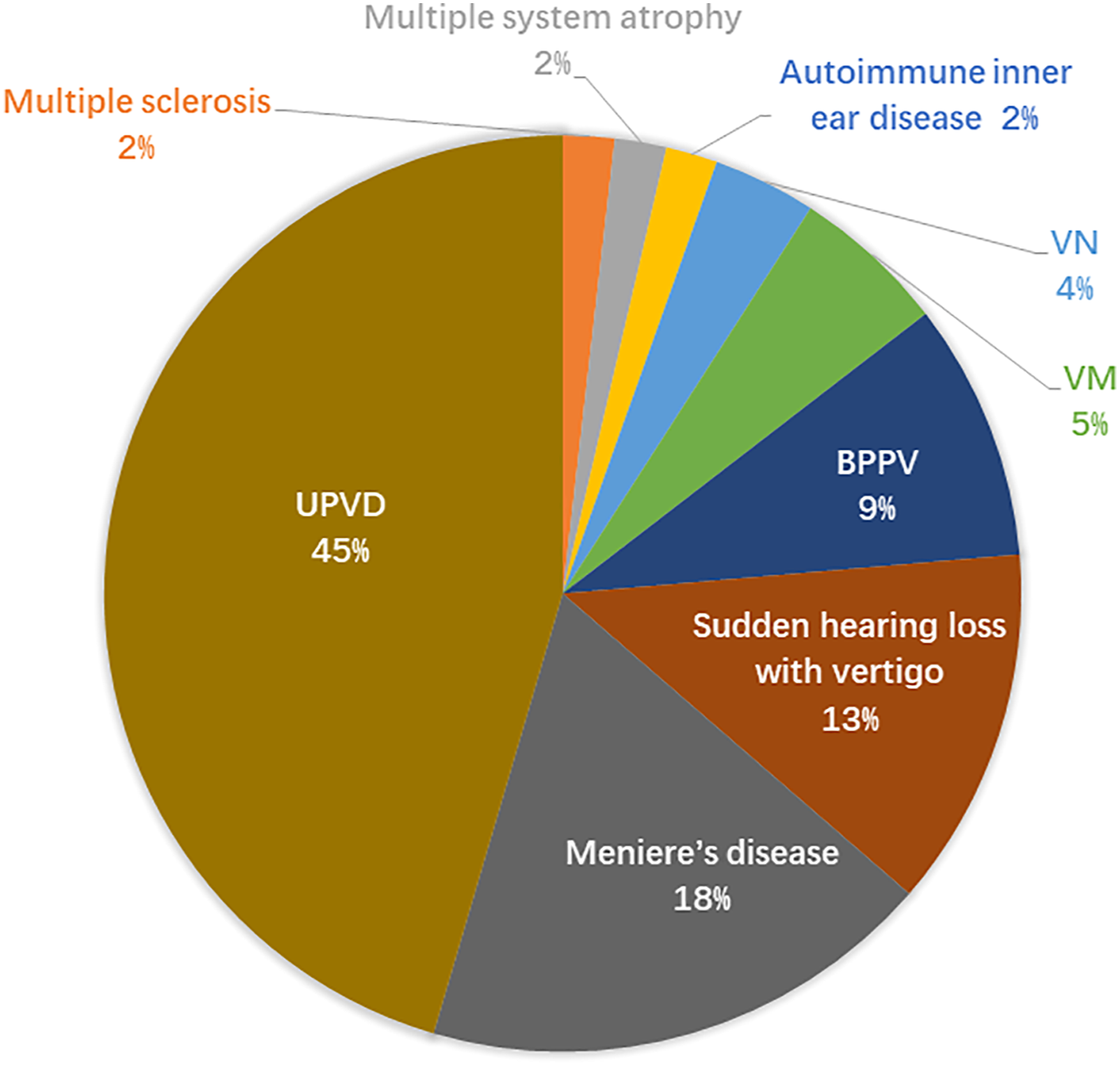
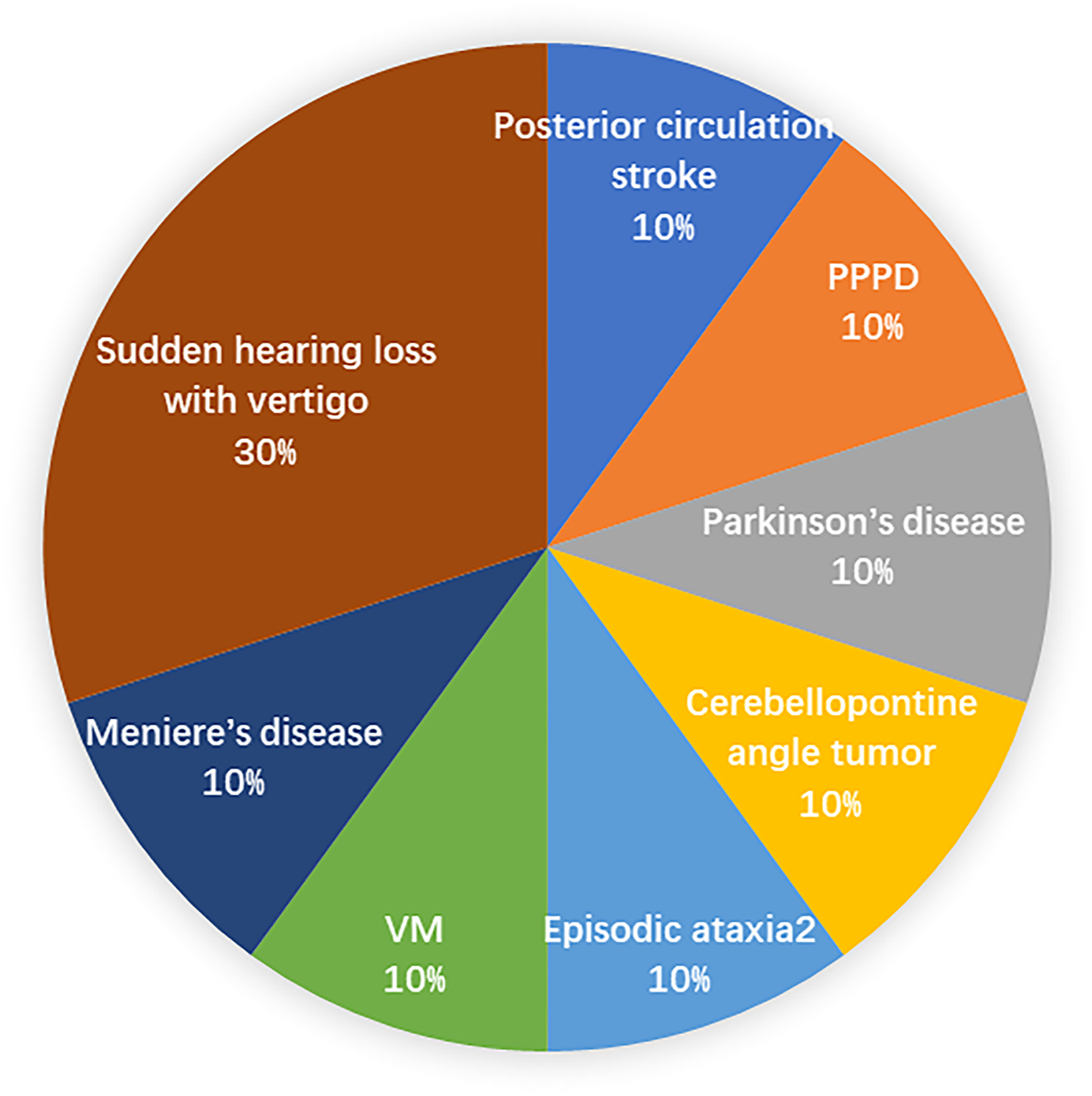
The main etiologies were UPVD (n = 25), MD (n = 10), SHLV (n = 7), BPPV (n = 5), VN (n = 2), AIED (n = 1), VM (n = 3), multiple sclerosis (n = 1), multiple system atrophy (n = 1) in the caloric test (+)/h-vHIT (−) group, which were SHLV (n = 3), MD (n = 1), VM (n = 1), episodic ataxia type 2 (n = 1), cerebellopontine angle tumor (N = 1), Parkinson’s disease (n = 1), PPPD (n = 1), posterior circulation ischemia (n = 1) in the caloric test (−)/h-vHIT (+) group (Figures 1–3). Comparison of the etiological distribution between patients in the two groups. Etiological distribution of patients in the caloric test (+)/h-vHIT (−) group. Etiological distribution of patients in the caloric test (−)/h-vHIT (+) group.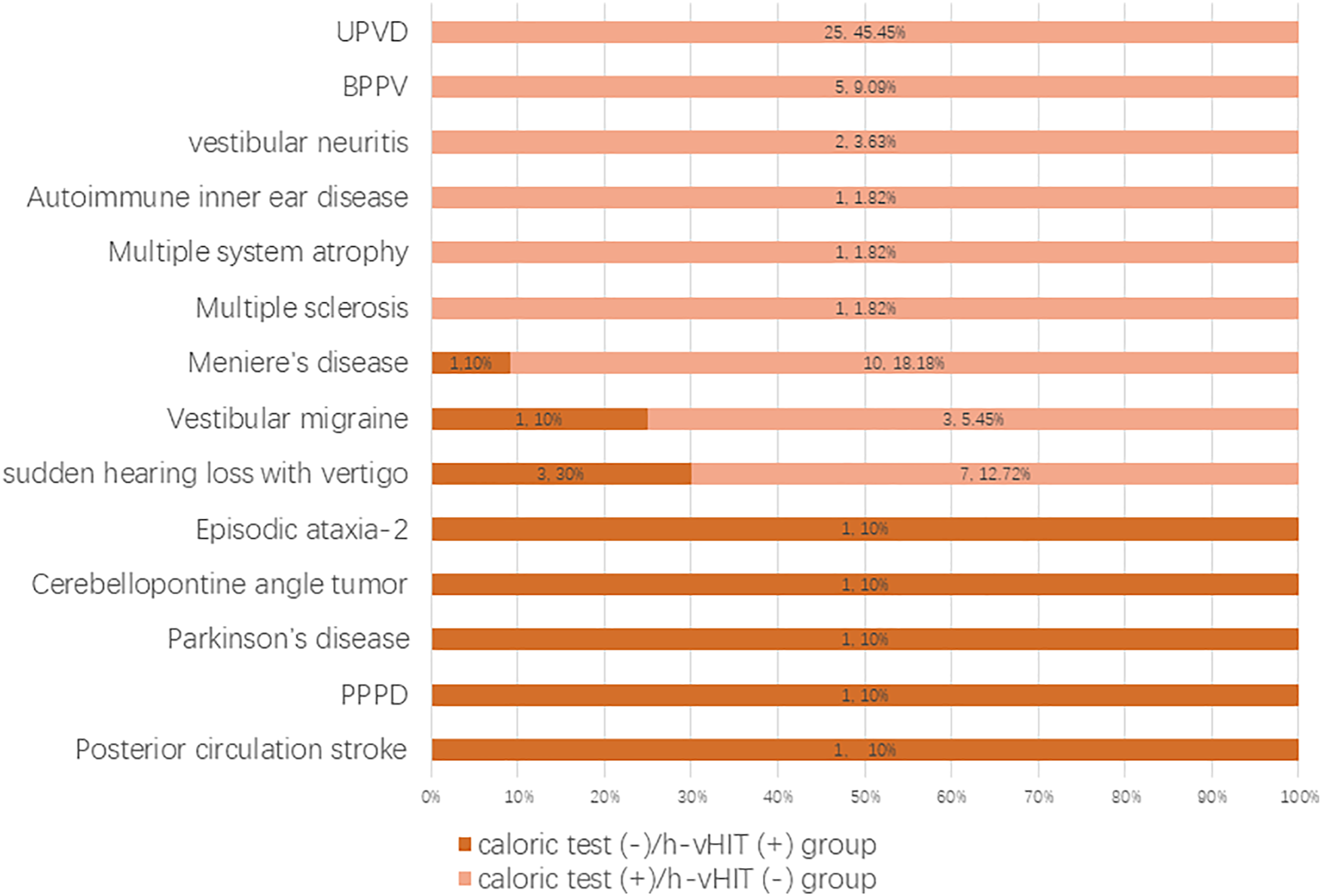
Discussion
In some patients with dizziness/vertigo, there is a discrepancy between the caloric test and the vHIT. In this study, 19.88% of 327 patients with dizziness/vertigo who got treatment in the vertigo clinic of our hospital’s Department of Neurology and did both the h-vHIT and the caloric test exhibited a dissociation between the two tests. This observation is comparable to that of Kim et al., 4 who found that 18.1% of patients had dissociated results between the caloric test and the vHIT. Patients in the caloric test (+)/h-vHIT (−) group had predominantly peripheral vestibular lesions, whereas patients in the caloric test (−)/h-vHIT (+) group had both peripheral and central vestibular lesions.
Our data revealed that 90.9% (50/55) of patients in the caloric test (+)/h-vHIT (−) group had peripheral vestibular lesions, with UPVD (45.5%) being the most prevalent cause, followed by MD (18.2%). Many prior research showed that endolymphatic hydrops was to blame for the dissociation between caloric and vHIT outcomes.3,4,17 Endolymphatic hydrops can greatly increase the cross-sectional area of the endolymphatic duct, thereby enlarging its volume and causing convective currents between high-density and low-density endolymph, resulting in pressure gradient generation near the crista ampullaris and the reduction of the buoyant force, which counteracts the hydrostatic pressure acting on the crista ampullaris, thus weakening the degree. However, because the size or shape of the complete bone labyrinth does not change, the stimulation speed created by vHIT does not change, that is, the vHIT gain does not change. 18 This theory was also supported by a recent study, 18 which employed intravenous Gd enhanced inner ear MRI to assess endolymphatic hydrops in MD patients with normal vHIT gain and discovered that the level of endolymphatic hydrops was associated to the decrease in caloric responses. 19 However, only 18.2% of the patients in this study were diagnosed with MD, which differs from the previous study. This could be because most of our patients present with recurrent dizziness/vertigo during a disease-free period, and the pathological changes of the disease as well as the clinical symptoms are not typical enough.
Although vHIT gain is now the primary indicator for assessing peripheral vestibular function,20,21 the CS of vHIT is often employed as a secondary indicator, CS can also indicate the degree of recovery of peripheral vestibular organ function.22,23 Although all patients in the caloric test (+)/h-vHIT (−) group of this study had normal horizontal vHIT gain, 36.4% (20/55) had CS on the abnormal side of the caloric test. Perez et al 24 employed vHIT to analyze 623 individuals with dizziness/vertigo, and they discovered 36 patients with normal horizontal vHIT gain values and CS. The researchers came to the conclusion that this group of individuals had lesser degree of peripheral vestibular function. The function of previously damaged peripheral vestibular organs will be largely restored over time as a result of central compensatory activity of the vestibular system, contributing to the recovery of vHIT gain to normal.25,26 CS still occurs, though, because the VOR is slightly diminished. Another study indicated that in individuals with impaired vestibular function, high-frequency function of the VOR (vHIT gain) was the quickest to recover, possibly because daily activities are largely high-frequency motions and people do vestibular rehabilitation exercises by walking unconsciously. While the VOR’s low-frequency function recovers more slowly, abnormal caloric test CP values can linger for months, 27 which is more akin to the current study. As a result, dissociation results from the two tests may be connected to the degree of disease healing. Low vHIT gain and high amplitude CS characterize acute peripheral vestibular lesions, but as the disease progresses, vHIT gain returns to normal and CS amplitude and frequency diminish. As a result, the dissociation of the two test results could be due to the patients’ slow recovery of vestibular function in this study.
In other words, the dissociation of the two test findings in the caloric test (+)/h-vHIT (−) group could be connected to the disease’s origin, as well as the disease’s length, pathophysiology, degree of lesions, and whether the disease is in exacerbation or remission.16,27 In our study, there was significantly less ipsilateral impairment of vHIT gain in vertical semicircular canals (3.6%) in the caloric test (+)/h-vHIT (−) group compared to previous studies, 26 and we discovered that 63.6% of the patients had subacute or chronic diseases, and the majority of the patients had recurrent dizziness/vertigo. The caloric test (CP values) has been shown to reflect semicircular canal function for lengthy periods of time, 28 but vHIT increase can quickly return to baseline. The majority of the patients in this study had recurrent dizziness/vertigo and were in remission; thus, their high-frequency aVOR function was recovered during the remission period, but their low-frequency aVOR function was not, resulting in a dissociation between the two tests’ results.
A negative caloric test with a positive vHIT is another dissociation pattern. Our dissociation pattern was seen in 15.39% (10/65) of the patients in this study, which is a somewhat uncommon pattern. In most cases, a decrease in vHIT gain and the presence of CS are considered signs of peripheral vestibular lesions; however, abnormal vHIT can also be seen in central lesions, 29 where the causes of central lesions include compression of the vestibular nuclei, eighth cranial nerve, impaired blood supply to the inner ear, or lateral pons infarction. 30 The labyrinth, lateral pons, and flocculus are all supplied by the anterior inferior cerebellar artery (AICA). Audio-vestibular impairment can result from an AICA infarction. Chen et al. 31 discovered that 13 of 33 patients with PCS suffered AICA stroke, and that vHIT demonstrated bilateral gain decrease in these 13 patients with relatively mild saccades. Furthermore, the caloric test was normal in these patients, demonstrating that the caloric and vHIT test findings were dissociated. This could be due to the degree of inner ear, vestibular nuclei, and flocculus involvement. According to previous research, lesions of the flocculonodular lobe can cause an abnormal h-vHIT but a normal caloric test. The direct VOR pathway between the vestibular nuclei, which can decrease VOR gain during low-frequency stimulation and boost VOR during high-frequency stimulation, may play a role in the regulation of horizontal VOR.32,33 During vestibular testing after a flocculus lesion, dynamic vestibular response patterns appear, such as a decrease in vHIT gain during healthy side head rotations and a normal caloric test. The above-mentioned locations, such as the flocculus, may be involved in the current investigation for patients with cerebellopontine angle tumor and EA-2, resulting in dissociation between the results of the two tests. However, the patients identified with diagnoses such as VM and posterior circulation ischemia in this study that did not clearly involve the brainstem, cerebellum, or AICA lesions, they may have had a mix of peripheral vestibular disorders and thus had aberrant vHIT.
Peripheral vestibular lesions were less common in the caloric test (−)/h-vHIT (+) group in this investigation; only four patients had clearly identified peripheral vestibular lesions, three of whom had bilaterally diminished VOR gains in the horizontal semicircular canals. Furthermore, three patients with central lesions that were possibly accompanied by peripheral vestibular lesions showed bilateral gain reduction in the horizontal semicircular canals. The reason for this could be that during the acute stage of peripheral vestibular lesions, the static compensatory mechanism kicks in, and the bilateral vestibular nuclei use the push-pull mechanism to rebalance the firing rates of the vestibular nerves on both sides, reducing the horizontal VOR gain. However, among patients with clearly defined peripheral vestibular lesions, two patients with SHLV had bilateral lesions, which could be due to vestibular dysfunction on both sides caused by factors such as vascular lesions. These patients showed only VHIT gain impairment, which we speculate could be due to damage to the blood vessels supplying the high-frequency vestibular nerve, resulting in the dissociation between vHIT and caloric results. The sickness duration in the other two patients (diagnoses of VM and posterior circulation ischemia) with central lesions perhaps accompanied by peripheral vestibular lesions was 10 days, indicating that the lesions had not entirely invaded the vestibular organs. Lee et al. 34 performed vestibular function testing on patients with VN who presented with acute vestibular illness and discovered that caloric test results were normal within 2 days of disease onset in these individuals. In these patients, the authors believe that inflammation may worsen with time, and vestibular function may vary depending on the intensity of the inflammation and the sensitivity of brain systems; therefore, low-frequency vestibular afferents (.003 Hz) may be relatively spared during the early stages of inflammation, resulting in a normal caloric test. As a result, lesions may be caused not only by inflammatory mechanisms, but also by vascular mechanisms, which affects the extent of peripheral vestibular lesions. However, because such lesions are uncommon, the dissociation between caloric and vHIT test results produced by this type of peripheral vestibular lesions requires further investigation.
Conclusions
Dissociation between the results of caloric test and h-vHIT is not uncommon. A positive caloric test with a negative h-vHIT was more common, and these patients mostly had peripheral vestibular lesions; however, a negative caloric test with a positive h-vHIT was uncommon, and these patients had both peripheral and central vestibular lesions. More research is needed to look at the underlying causal links.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Aerospace Center Hospital (Grant no. YN202106).