
Abstract
Objective:
To compare video head impulse test (vHIT) and caloric test efficacy in decompensated and compensated vertigo patients and to further investigate whether vHIT alone can be used as a diagnostic tool in vertigo.
Methods:
This study included 25 patients diagnosed with vertigo and without any previous history of vertigo or hearing loss before their admission to our clinic. The control group consisted of 16 healthy adult volunteers. Patients were classified into 2 groups, compensated and decompensated. Video head impulse test and caloric tests were performed and the results were compared between the groups.
Results:
The difference of caloric test values between control-compensated groups and compensated-decompensated groups was statistically significant (P < .001, Pearson χ2). However, there was no statistically significant difference between the compensated and control groups according to vHIT gain asymmetry values (P = .087). In the very early stages of the disease with spontaneous nystagmus, the diagnostic significance of vHIT was similar to that of the caloric test. When both sides were compared, vHIT gain asymmetry values were close to the caloric test asymmetry values. In the compensated stage, caloric test was superior to vHIT in differentiating compensated vestibular pathologies. When vHIT sensitivity was evaluated according to the bi-thermal caloric test results, the sensitivity of the vHIT gain asymmetry value was 85.71% and 23.08% for decompensated and compensated patients respectively.
Conclusion:
In the early decompensated stages of the disease with spontaneous nystagmus, vHIT shows similar diagnostic accuracy to that of the caloric test. Since patients can tolerate vHIT more easily, our results suggest that vHIT can be considered as a primary evaluation method in the early (decompensated) period of the disease and should be preferred over the caloric test during the acute phase. Caloric test is more reliable at the compensated stage. Video head impulse test is inadequate in evaluating the compensated vestibular hypofunctional states after compensation has been restored.
Level of Evidence:
Level 2b
Introduction
Bi-thermal caloric test is a traditional test that provides information about the vestibular function of the ear by comparing the function of 2 horizontal canals on both sides1,2 and is widely used in vertigo clinics but has many limitations as described in the literature.3,4 An important limitation is that the caloric test produces low-frequency stimulation in the vestibular system. Vestibular receptors respond to sudden, short head movements between 1.0 and 3.0 Hz, whereas caloric test represents head movement equivalent to about 0.003 Hz. This means that the caloric stimulus frequency is significantly below the optimal effective processing limit of the vestibular receptors. Moreover, caloric test is based on comparing the responses of both sides to caloric stimuli. In the presence of bilateral vestibular function loss (such as amino-glycoside toxicity), the results may be within normal limits due to symmetrical loss of vestibular function. Moreover caloric tests only evaluates lateral semicircular canal. Therefore, the evaluation of bilateral peripheral vestibular pathologies should be made cautiously by bi-thermal caloric tests.
A more practical vestibular evaluation method was necessary to assist or replace the caloric test to compensate for the limitations mentioned above. The head impulse test was first described by Halmagyi and Curthoys in 1988. 4 MacDougall et al developed a video detector and recording system (video head impulse test [vHIT]) in 2009 that could individually test each of the 6 semicircular canals. 5 Because this system is easy to implement, cheap, and tolerable more easily, it has started to replace the routine VNG-registered bi-thermal caloric testing in many vertigo clinics. 2 This test has several advantages. First of all, there is no loss of the stimulus energy given by head thrusts to the semicircular canals. 3 Other than that, the test is not affected by anatomical differences of the external ear canal and the tympanic membrane. Besides, it can be applied easily even at the patient’s bedside, lasts about 10 minutes, and can be applied even during the acute vertigo attacks, which is an important advantage over caloric testing. 6 It does not require a special room and room conditions during the test. Six semicircular canal functions can be evaluated separately, the (repeatable) test is easily tolerated by patients including children and patients with severe vertigo; therefore, it may be used for follow-up in case of ototoxic drug usage.2,7,8
The aim of this study was thus to compare the efficacy of vHIT and caloric tests in different stages of vertigo and to investigate whether vHIT can solely be used as a diagnostic tool in vertigo.
Materials and Methods
This prospective study was performed on 25 patients who presented with vertigo complaints to our clinic between March and September 2018 without any previous vestibular or auditory complaints prior to their application to our clinic. Seventeen of 25 patients were male and 8 of 25 patients were female. The mean age at the time of diagnosis was 45.5, ranging between 33 and 68. Sixteen healthy, age-matched adult volunteers between 30 and 65 years of age without any known diseases were randomly selected as the control group. The control group consisted of 9 of 16 female and 7 of 16 male healthy adults. The mean age of the control group was 44.5 ranging between 30 and 65 years.
After detailed history was obtained, full otolaryngologic, neuro vestibular and oculomotor examinations were performed to all patients and volunteers (control group) by the same person. People who could not tolerate caloric test and who were diagnosed as Benign positional paroxysmal vertigo were not included in the study.
The patients were classified into 2 groups: patients with spontaneous nystagmus were classified as the decompensated group and patients without spontaneous nystagmus were classified as the compensated group. Of the 25 patients, 18 had no spontaneous nystagmus on their first exam. These patients were accepted as the compensated patient group. All of the remaining 7 patients presented with an acute vestibular attack. Their examinations revealed spontaneous nystagmus and were included in the decompensated patients’ group. The diagnosis of 18 patients in the compensated group were as follows: 2 as Meniere disease, 2 as labyrinth fistula, three as acoustic neuroma, 11 as vestibular neuritis. The diagnosis of 7 decompensated patients were 6 vestibular neuritis, 1 Meniere disease.
Video head impulse test and then bi-thermal caloric tests were performed on the same day in the compensated group. In the decompensated group, vHIT was performed on the day of admission. After the recovery of spontaneous nystagmus (mean 10 days), repeat vHIT and bi-thermal caloric tests were performed. Bi-thermal water caloric test was performed in the standard fashion with water with Disoft infra-red video oculography system (DIFRA; Micromedical Technologies). Thirty percent difference in responses to caloric stimuli between the canals were considered as canal hypofunction. Video head impulse test was performed by applying 20 stimuli toward each direction with the Visual Eyes 4 Channel system of Micromedical Technologies. Although all 6 canals were tested with vHIT, only lateral canal responses were evaluated since only lateral canals can be tested with caloric test. All the tests were performed by the same person. Overt and covert saccades were recorded, vestibuloocular reflex (VOR) gain and gain asymmetry values were noted. Gain values of 0.79 to 1.20 were accepted as normal. Gain asymmetry values of 13.3 and above between ears of the same individual were considered as abnormal. 9 Normal and abnormal test results were shown in Figures 1 and 2, respectively.
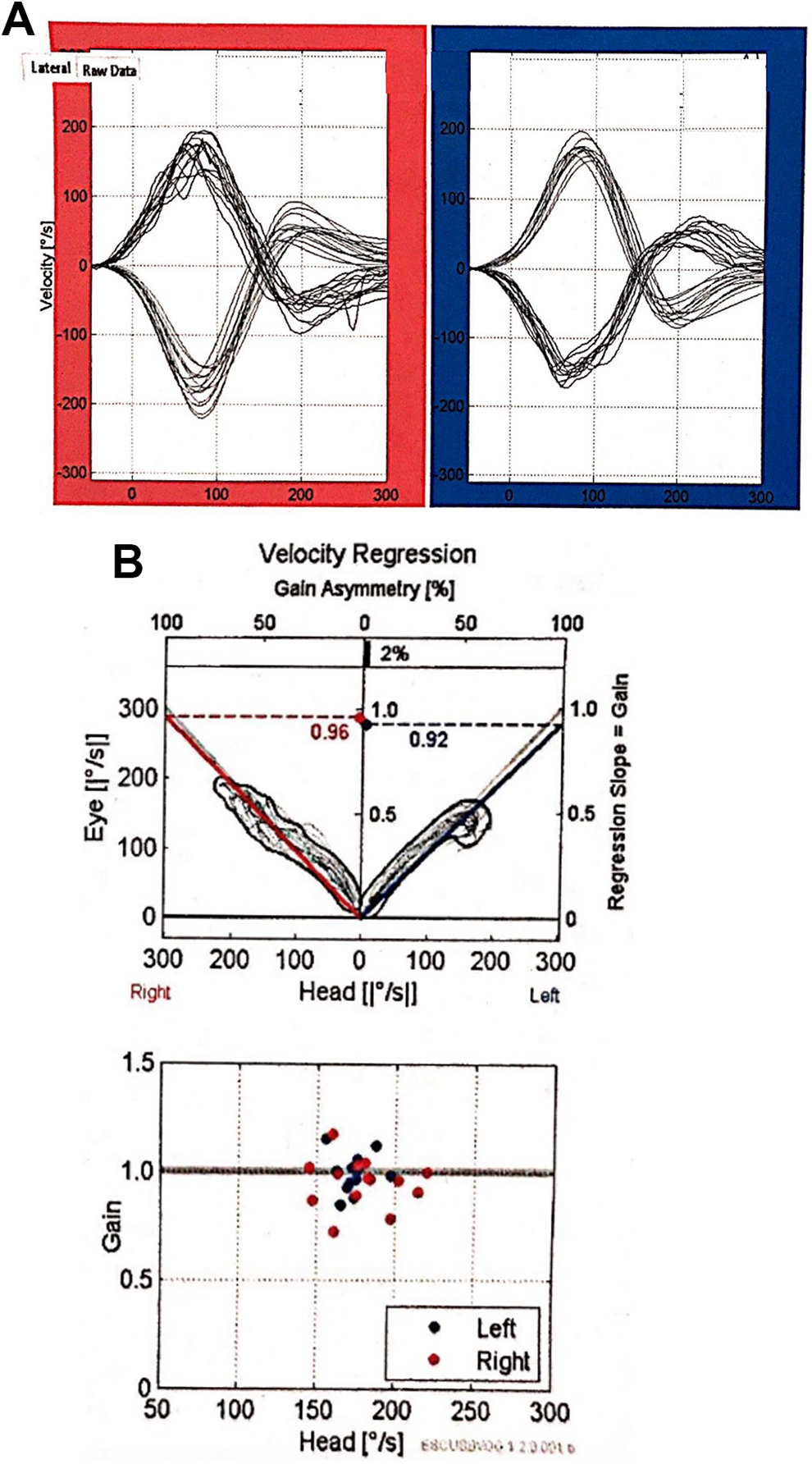
vHIT analysis of a healthy volunteer. A, Blue color represents the results for leftward head turns (function of the left horizontal canal). Red color shows the results for rightward head turns (function of the right horizontal canal). The eye velocity records (lower line) have been inverted and superimposed on the head velocity records (upper line), showing the close match of the 2 velocities. B, The top graphic shows the gain asymmetry value of 2%, which falls in the normal range (0%-13.3%). The lower graphic shows the VOR gains for rightward (red circles) and leftward head turns (blue circles) for the peak head velocity for every single head turn in both directions. Vestibuloocular reflex gains close to 1.0 shows normal semicircular canal function for both directions of head rotation. vHIT, indicates video head impulse test.
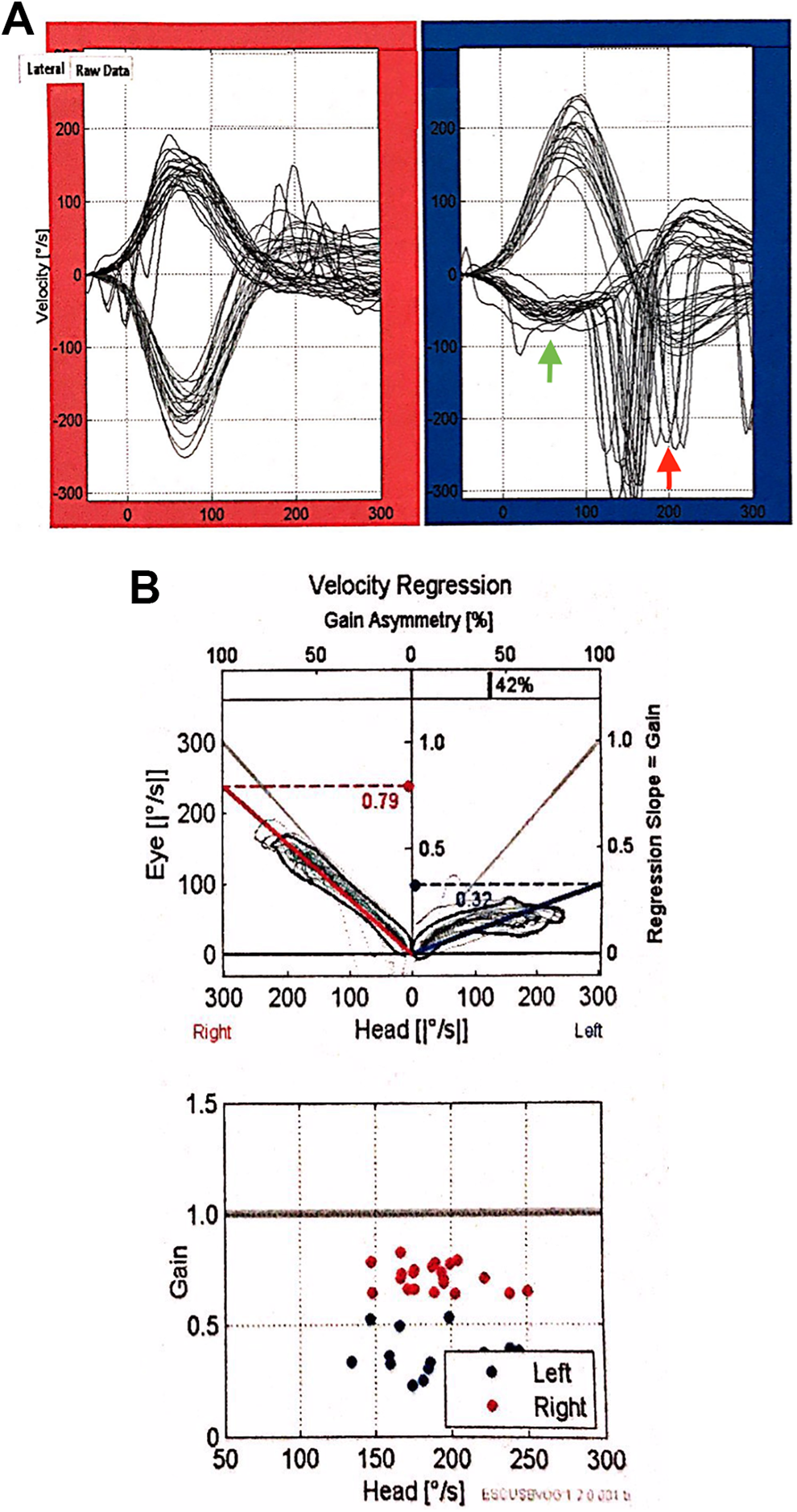
vHIT analysis of a patient with unilateral (left) vestibular hypofunction. Blue: left side, red: right side. Green arrow represents covert saccades, red arrow represents overt saccades. A, During impulses toward the affected left side, the eye velocities reached are much lower than those during impulses toward the intact right side, and the VOR gains for the leftward impulses are correspondingly lower. Gains for impulses toward the right side have nearly normal value. B, The gain asymmetry is 42% between 2 sides. The VOR gains for the ipsilesional leftward head turns are all around 0.3, which is substantially below the range of normal gains (0.79-1.20). vHIT, indicates video head impulse test.
Video head impulse test analysis of a patient with unilateral (left) vestibular hypofunction (Figure 2) shows that the head impulses to the affected (left) side resulted in significantly low VOR gains and eye velocities compared to the unaffected (right) side. After cessation of the impulses, strong overt saccades were observed on the left paretic side around 200 ms. The last few impulses resulted in covert saccades around 100 ms.
Statistical Analysis
The paired group comparisons (control vs compensated, control vs decompensated, compensated vs decompensated) of caloric test and vHIT gain asymmetry frequencies were made with multi-eyed χ2 test. Cutoff values were 30% or more difference for bi-thermal caloric test and 13.3 or more for vHIT gain asymmetry values. The multivariate analysis of the effect of age and sex as an independent variable on the caloric test and vHIT gain asymmetry frequencies, and independent predictors of these factors in predicting vHIT gain asymmetry values with the caloric test were analyzed using logistic regression analysis. Hosmer–Lemeshow test was used for model fit.
The number of patients in the study groups was calculated using ANOVA power analysis with 80% power (1-β) and at .05 statistical significance (α) with 0.69 effect size. According to these assumptions; it was found that at least 7 individuals were required for 3 study groups.
Results
The age distribution and the averages were similar in all 3 groups. There was no statistically significant difference among the groups (P = .813, ANOVA). Gender distributions were also similar among the groups, and there was no statistically significant difference (P = .164, Pearson χ2).
The differences between the percentages in all 3 groups were statistically significant (P < .001, Kruskal Wallis). The differences between the percentages of vHIT gain asymmetries in all 3 groups were statistically significant (P < .001, Kruskal Wallis).
When we compared up to the cutoff value of 30% in the caloric test as a normal limit, there was a statistically significant difference in all 3 groups (P < .001, Pearson χ2). In the decompensated group, caloric test values of 30% or more were obtained in all patients. In the compensated group, 13 of 18 patients had caloric test values above 30%, while 5 of 18 patients had caloric test values within the normal limits. Caloric tests were normal in all subjects in the control group.
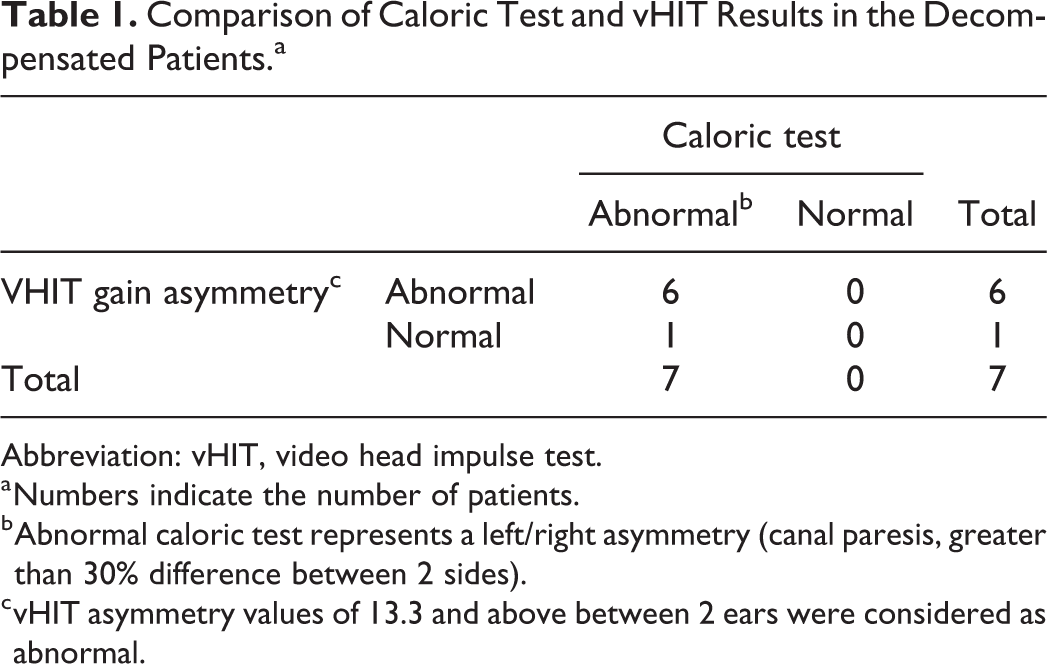
Regarding vHIT, when the comparison was made using the cutoff value of 13.3%, the differences in all 3 groups were statistically significant (P < .001, Pearson χ2). Video head impulse test gain asymmetry in the decompensated 7 patients was over 13.3 in 6 of 7 patients, and below 13.3 in only 1 of 7 patient (Table 1).
Comparison of Caloric Test and vHIT Results in the Decompensated Patients.a
Abbreviation: vHIT, video head impulse test.
a Numbers indicate the number of patients.
b Abnormal caloric test represents a left/right asymmetry (canal paresis, greater than 30% difference between 2 sides).
c vHIT asymmetry values of 13.3 and above between 2 ears were considered as abnormal.
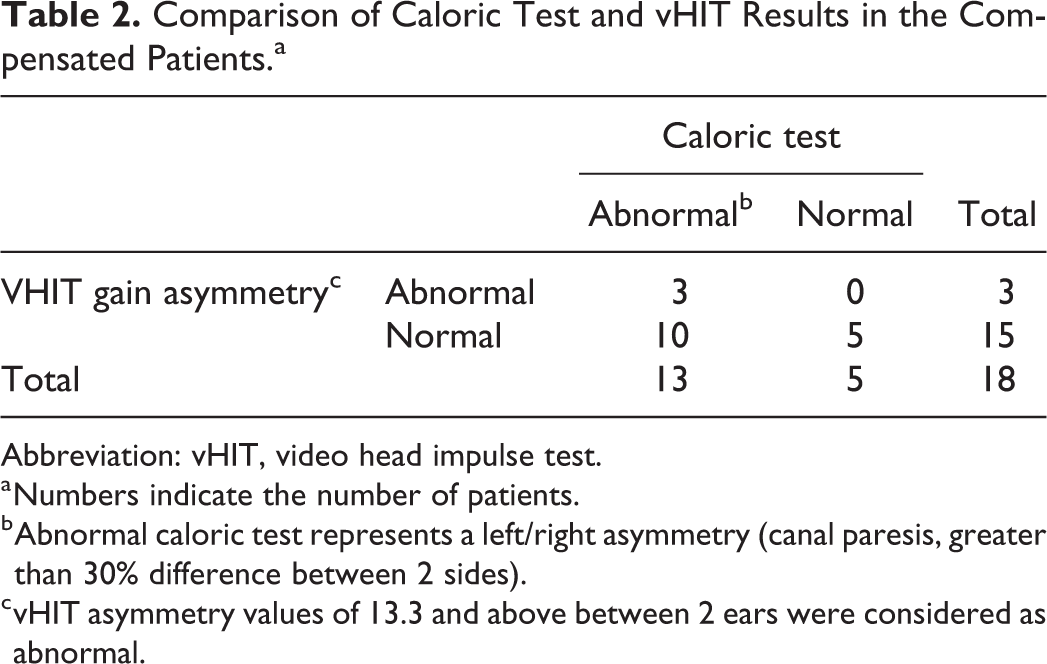
In the compensated patient group, 3 of 18 patients gain asymmetry was higher than normal range (0-13.3%) 9 and 15 of 18 patients were in the normal range. Gain asymmetry was below 13.3 in all patients in the control group (Table 2).
Comparison of Caloric Test and vHIT Results in the Compensated Patients.a
Abbreviation: vHIT, video head impulse test.
a Numbers indicate the number of patients.
b Abnormal caloric test represents a left/right asymmetry (canal paresis, greater than 30% difference between 2 sides).
c vHIT asymmetry values of 13.3 and above between 2 ears were considered as abnormal.
When the comparison was made according to the cutoff value of 30% or more in the caloric test, the differences of the frequencies between decompensated patients with normal individuals and compensated patients with normal individuals and decompensated patients with compensated patients were statistically significant, respectively (P < .001, Pearson χ2; Table 3).
Comparison of Caloric Test and vHIT Results Based on Their Cutoff Values in Coupled Groups.
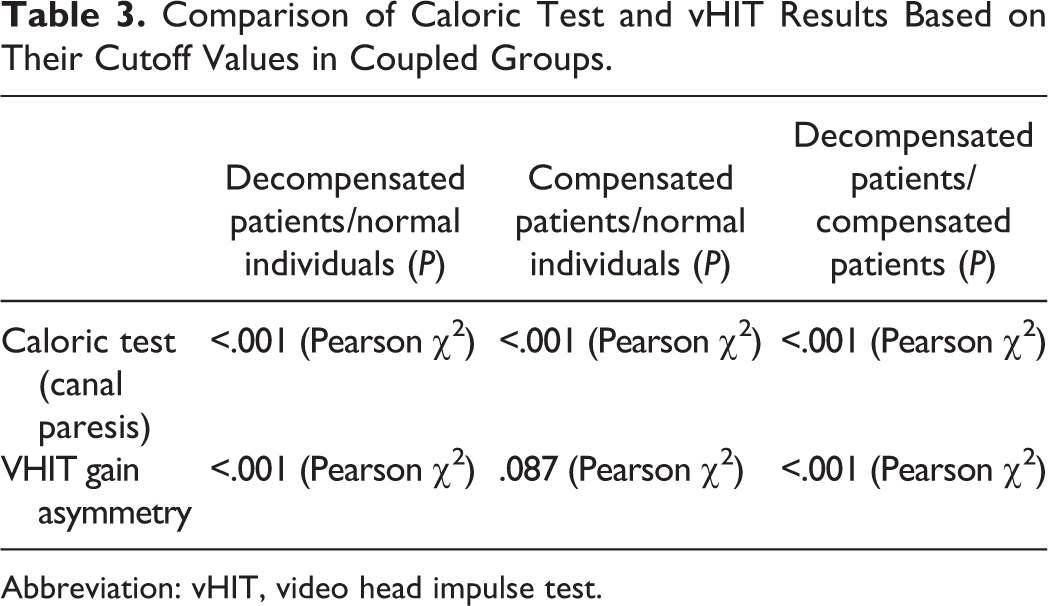
Abbreviation: vHIT, video head impulse test.
There was a significant difference between the frequencies (P < .001, Pearson χ2) in paired group comparisons with vHIT (decompensated patients/control individuals, decompensated/compensated patients). However, the frequency between compensated patients and normal individuals was not statistically significant. (P = .087, Pearson χ2; Table 3).
Video head impulse test and caloric test results of the 7 decompensated patients and of 7 randomly selected compensated patients are shown in Table 4. In the 7 decompensated patients, caloric test showed unilateral impairment in all 7 and vHIT in 6 of 7, so that asymmetry results were similar in the 2 tests. In contrast, in the 7 compensated patients, caloric test showed unilateral impairment in 6 of 7, whereas vHIT in only 2 of 7. Moreover, vHIT gain values were lower in the 7 decompensated patients than in the 7 compensated patients.
Comparison of Caloric Test and vHIT Results in 7 Decompensated and in 7 Randomly Selected Compensated Patients.
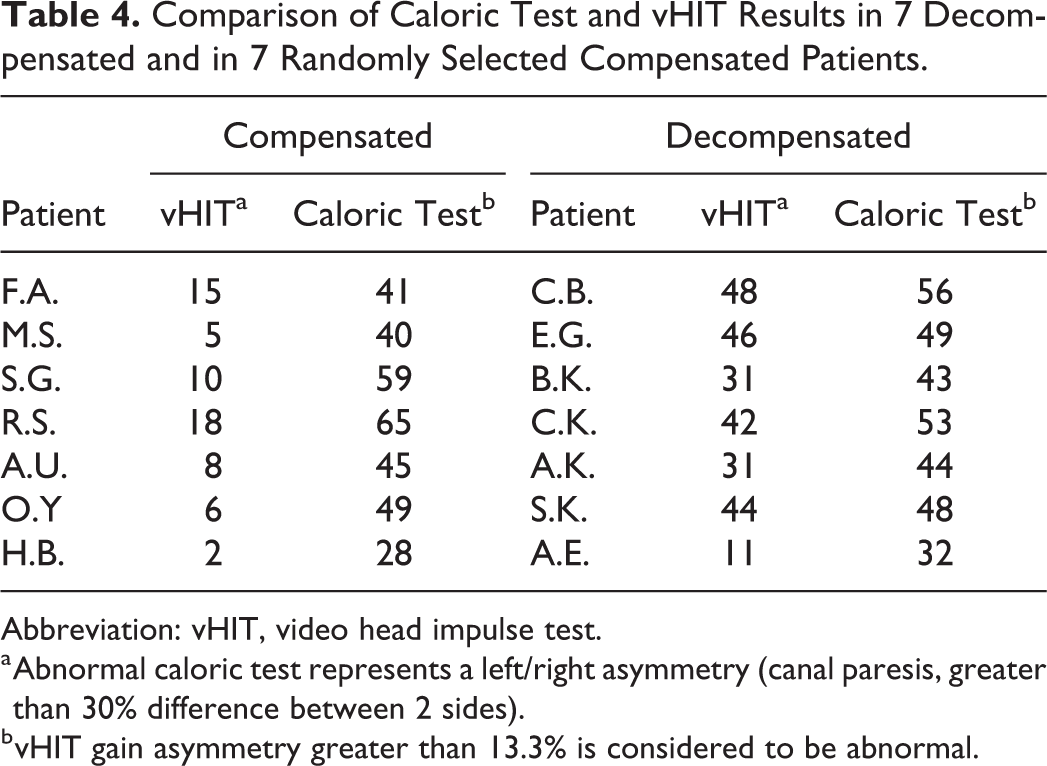
Abbreviation: vHIT, video head impulse test.
a Abnormal caloric test represents a left/right asymmetry (canal paresis, greater than 30% difference between 2 sides).
b vHIT gain asymmetry greater than 13.3% is considered to be abnormal.
In addition, we have studied a small subgroup of patients diagnosed with acoustic neuroma. The values of gain asymmetry based on CT and vHIT were presented in Table 5. The vHIT and CT values for the first patient showed vestibular hypofunction. Even though for the second and third patients, CT displayed the existing hypofunction, and vHIT was not able to demonstrate hypofunction.
Comparison of Caloric Test and vHIT Results in the Patients Diagnosed With Acoustic Neuroma.
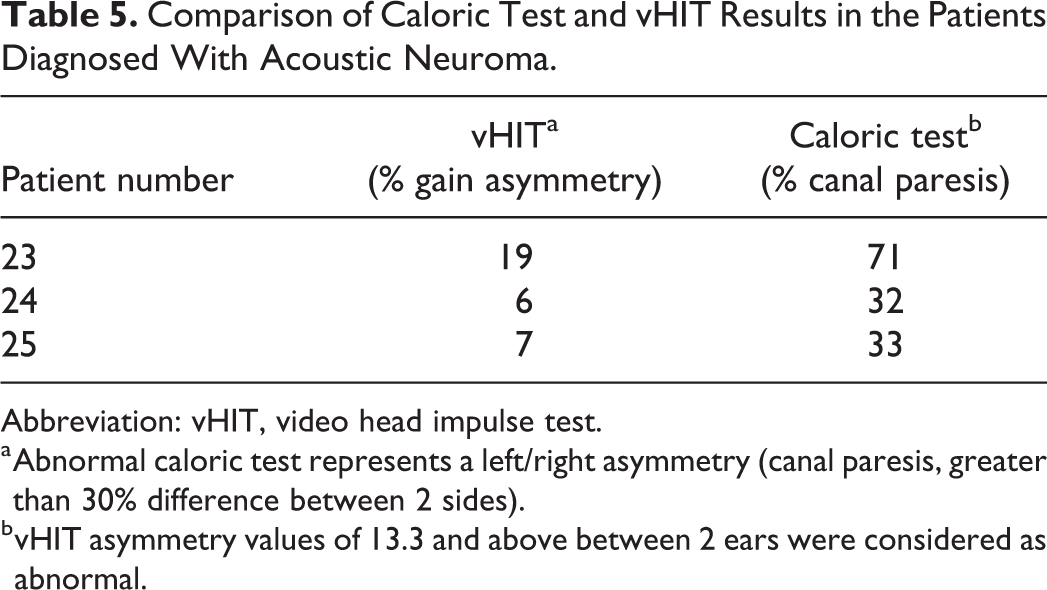
Abbreviation: vHIT, video head impulse test.
a Abnormal caloric test represents a left/right asymmetry (canal paresis, greater than 30% difference between 2 sides).
b vHIT asymmetry values of 13.3 and above between 2 ears were considered as abnormal.
Discussion
The head impulse test was first described by Halmagyi and Curthoys in 1988. 4 In 2009, MacDougall et al 5 developed a video method of testing function of each of the 6 canals individually. Video head impulse test tests all 6 canal functions at high frequencies, whereas caloric test evaluates low frequencies and only lateral semicircular canals. Their results showed that vHIT yields similar diagnostic accuracy to caloric test in the early stages with spontaneous nystagmus. There is an increasing tendency to use vHIT in otolaryngology clinics in recent years after its popularization due to its ease of use, easy tolerability, practicality, and its applicability even at the bedside.
In this study, a caloric test was performed with water. Although Bell et al 10 used air caloric stimulation to compare vHIT, Barros and Caovilla 11 suggested that the caloric test with water should be preferred due to its stronger response than air caloric stimuli. The American National Standards Institute does not accept the air caloric test as a standardized method.12,13 Thus, only caloric tests with water were performed in this study.
Considering the caloric test, the accepted limit (cutoff value) of the caloric test differs in many studies. Some studies accept 25% and above as pathological.7,14,15 McCaslin et al 9 accepted much higher values as meaningful and they stated that asymmetry should exceed 40% to be meaningful and 25% asymmetry was not important enough for referring canal paresis and could be misleading.
Mahringer and Rambold 7 reported that a 39.5% caloric asymmetry is more consistent with the vHIT results obtained. However, our experience in our department demonstrated that 30% caloric response difference was in accordance with 0.79 (borderline normal) vHIT results. Therefore, our department has accepted 30% or above as the cutoff value in our caloric tests, and we used the same cutoff value in this study as well.
Regarding vHIT, McCaslin et al 9 accepted gain values of 0.79 to 1.20 as normal, and they considered gain asymmetry values of 13.3 and above between ears of the same individual as abnormal. We also used the same values for normal and abnormal gain asymmetry values.
No significant effect of age and gender on vHIT and caloric tests was found in accordance with literature. 16 The decompensated group consisted of 7 patients. The caloric test results were abnormal and pathologic in all these patients whereas only 6 of 7 of these patients showed abnormal vHIT results. Both vHIT and caloric test asymmetry percentages were similar (Table 4) in the determination of the affected side and the degree of pathology in the acute stage and represent equally reliable results in patients with acute peripheral vestibular attacks. These results are in accordance with Mahringer and Rambold 7 and Bartolomeo et al 17 studies.
Bartolomeo et al 17 reported that both vHIT and caloric tests were found abnormal in patients with acute unilateral vestibular neuritis at the time of diagnosis. One month later, 13 of (40%) the 29 patients had mild caloric deficits, while vHIT values returned to normal in all patients. In 12 of 29 patients, severe caloric deficits were found (62.5% or more) and all patients had abnormal vHIT values. Four patients had moderate (40%-62.5%) caloric deficit and 2 (50%) of these patients had abnormal vHIT results. In 12 of 29 patients, severe caloric deficits were found (62.5% or more) and all patients had abnormal vHIT values. So VHIT decreased to normal values in 15 (51.8%) of 29 patients, whereas only in 8 of 29 patients caloric test results returned to normal. 17 In a similar study, Mahringer and Rambold 7 found 63% vHIT positivity in the acute group (symptoms occurring within the last 5 days) and 33% vHIT positivity was found in the non-acute disease group (symptoms started more than 5 days before). 7 However, bi-thermal caloric tests are very disturbing and not tolerable during the hyper acute phase of the peripheric vestibular disease and should not be performed in acute phase. On the other hand, vHIT can be performed during this hyper acute phase, even in patients with spontaneous nystagmus, and therefore, vHIT is considered as a primary evaluation method in the early (decompensated) period of the disease.
The compensated group consisted of 18 patients. Fifteen of 18 patients showed abnormal pathologic results with caloric test, whereas only 3 of 18 patients showed abnormal pathologic results with vHIT. Our results were consistent with other studies.18-20 If we had used vHIT as a sole diagnostic test, we would have misdiagnosed 15 of 18 patients in the compensated group. Similar results were given in the study of Burston et al. 18 According to Burston et al, if only vHIT had been used, 34 of 60 patients with abnormal results in the caloric test would have been overlooked. These results suggest that vHIT may be inadequate in evaluating the compensated vestibular hypofunctional states. This may be because vHIT tests the high frequency losses, and high frequency losses can improve earlier, thus the values of vHIT return to normal earlier than the caloric test. This finding is important and should be emphasized since vHIT has become a routine for diagnosis and follow-up; caloric tests have completely been abandoned in many clinics. Our study shows that vHIT is insufficient in diagnosing compensated peripheral vestibular diseases.
Another important finding of this study was vHIT values were in the normal range in 2 of 3 vestibular schwannoma patients with compensation, whereas the caloric test results were abnormal in all 3 patients. If we had applied vHIT alone, the vestibular schwannoma would be overlooked in 2 of 3 cases. This finding supports our conclusion that vHIT alone may not be sufficient to evaluate peripheral vestibular diseases in the compensated period. However, the values of the caloric tests for the compensated group continued to be abnormal even after the disease symptoms improved until complete recovery.
Tranter-Entwistle et al 19 reported that central compensation occurs due to the slow-growing nature of vestibular schwannomas, and this central compensation decreases the symptoms of the tumor due to pressure on the vestibular nerve. Similar results were obtained in our study to support these findings. In a patient who was admitted with dizziness and diagnosed with a 3.5-mm acoustic neuroma on magnetic resonance imaging (MRI) exam, the vHIT results were normal although the caloric test detected 33% vestibular hypofunction (Table 5). The fact that vHIT values were within the normal limits in these vestibular schwannoma patients suggests that the concept of compensation should be considered as a separate research topic.
Caloric test values of 5 patients who had pathological results at their first test returned to normal during the follow up period. Of these 5 patients, 3 were diagnosed with vestibular neuritis and were treated with corticosteroids and antivirals. Halmagyi et al 21 reported that vestibular neuritis can get better by time in patients who have received early steroid and antiviral treatment. In these 3 patients, improvement in vestibular ipsilateral VOR was also noted.
One other patient of these 5 patients with complaints of vertigo and hearing loss was diagnosed with perilymphatic fistula. The exploratory tympanotomy was performed immediately and the perilymphatic fistula at the oval window was diagnosed and repaired. Postoperative hearing loss and dizziness improved completely. Another patient who was diagnosed with Meniere disease and treated with acetazolamide and betahistine is still in remission. Therefore, complete recovery of these 5 patients led to normal caloric test results.
Difference of the caloric test values between control and compensated groups and compensated and decompensated groups were statistically significant. However, vHIT gain asymmetry values showed no statistically significant difference between compensated and control groups (Table 3). These results suggest that vHIT is insufficient compared to caloric test in determining the compensatory, chronic vestibular hypofunction status implying that caloric test is superior to vHIT in the evaluation of the compensated patients.
Khater and Afifi 8 suggested that vHIT’s ability to detect unilateral peripheral vestibular pathologies may be used in diagnosis and follow-up of Meniere disease and vestibular neuritis. Our results do not support this statement; although vHIT values of the compensated patients return to normal, caloric tests continue to be asymmetric in the long term. Therefore, using vHIT for follow-up in these diseases could be misleading. However, this finding may be interpreted as improvement/compensation.
Conclusion
In the early decompensated stages of vertigo patients with spontaneous nystagmus, vHIT shows similar diagnostic accuracy to caloric test and should be preferred over caloric test during acute phase. vHIT may be inadequate in evaluating the compensated vestibular hypofunctional states after compensation has been restored. Video head impulse test does not provide reliable results in diagnosis of slow developing, long-standing compensated cases as in acoustic neuroma. Using only vHIT may lead to overlooking of vestibular schwannoma cases. The proposal to use vHIT in follow-up of peripheric vestibular pathologies is not supported due to normal vHIT values in these patients. However, normal vHIT results may be interpreted as improvement/compensation has occurred.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.