
Abstract
Primary leiomyosarcoma of the tongue is a rare malignant mesenchymal tumor with high recurrence rate and metastatic potential. Through analysis of one case condition and literature review, this paper discusses the clinical characteristics and treatment methods and recommends that expanded resection surgery should be the first intervention. Postoperative adjuvant radiotherapy and combined chemotherapy should be administered if the case specifically requires such an approach.
Introduction
Leiomyosarcoma is a malignant tumor of the smooth muscle cells or their mesenchymal precursor cells. It is most common in the uterus, gastrointestinal tract and retroperitoneal cavity. 1 Leiomyosarcoma is an aggressive and rare soft tissue sarcoma, and has one of the highest mortality rates for head and neck sarcomas. 2 The oral cavity (22%), nasal cavity (19%), and face and neck (17%) are the most common sites of leiomyosarcoma in the head and neck 3 ; it is more common in intra-buccal areas than in the tongue. Primary leiomyosarcoma of the tongue is an extremely rare mesenchymal malignancy with high recurrence rate and metastatic potential. 4 Leiomyosarcoma has been associated with loss of chromosome 13, decreased expression of p16 and Epstein-Barr virus infection, amongst other factors, all of which require further study to understand the mechanisms leading to disease.
Sarcomas of the head and neck often present with non-specific signs and symptoms, and in the majority of cases these tumors manifest as painless masses. These can therefore be misdiagnosed as benign lesions. Surgery followed by radiotherapy is the most common course of treatment 5 as local recurrence and metastasis is not uncommon in oral smooth muscle tumors. Due to the low incidence and atypical symptoms, prognosis varies greatly. Additional reports of this disease will help increase the understanding and aid diagnosis. This paper reports a case of leiomyosarcoma on a child’s lingual dorsum, discusses the characteristics of pathogenesis and diagnosis, treatment and prognosis based on other findings in the literature.
Materials and methods
Ethical approval and informed consent
All procedures undertaken in research involving human participants comply with the ethical standards of the institution and/or the National Research Council and the Declaration of Helsinki of 1964 and its subsequent amendments or similar ethical standards. Informed consent was obtained for all individual participants in the study.
Case report and literature review
In this paper, we report a 6-year-old female case of primary leiomyosarcoma. A Medline literature search on PubMed was performed, using key words “leiomyosarcoma, tongue” which yielded 56 articles. A total of 17 articles were included based on primary coverage and relevance to this report (Figure 1). Flowchart.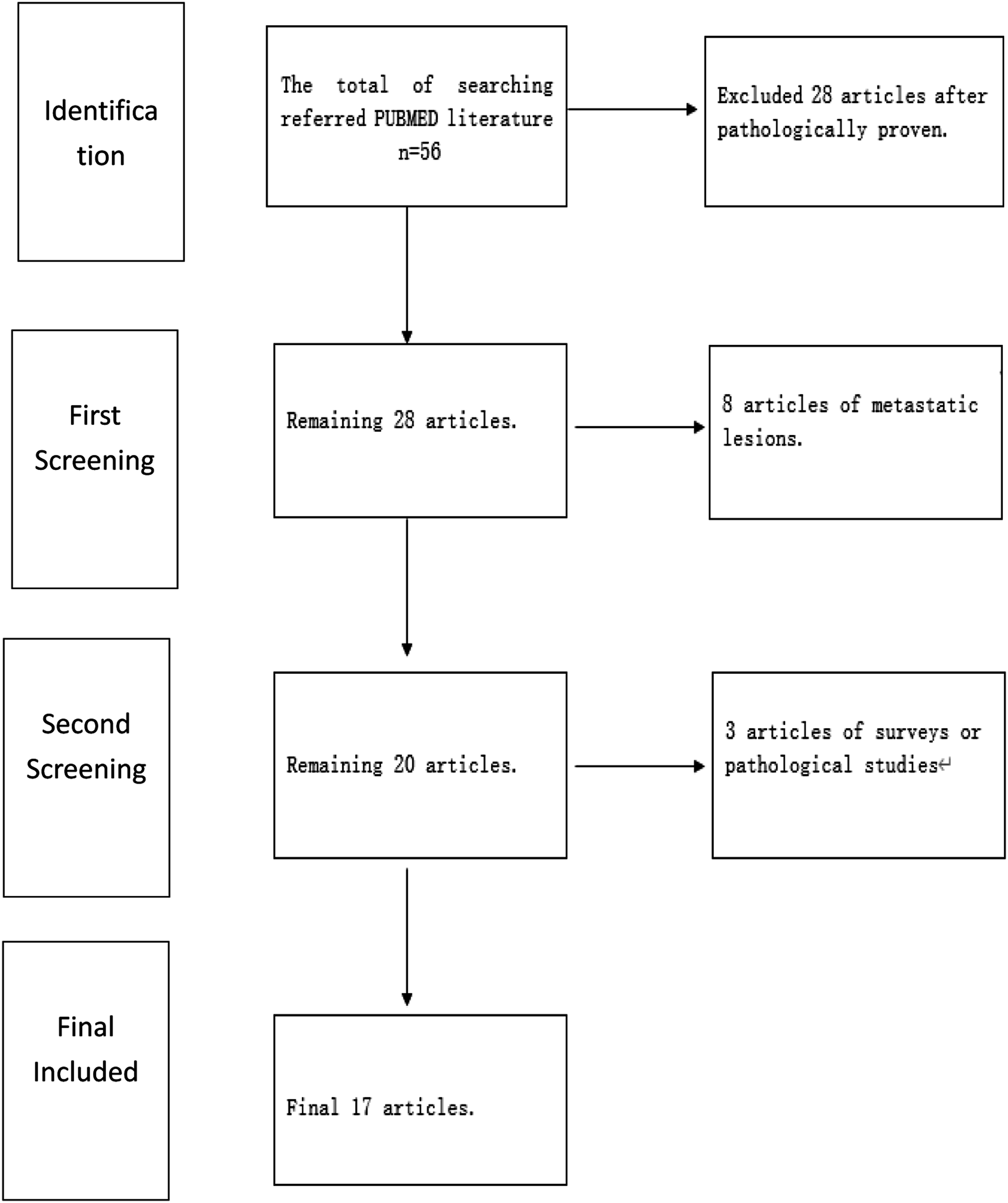
Results
Case report
A 6-year-old female patient presented at ___ Hospital with a raised mucosal growth over the lingual dorsum on the rear of sulcus terminalis linguae. The patient reported that this had been present for one month prior to hospital admission. No discomfort or symptoms were reported. The growth was approximately 1.5 cm in size and the patient had begun to feel uncomfortable when eating, therefore came to hospital for investigation.
The growth was located on the sulcus terminalis linguae′ was pink in color, was completely within the mucosa and had a clear margin. Upon palpation the mass was solid with a slightly hard base and no tenderness. No palpable enlarged lymph nodes were apparent in the neck (Figure 2A). Preoperative enhanced magnetic resonance imaging examination revealed excessive blood supply to the solid lesion tissue of the tongue (Figure 2B, C), and the margin of the surrounding tissue was still clear. (Figure 2). (A) Preoperative intraoral tumor (arrow), (B) Horizontal, T2 phase, tumor located at lingual root, high signal, (C) Coronal, T2 phase, clear margin of tumor.
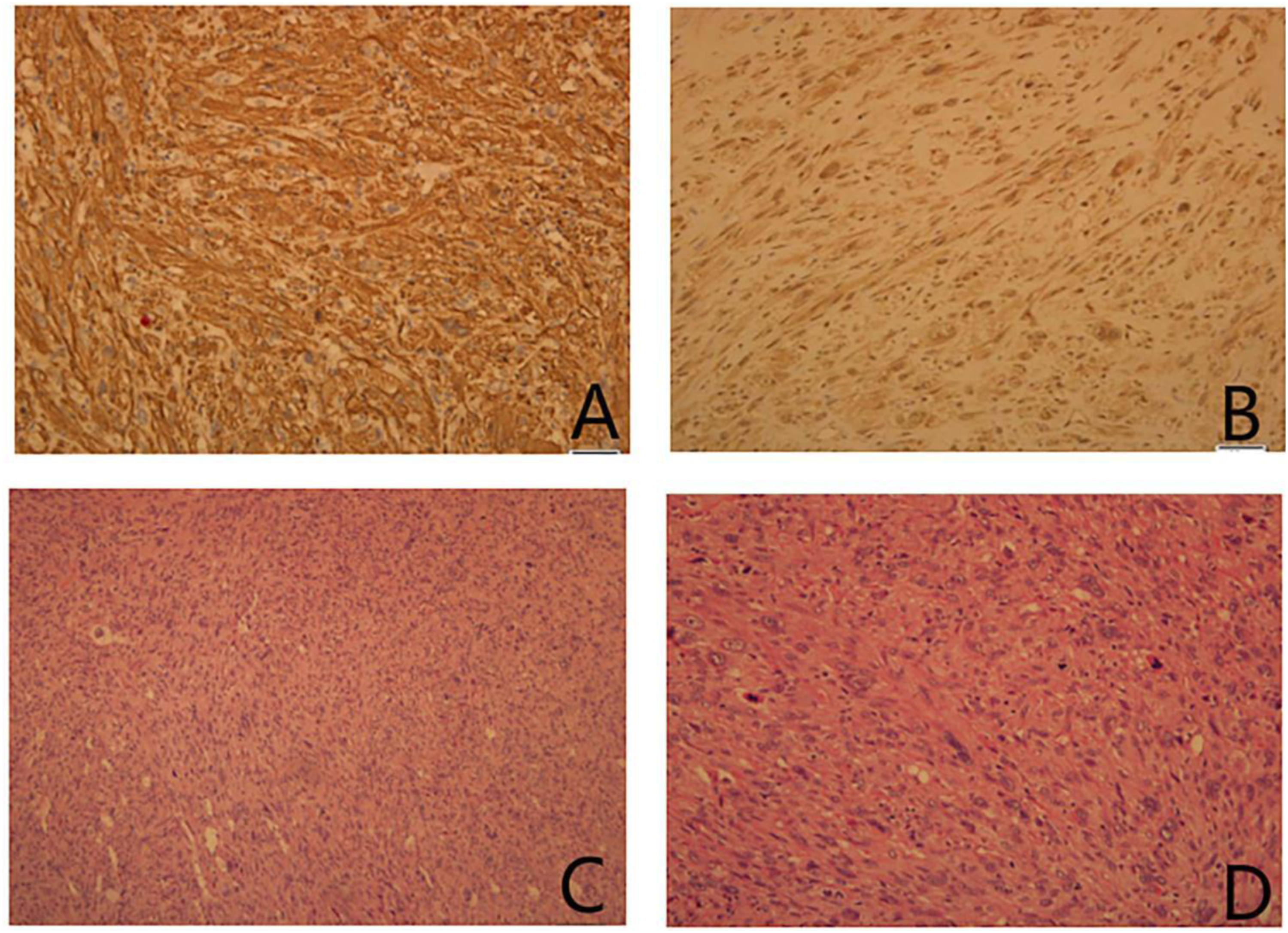
The preoperative diagnosis was a tongue tumor with unclear nature, and an exploratory excision biopsy was performed under general anesthesia (Figure 3). Evaluation of the sample revealed that the pathology should be identified following the surgery, and therefore no extended resection was performed at that time. The postoperative pathology and immunohistochemistry results confirmed that the sample was a leiomyosarcoma (Figure 4). A second resection was performed which was expanded by 1 cm to remove additional lesional tissue and to create a clear margin. No chemoradiotherapy was performed postoperatively, and the prognosis of the patient was good after 2 years of follow-up. The intraoperative situation of the first surgery. (A) Spindle cells with vesicular cytoplasm. (B) Areas of spindle cell proliferation. (C) Low power view of main lesion. (D) Numerous mitotic figures (arrow).
Literature review of leiomyosarcoma
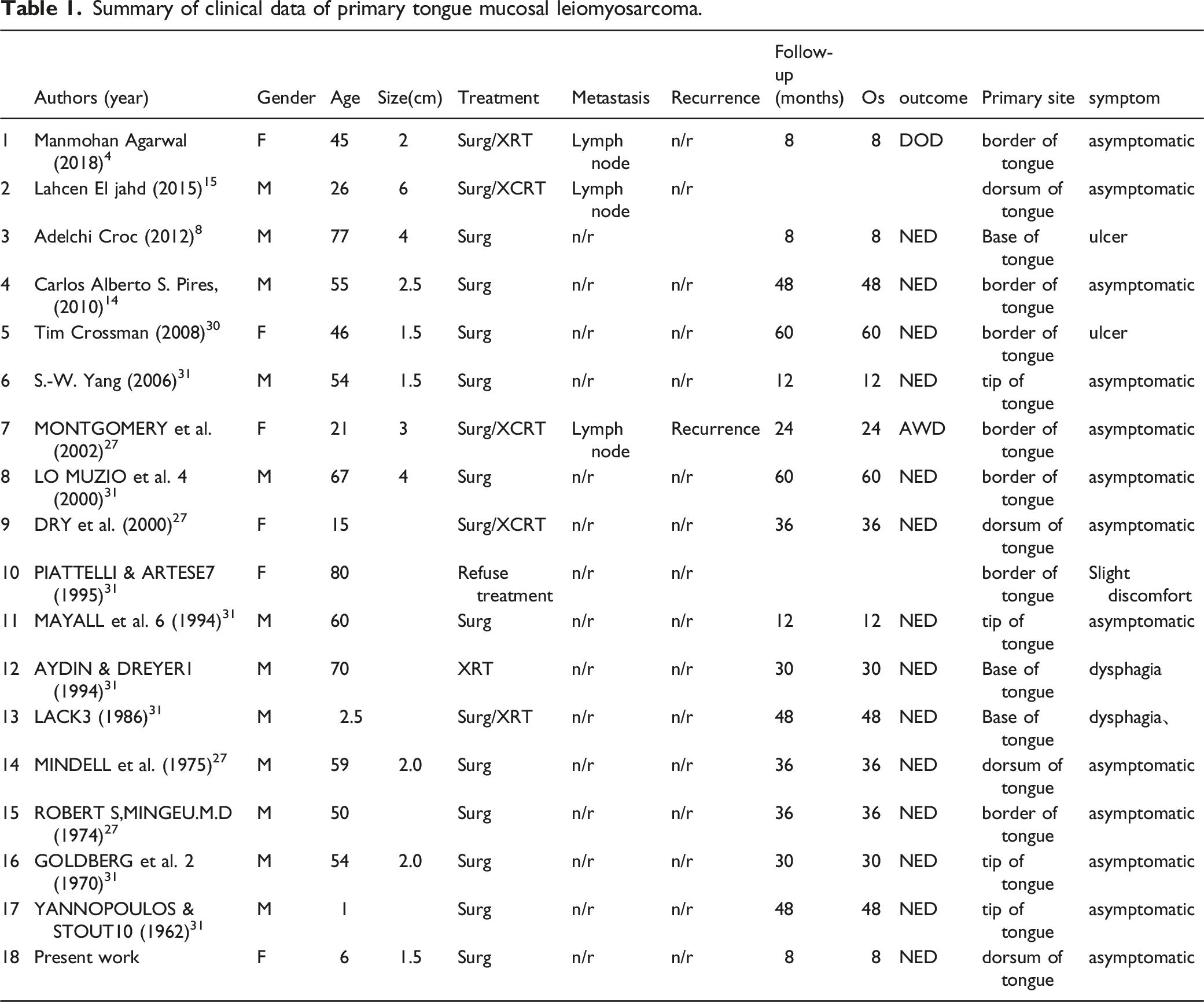
Summary of clinical data of primary tongue mucosal leiomyosarcoma.
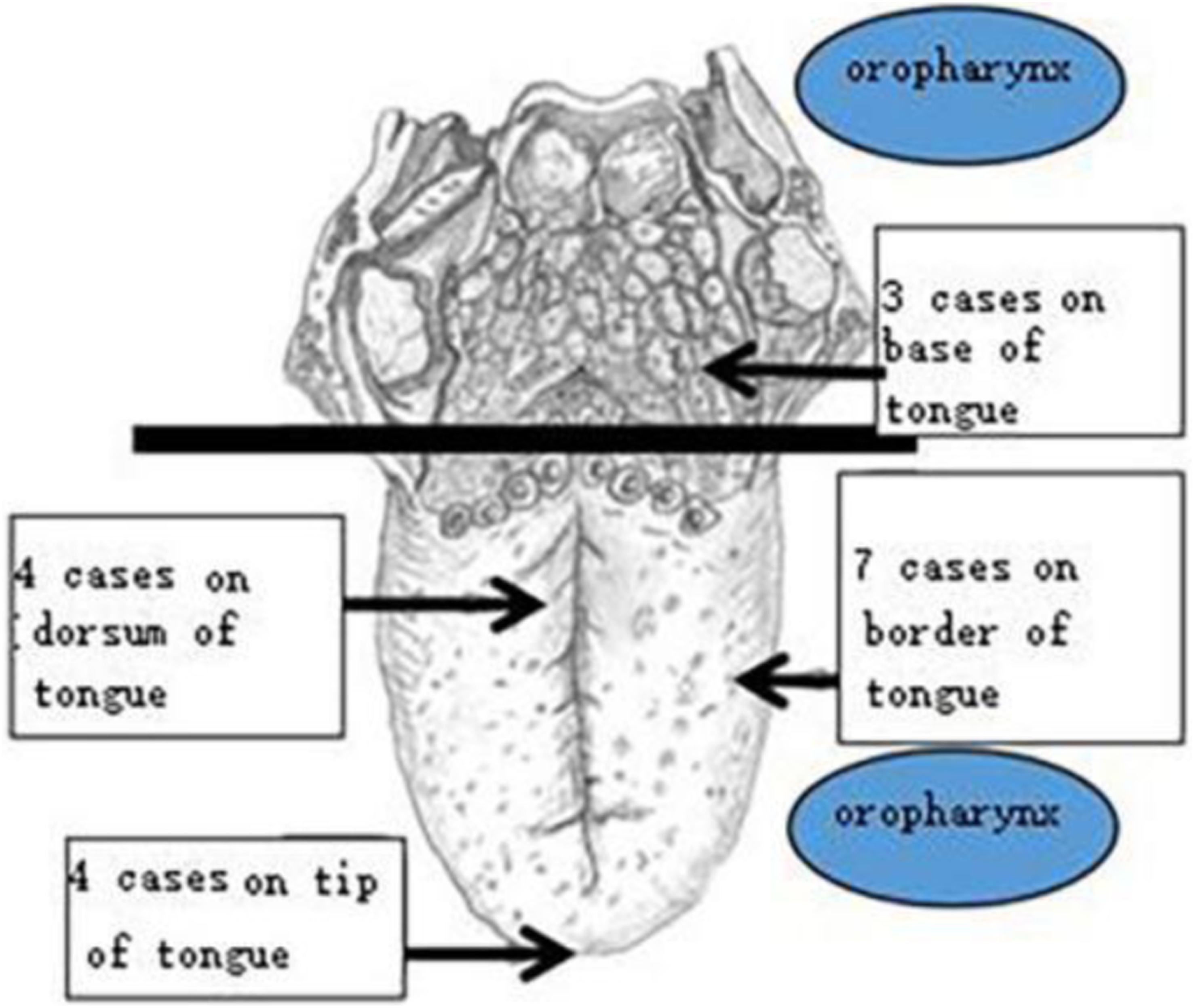
The literature-reported locations of primary tongue leiomyosarcoma.
Our patient was treated with expanded surgery of 1 cm over two years, and there was no chemoradiotherapy administered after the surgery. No recurrence has been identified to date, however the rarity of the disease means that no definitive prognosis can be anticipated at this point, or that the prognosis for pediatric patients with primary tongue leiomyosarcoma is better than patients with tumors of oral origin.6,7 Though the case numbers are low and literature scarce, there is some evidence to suggest that successful resection of the tumor with post-surgical radiotherapy or chemotherapy could provide an excellent prognosis for patients. 8 However, clearly this disease requires further investigation and long-term postoperative follow-up of patients.
Discussion
Leiomyosarcomas, which occur in the jaw and oral tissues, are thought to originate from the vascular media, contoured papilla, or multipotent mesenchymal cells 9 of the smooth muscle.
Leiomyosarcoma is a highly invasive tumor primary tongue with high recurrence rate and metastatic potential, and accounts for 5-10% of all soft tissue sarcomas. It is most commonly reported in the peritoneum, and rarely in the oral cavity. Rarer still is occurrence on the tongue and oral tissue.10 -12 Due to the lack of smooth muscle in the head and neck, this disease rarely occurs in this area, but currently accounts for approximately 4% of whole body leiomyosarcomas. 15 The proportion of soft tissue sarcomas of the head and neck is approximately 1%-4%. Of the reported cases of leiomyosarcoma of the head and neck, the majority involve skin and soft tissue, with only a few cases involving the oral cavity (5.7%) and even fewer cases involving the skull and mandible (0.7%). 13 It is relatively common on the oral inner cheek but rare on the tongue. 11 Cases can be easily misdiagnosed due to being clinically asymptomatic, with only a raised tongue growth, no uncomfortable symptoms, and given that it needs to be identified by postoperative pathology and immunohistochemistry.
Diagnostic requirements for primary tongue leiomyosarcoma are as follows: (1) there is no history of sarcoma in the patient, (2) current sarcomas are not metastatic, (3) macroscopic manifestation is consistent with the source being smooth muscle, (4) exclude carcinosarcoma, (5) histologic examination and immunohistochemical staining are essential. 14 Immunohistochemical identifications of desmin, vimentin, actin and myoglobin are helpful in diagnosis. 15
Leiomyosarcomas of the head and neck are more aggressive and generally have a worse prognosis than leiomyosarcomas of the uterus or gastrointestinal tract. 16 Adjuvant/neoadjuvant chemotherapy or radiotherapy for head and neck sarcomas had no significant effect on disease-free survival, especially overall survival. Radiotherapy or chemotherapy without surgical treatment of patients is highly unlikely to eliminate the disease; aggressive surgical intervention remains the main method of management for patients with localized sarcomas of the head and neck. 17 Leiomyosarcoma of head and neck is locally invasive and has a poor prognosis. 18 Local extended resection is the preferred treatment, and some reports suggest a surgical margin between 2 and 5 cm is necessary.19 -21 However, current studies show that the resection range can be controlled to between 0.5 and 1 cm if adjuvant radiotherapy is used. 22 Neck dissection is not necessary for cN0, 23 the main treatment modes for occurrence at this site were surgical resection and postoperative radiotherapy, 5 adjuvant radiation is recommended whether surgical margins are positive or not. 24 As for chemotherapy, this should be considered on a patient-by-patient basis. Some studies suggest that adjuvant chemotherapy plays a significant role in reducing local and distant recurrence. 25 Generally, however, the incidence of lymph node metastasis in sarcomas is low, and neck dissection is performed only for patients with positive lymph nodes. 26 However, oral leiomyosarcoma is different and local lymph node metastasis may be possible. 27 Distant metastases involving the lungs, lymph nodes, scalp, and brain stem may also occur. 5
Tumor diameter & GT of 5 cm, a positive margin, low differentiation status, advanced age, and deep tumor invasion are all adverse factors which negatively impact upon survival time. 28 For oral smooth muscle, local recurrence and metastasis are not uncommon, the primary site of the tumor was a predictor of metastasis. Bony involvement and metastasis were associated with poor prognosis. 29 Typically, surgeons limit the resection scope because of the limitation of anatomic site or the protection of important structures and physical functioning. Overall 5 - and 10-year survival rates for head and neck sarcomas have been reported to be 42% and 20%, respectively. 29 One study reported a 5-year disease-specific survival rate of 87.6% for well-differentiated leiomyosarcoma and 52.7% for non-well differentiated leiomyosarcoma. Local recurrence is the most common cause of death.16,30 This report reviewed and analyzed 41 cases of head and neck leiomyosarcomas, where only two patients (5%) survived beyond the 5-year follow-up period. Compared to lesions in other parts of the head and neck, lesions in the skin, nasal cavity and throat have better prognoses. Oral cavity lesions have poor prognoses due to the limit of anatomical structure. In our literature search, all three reported patients with tongue leiomyosarcoma died within 5 years. 25 Prognosis for leiomyosarcoma therefore is highly dependent on the site.
Conclusion
Expanded resection surgery is the preferred treatment, radiotherapy or chemotherapy may not be necessary when margins are adequate. In particular, leiomyosarcoma of the tongue should be supplemented with radiotherapy where a negative edge is not available. Considering this paper and previous literature reports, prognosis of tongue leiomyosarcoma seems to be reasonable. However, more reporting of cases and follow-up studies are essential.
Footnotes
Author’s contributions
Shaojie Wang: write the article. Changlong Song: write the article. Xinjie Yang: gather the information. Yaowu Yang: organise the materials and summarize the article. Jianhua Wei: provide the case and proofread the article.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors certify that they are not affiliated with or involved in any organization or entity with any financial interest (e.g., honorarium; Education grant; To participate in the spokesman's work; Membership, employment, consulting, share ownership or other equity interests; As well as expert testimony or patent licensing arrangements), or non-financial interests (such as personal or professional relationships, affiliations, knowledge, or beliefs) in the subject matter or material discussed here in.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.