
Abstract
Objective
The current study was conducted to explore the association between laryngopharyngeal reflux disease (LPRD) and refractory chronic rhinosinusitis (RCRS), and to reveal the potential role of LPRD in the development of RCRS.
Methods
A total of 104 patients diagnosed as chronic rhinosinusitis (CRS) and hospitalized, as well as 50 healthy participants were enrolled into this study. Among patients enrolled, 53 were RCRS and 51 were CRS. All participants were assessed with reflux symptom index (RSI) and reflux finding score (RFS). Patients with RSI >13 and/or RFS >7 were diagnosed as LPRD. In addition, pepsin in the nasal secretions from the middle meatus tract complex at fasting in the morning was analyzed using ELISA. Patients with pepsin concentration of >75 ng/ml was considered as positive, and confirmed as LPRD.
Results
There was no significant difference in age, sex, height, and weight among RCRS, CRS, and control groups. The positive rates of RSI and RFS scores were 39.6% in the RCRS and 52.9% in the CRS, respectively, which were significantly higher than that of the control group (14.0%, P < 0.05), respectively. Significantly higher positive rate of pepsin assay was also observed for RCRS(43.4%) and CRS(64.7%) when compared with the control group (18.0%, P < 0.05). The positive rate of pepsin assay was strongly associated with the positive rate of RSI or RFS (P < 0.001).
Conclusion
The present findings have important implications that RSI and RFS score was highly associated with pepsin assay result in the patients with RCRS or CRS. We confirmed the importance of RSI and RFS scoring system as well as pepsin test, which may offer insight for clinical screening for LPRD among CRS patients.
Introduction
Chronic rhinosinusitis (CRS) is a common chronic inflammatory disease of nasal sinuses and nasal mucosa in otorhinolaryngology, with an overall incidence of 5%-12% worldwide,1-3 and 2%-8% in China.4-6 The current treatment options for CRS includes conservative medical treatment and surgery. However, among patients who receive the standardized surgery and medical treatment, some still suffer from symptoms and inflammatory reactions of sinus mucosa, including edema, hypertrophy, granulation tissue formation, polyp formation, and purulent secretion, which is defined as refractory chronic rhinosinusitis (RCRS). 7 Refractory chronic rhinosinusitis has high recurrence rate and prolonged healing process following standardized treatment, which leads to reduced quality of life and economic burden of the patients. Pathophysiological mechanism of RCRS is still to be established. Studies have shown that laryngopharyngeal reflux disease (LPRD) is closely related to CRS, with 37%-72% in the incidence of LPRD in patients with CRS. 8 Chambers et al 9 found that most of the CRS patients with poor treatment outcome were accompanied by pharyngeal reflux (LPR) symptoms, and speculated that LPR may be one of the risk factors affecting the curative effect of sinusitis surgery.
The in-depth study of LPRD has confirmed the important role of pepsin in the damage of pharynx and larynx, nasal cavity, and paranasal sinus mucosal injury caused by gastric content reflux. Pepsin is hence considered to be a reliable marker of laryngopharyngeal reflux (LPR), and pepsin test is often applied as an ideal tool to help diagnose LPRD.10,11
Since the potential involvement of immunity in the development of RCRS, great focus has been laid on relevant factors of the occurrence and development of RCRS in the field of nasal science. However, limited studies exist concerning the relationship between RCRS and LPRD. Therefore, we sought to investigate whether there is an association between LPRD and RCRS by assessing reflux symptom index (RSI) and reflux finding score (RFS), as well as quantifying pepsin amount in the nasal secretions, with an attempt to provide ideal candidate for the clinical diagnosis and treatment of RCRS.
Materials and Methods
Participants
Patients harboring chronic sinusitis and admitted into our hospital were enrolled into this study from September 2018 to December 2019. Fifty healthy volunteers who underwent physical examination in our hospital during the same period were selected as the control group. This study protocol was approved by our hospital, and all participants signed informed consent.
Inclusion Criteria
(1). Patients met the diagnostic criteria of the CRS and RCRS defined by the Executive summary of EPOS 2020 including integrated care pathways 12 ; (2). Patients had at least one of the following symptoms: sore throat or discomfort in the throat, globus sensation (foreign body sensation in the throat), pharyngeal itching with irritation cough, dysphagia (difficulty in swallowing food, water, or tablets), constant throat clearing, hoarseness, or dysphonia.
Exclusion Criteria
(1). Mental illness; (2). Congenital malformation of esophagus; (3). Immunodeficiency diseases; (4). Severe systemic diseases; (5). Posterior nostril polyp, allergic fungal sinusitis, nasopharyngeal fibroangioma, sinonasal inverted papilloma, nasal cavity and paranasal sinus malignant tumor, and patients with history of radiotherapy or chemotherapy; (6). Patients with diseases caused by Helicobacter pylori (HP) infection including chronic gastritis, gastric ulcer, and gastric cancer; (7). History of glucocorticoids, anti-acid drugs, or antibiotics in the past 2 months.
Assessment of Laryngopharyngeal RSI and RFS
(1). Laryngopharyngeal RSI: all participants were assessed using RSI following the guidelines proposed by Belafsky et al. 13 Based on the 6-level scoring method of 0-5 points, each RSI symptom was scored from 0 (no compliant) to 5 (severe compliant). Prior to the evaluation, a dedicated physician explained the levels of the scale system to the patients in detail. In order to avoid the bias, it was not allowed to induce the participants in answering questions. The participants were preliminarily considered LPRD based on RSI if the total score was more than 13.
(2). Laryngopharyngeal RFS: all participants were examined with electronic fiber laryngoscope by 2 otorhinolaryngologists, who both had at least 3 years of clinical experience. The RFS was assessed following the guidelines proposed by Belafsky et al. 14 The participants were preliminarily considered to have LPRD if the RFS total score was more than 7.
Pepsin Quantification
Pepsin was quantified using ELISA--a commercially available kit (Jiangsu MeiAn Pharmaceutical Co., Ltd., Jiangsu, China). Briefly, 1-3 ml nasal secretion of the middle meatus tract complex was collected from each participant at fasting in the morning, and stored at liquid nitrogen for further pepsin quantification based on the manufacturer’s instruction.
Statistical Analysis
All statistical analyses were performed using SPSS 22.0 statistical software to process the data. Variables such as age, gender, and height and weight were tested for normal distribution using one-way ANOVA, Chi square test, and Kruskal Wallis h test, respectively. Chi square test and consistency kappa test were used to compare the rates. A P < 0.05 was considered statistically significant in all comparisons.
Results
Demographic Characteristics of the Patients.
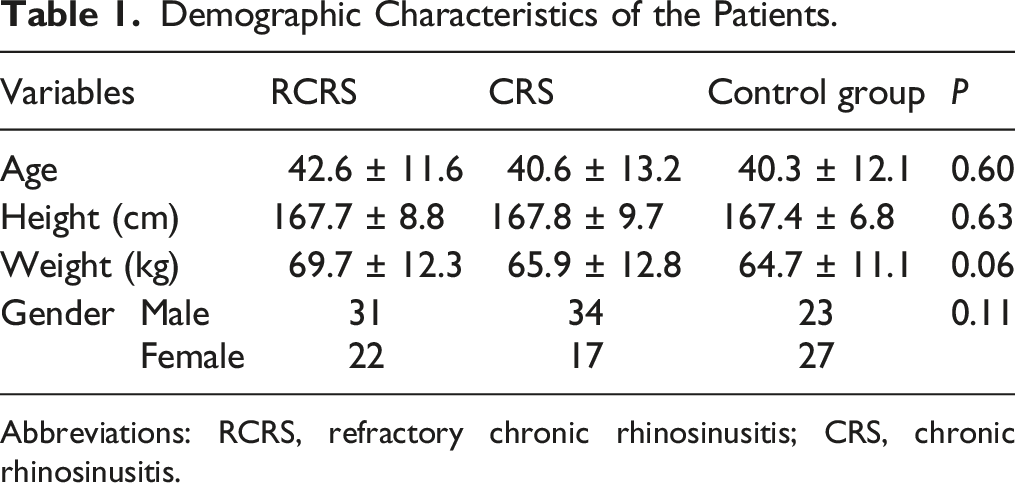
Abbreviations: RCRS, refractory chronic rhinosinusitis; CRS, chronic rhinosinusitis.
Comparison of RSI and RFS Scores in the Diagnosis of LPRD.

Abbreviations: RSI, laryngopharyngeal reflux symptom index; RFS, laryngopharyngeal reflux finding score; LPRD, laryngopharyngeal reflux disease; RCRS, refractory chronic rhinosinusitis; CRS, chronic rhinosinusitis.
Comparison of Pepsin Test.
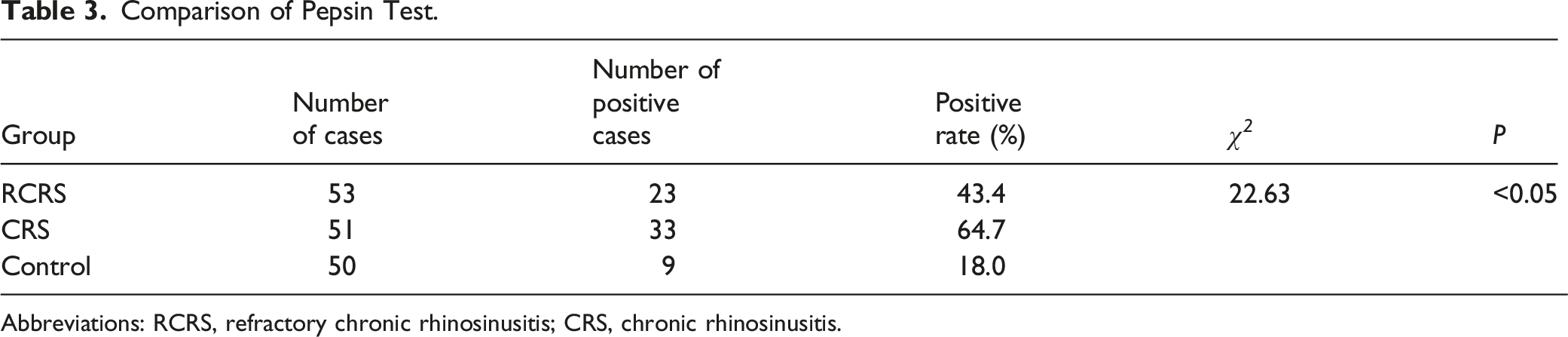
Abbreviations: RCRS, refractory chronic rhinosinusitis; CRS, chronic rhinosinusitis.
Consistency of Pepsin Test and RSI, RFS Score in the Diagnosis of Pharyngeal Reflux.
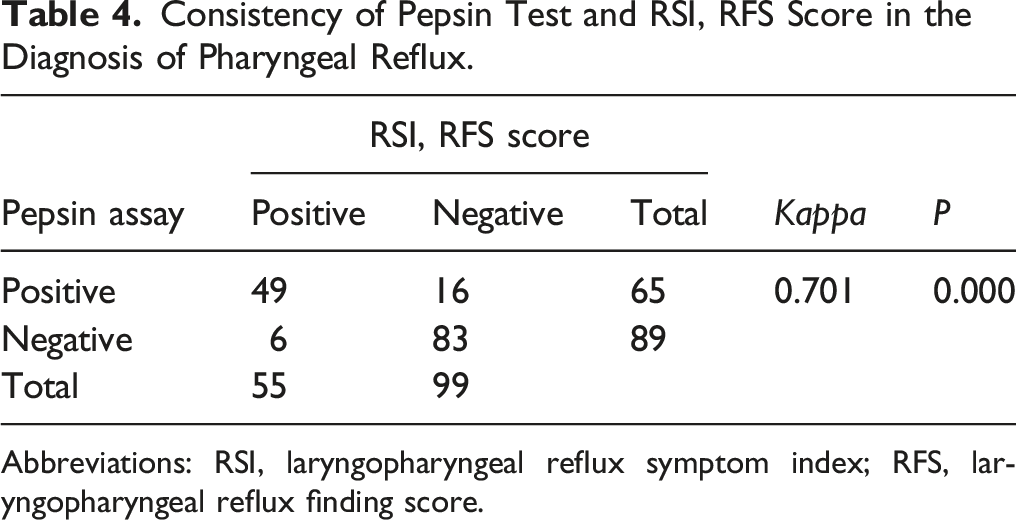
Abbreviations: RSI, laryngopharyngeal reflux symptom index; RFS, laryngopharyngeal reflux finding score.
Discussion
Although the exact pathogenesis of LPR is unknown, several studies have been implicated in the high incidence of LPR and gastroesophageal reflux (GER) in patients with CRS or RCRS.8,15,16 These results are compatible with our current study that the positive rate of RSI and RFS, and positive outcome of pepsin assay were significantly higher in the patients with RCRS or CRS compared to control group, suggesting that patients with RCRS or CRS had a higher incidence of LPR.
Chronic rhinosinusitis is thought to be involved in infection, allergy, abnormal anatomy of nasal cavity and sinuses as its major pathogenic factors. In addition, environmental factors, genetic factors, mucosal ciliary dysfunction, and poor systemic immune function may contribute to the development of CRS, which often causes symptoms such as nasal congestion, head heaviness, mucopurulent runny nose, headache, and anosmia, with a long course of disease and frequent recurrence. Some CRS patients may become refractory to standardized treatment of surgery and medicine, resulting in stress, large economic burden, and reduced quality of life of patients.
Laryngopharyngeal reflux refers to the general name of reflux reaching above the upper esophageal sphincter, causing corresponding throat symptoms and pathological signs, 17 which is closely related to many otorhinolaryngology diseases. The main clinical manifestations are globus sensation (foreign body sensation in throat), continuous throat clearing, throat pain, and chronic cough. The signs of LPR under fiber laryngoscope mainly include mucosal thickening in the posterior commissure area, vocal cord congestion and edema. 18 Since the symptoms of LPR are lack of specificity, diagnosis of LPR is difficult to determine in clinical practice. At present, the differential diagnosis of LPR include the following methods: (1) 24-h pH-Impedance test of esophagus and laryngopharynx, (2) RSI and RFS scoring, (3) pepsin detection, and (4) gastroscopy. Of them, the 24-h pH-Impedance test of esophagus and laryngopharynx is the gold standard for the diagnosis of LPR, but it is an invasive procedure, and the false positive rate of this method varied from 7% to 17%.19,20 However, studies have demonstrated that 24-h pH-Impedance test is a reliable method for the diagnosis of LPR. In this regard, Desjardin et al reported that pharyngeal pH alone was not reliable for the detection of pharyngeal reflux, and depicted that the only reliable analysis should take into account impedance patterns demonstrating the presence of pharyngeal reflux event preceded by a distal and proximal reflux event within the esophagus. 21 Recently, a study by Vance et al compared 24-h pH-Impedance testing and pharyngeal Probe (Restech) testing. 22 They found that RIS score of patients were better correlated with 24-h pH-Impedance test than with Restech for percent time spent in both upright and supine position, while Restech was better correlated with total patient symptom scores including cough, heartburn, burping, and throat clearing. It was also suggested that Restech detected more percent time in reflux for total reflux, supine reflux, and upright reflux, and that it detected longer event times than Impedance. 22
Reflux symptom index and RFS score systems are two scales proposed to evaluate clinical manifestations and signs of LPR,13,14 which is of great significance for the diagnosis and treatment of the disease. Patients with RSI >13 and/or RFS >7 could be diagnosed as LPR.23-27 Here in the current study, RSI and RFS score system was applied and positive rates of these parameters were analyzed in the patients with RCRS or CRS. We found that positive rates of both RSI and RFS scores were significantly higher in the patients with RCRS or CRS, and that positive rate of RSI and RFS scores were significantly correlated with the positivity of pepsin assay, suggesting these two parameters may have a role for the diagnosis of LPR among patients with CRS or RCRS.
Pepsin quantification in the content of nasal secretion from CRS patients was used for the confirmation of LPR with fairly high sensitivity (95.5%) and specificity (66.67%).28-30 It has also been reported that pepsin was not detected in the biopsies of nasopharynx of 20 patients with drug and surgical refractory CRS, while the presence of pepsin was detected in the nasal lavage fluid in 5 of the 20 patients, but not in the control group, indicating the reflux of gastric contents reached the nasal cavity and paranasal sinuses. 31 Furthermore, Li et al 32 tested pepsin in 35 CRS patients (11 of them underwent surgical treatment due to abnormal nasal anatomy), and found that the positive rate of pepsin assay in the CRS patients was significantly higher than that in the control group, indicating that LPRD may be related to the occurrence of CRS. Based on our study, the positive rate of pepsin test in the RCRS or CRS groups was significantly higher than that in the control group, indicating that pepsin assay could be used for assisting the diagnosis of LPR in the patients with CRS or RCRS. These results are compatible with previous study by Ozmen et al. 29 However, our study found that the positive rate of pepsin assay in the patients with RCRS was lower than that in the patients with CRS. In contrast, a higher incidence of pepsin positivity in the pharyngeal reflux of patients with postoperative recurrence of CRS was found by others. 29 However, these studies have methodological differences. Considering the small sample size and combined influence of multiple factors such as regional differences in research objects of our study, there may be bias. In addition, it is noteworthy that pepsin was found in some nasal secretions of the control group in this study with positive test results, indicating that patients without CRS may also have pharyngeal reflux.
It has been reported that the incidence of LPR in patients with CRS was 37%-72%. 8 Consistently, the positive rate of pepsin test in the CRS group of this study was 64.7%. These findings suggested that LPRD may play an important role in the pathogenesis of CRS. Although the mechanisms of CRS caused by LPRD remains to be further defined, the following mechanisms are thought to be involved. (1). Under normal circumstances, the esophageal mucosa can produce carbonate to neutralize the gastric acid and pepsin in the reflux, so as to reduce the damage to the esophageal mucosa. However, with the lack of carbonate in the nasopharynx and laryngopharynx, even a small amount of gastric acid and pepsin can directly cause irreversible damage to the upper airway mucosa, stimulate the nasal cavity and paranasal sinus mucosa, resulting in mucosal edema, ciliary clearance dysfunction, and nasal sinus opening obstruction causing secondary infection. (2). Neurogenic mechanism mediated by vagus nerve: reflux of gastric contents can cause the disturbance of autonomic nervous system, which further leads to nasal cavity and paranasal sinus mucosal edema, as well as blockade of the drainage of paranasal sinus. (3). Helicobacter pylori infection: HP, a gram-negative bacilli that exists in the epithelium of gastric mucosa, was found in nasal polyps of 23 patients with CRS and GER of all 6 patients with symptoms of gastroesophageal reflux diseaseGERD, whereas HP was not detected in the control group. 33
In conclusion, LPR may be a risk factor for RCRS, and it is related to CRS. Patients harboring RCRS or CRS could be preliminarily screened using RSI and RFS score system as well as pepsin assay in the samples of nasal secretion or content of LPR in clinical practice. Furthermore, 24-h pH-Impedance test is strongly recommended in order to confirm the diagnosis of LPR.
Footnotes
Authors’ Contributions
XL S and RX M contributed to the conception and design of the study; ZJ Z, YC L, and YT W performed the experiments, collected and analyzed data; HJ L, JH, QY S, and RX M wrote the manuscript; RX M, NY F, WL W, and XL S revised the manuscript. All authors reviewed and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Ningxia Science Foundation of China (No.2021AAC03513), and Ningxia Medical University Scientific Research Foundation (No.XM2018143).
Ethics Approval
The study protocol was approved by the Ethics Committee of Second Affiliated Hospital of Ningxia Medical University. Informed consent was obtained from all the study subjects before enrollment.
Data Availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.