
Abstract
Significance Statement: Paragangliomas rarely present as a thyroid mass. 1 While fine needle aspiration (FNA) can establish the diagnosis, it can be challenging to distinguish between paragangliomas and medullary thyroid carcinoma due to their neuroendocrine origin. 2 Furthermore, histological distinction between benign and malignant paragangliomas is unclear. 3 Incorporating imaging, histological, and clinical findings is essential to establish the diagnosis.
A 58-year-old woman presented with a six week history of episodic hemoptysis without difficulty breathing. Flexible laryngoscopy demonstrated a subglottic mass which on contrast-enhanced CT neck was an enhancing mass in the anterior tracheal wall inseparable from the right thyroid lobe and isthmus mildly narrowing the trachea (Figure 1). An FNA biopsy was performed the following day with cytology suspicious for medullary thyroid carcinoma. Serum carcinoembryonic antigen (CEA), calcitonin, and ionized calcium levels returned within normal limits. The patient was scheduled for a total thyroidectomy and possible tracheal resection and reconstruction. Axial CT Neck demonstrating an (A) endoluminal mass in the right anterior lateral tracheal wall inseparable from the right thyroid lobe/isthmus, and an (B) enlarged left level 1B lymph node.
Intraoperatively, the thyroid gland was firm but without palpable nodules and adherent to the first, second, and third tracheal rings. The mass was resected en bloc with the thyroid gland, resulting in a 1.8 cm × 1.8 cm tracheal window from the cricoid to the superior aspect of the 3rd tracheal ring (Figure 2). Within the tracheal lumen, the mucosa was resected superior to the window with concern for residual tumor. Subsequent repair of the tracheal defect was performed with a left rotational musculo-periosteal sternocleidomastoid (SCM) flap with the periosteum sutured to the trachea circumferentially.
4
Following the procedure, the patient was stable with no acute or persistent dysphagia, dyspnea, or dysphonia and was discharged home on post-operative day 2. Follow-up PET scan with Cu-64 dotatate showed no evidence of metastatic disease. A tracheal window (1.8 cm x 1.8 cm) from the cricoid cartilage to the superior aspect of the 3rd tracheal ring is shown following resection of the external portion of the mass en bloc with the thyroid gland.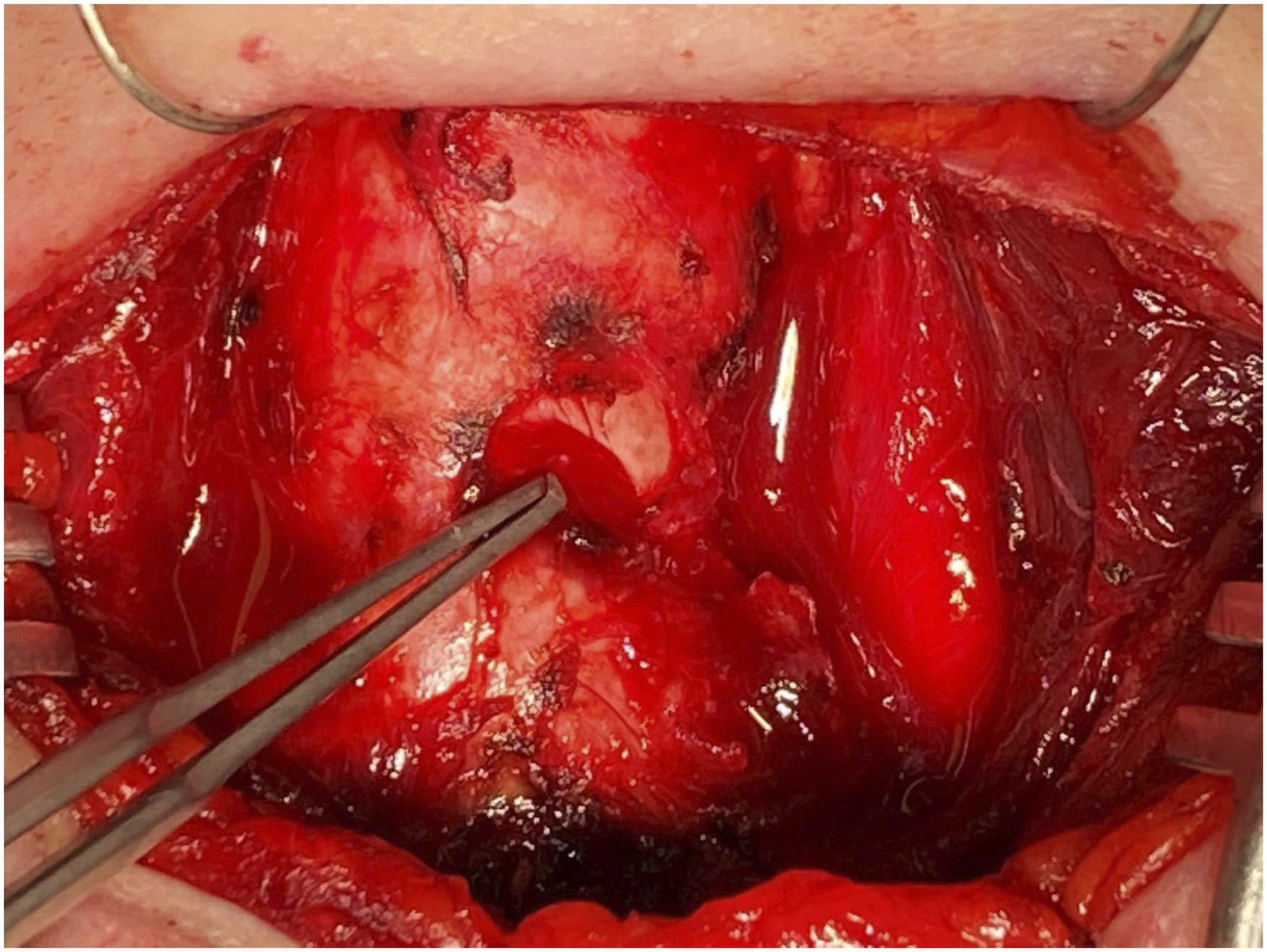
Final pathological specimens demonstrated nests of round to oval neoplastic cells with eosinophilic cytoplasm and inconspicuous nucleoli with minimal mitotic activity (Figure 3A-C). Immunohistochemical (IHC) staining was positive for synaptophysin and chromogranin with S100 staining in the sustentacular cells (Figure 3D-E). Notably, specimens were negative for CKAE1/3, CAM5.2, TTF-1, PAX8, and calcitonin, ruling out medullary carcinoma (Figure F). These findings were consistent with a paraganglioma. (A) The tumor located beneath the tracheal mucosa (hematoxylin-eosin, 100 x). (B) Prominent medium to small sized vessels shown with nested cellular growth pattern (hematoxylin-eosin, 100 x). (C) Tumor cells featuring round to oval nuclei, moderate to abundant eosinophilic cytoplasm, and variably prominent nucleoli (hematoxylin-eosin, 400 x). (D) S100 positivity in the sustentacular tumor cells (200 x), (E) synaptophysin positivity (200 x), and (F) calcitonin negativity (200 x).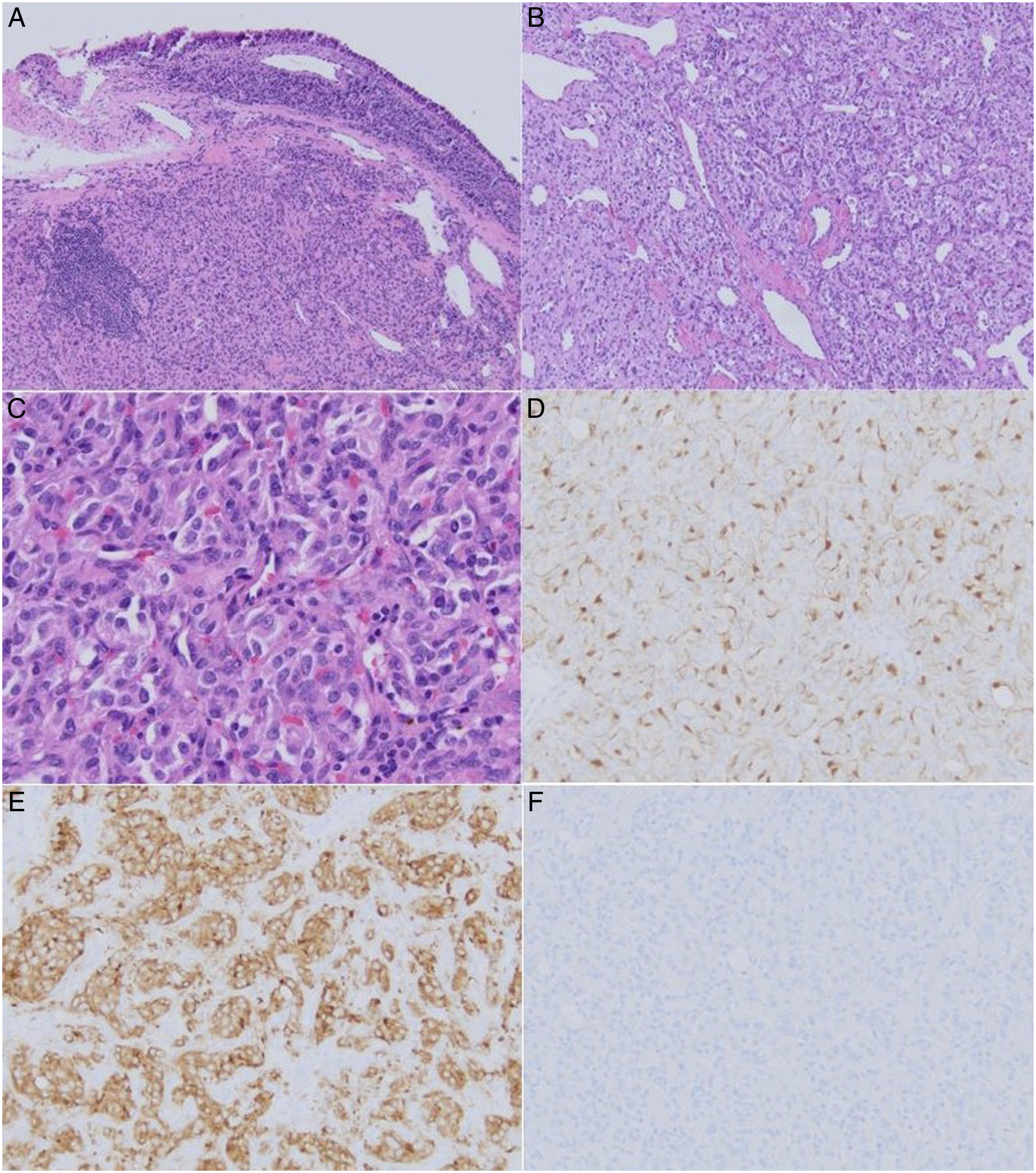
Paragangliomas are typically benign, slow-growing tumors that occur anywhere within the sympathetic and parasympathetic paraganglion system. 5 While 90% are found in the adrenal medulla, 5 3% can be found within the head and neck, and rarely in the trachea.1,6 Of the 16 reported cases of tracheal paraganglioma, 50% presented with hemoptysis, and one was found to have a primary site of origin at the anterior trachea.6,7
The cytological distinction between paragangliomas and medullary thyroid carcinoma can be difficult. 2 Cellular markers paired with specific genetic testing can help; however, this differentiation can be confounded by variants of medullary thyroid carcinoma that express variable markers.2,8,9 Once a diagnosis of a paraganglioma is made, there are no clear histological diagnostic criteria for differentiating between benign and malignant paragangliomas. 3 Instead, malignant paragangliomas are defined by the presence of metastases or spread to tissues where chromaffin tissue is absent. 10 Less than 10% of paragangliomas are malignant, and metastases are typically confined to regional lymph nodes. 10 Malignant paragangliomas carry a relatively poor prognosis with a relative 5-year survival of 59.5%. 10 Benign paragangliomas can be managed with observation alone, however, malignant paragangliomas require surgery with or without adjuvant radiation and/or chemotherapy.10-12
Imaging can be a helpful adjunct in establishing a diagnosis. Medullary thyroid carcinoma has characteristic features on ultrasound including a mass with solid composition, hypoechogenicity, and irregular margins. 13 Additionally, medullary thyroid carcinoma is primarily found in the lateral upper two-thirds of the thyroid lobes, rarely arising as a midline thyroid mass. 14 Characteristic imaging patterns of paragangliomas can be seen with contrast-enhanced CT (avid enhancement, unenhanced density > 10 Hounsfield units) and contrast-enhanced MRI (T2 prolongation and variable contrast enhancement resulting in the “light bulb sign”). 15
This case demonstrates a paraganglioma as a rare cause of hemoptysis, and highlights the need to consider atypical thyroid masses. When FNA and IHC staining findings are inconclusive, tumor location and imaging patterns unique to medullary thyroid carcinoma and paragangliomas can aid in establishing a diagnosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.