
Abstract
Human papillomavirus (HPV)–related multiphenotypic sinonasal carcinoma (HMSC) is a recently described neoplasm entity that presents only in the sinonasal tract. Histologically, it displays features of both a surface-derived carcinoma and a salivary gland carcinoma, and is associated with high-risk HPV, specifically HPV type 33. Whereas majority of the cases display high-grade histologic features, HMSC paradoxically behaves in a relatively indolent fashion. It is important and meaningful to distinguish HMSC from other histopathologic mimickers as the clinical features and management are distinctive. A 64-year-old woman presented having intermittent left-side epistaxis and progressive nasal obstruction. A well-defined, solitary, friable mass with an irregular surface that easily bled upon contact was found in the posterior part of the left nasal cavity. Endoscopic excision of the tumor which was originated from left nasal septum was done and the tumor was confirmed as HMSC. After surgery, definitive radiotherapy was performed in 28 fractions. HMSC is a histopathological type that has been rarely reported so that we report this case with literature review.
Introduction
High risk types of human papillomavirus (HPV) are one of the well-known causative factors in head and neck cancer. 1 HPV-positive squamous cell carcinomas occur predominantly in the oropharynx, accounting for up to 80% of cases. 2 HPV-positive oropharyngeal cancer has steadily increased especially in Western countries. As widely known, HPV-related oropharyngeal carcinomas show better clinical prognosis compared to HPV-negative carcinomas. Furthermore, the stages of oropharyngeal cancer vary according to HPV-positivity. 3,4
Through comprehensive HPV testing of all head and neck cancers, it has suggested that carcinoma related with HPV might be more common. 5 HPV–related multiphenotypic sinonasal carcinoma (HMSC) is a recently described neoplasm that located exclusively within the sinonasal tract. In 2013, Bishop et al first demonstrated sinonasal carcinoma, which is HPV positive and histologically similar to adenoid cystic carcinoma, as a new subset. 6 Bishop et al nominated this type of carcinoma as HMSC. 7 HMSC has only been classified as a preliminary tumor entity by the WHO of Head and Neck Tumor Classification 2017 edition. 8
Human papillomavirus–related multiphenotypic sinonasal carcinoma displays features of both surface-derived carcinoma and salivary gland carcinoma. It shows diverse histologic features including squamous differentiation, sarcomatoid transformation with chondroid and osteoid differentiation, and epithelial-myoepithelial carcinoma-like growth pattern. 9 Furthermore, it is closely associated with high-risk HPV. While HPV type 16 is the most common genotype so far in HPV-positive oropharyngeal carcinoma, HPV type 33 was dominant in most cases of HMSC instead. Bishop et al retrospectively examined 49 cases of HMSC and reported that all cases showed p16 positive and 33 cases were positive for HPV type 33. 7 In addition, types 35 and 56 were also identified. 10
As HMSC is a rare and unique type of tumor, its histopathological type has not yet been widely reported. As HMSC is a recently acknowledged entity, most of the reports have been dealing with its pathological features. 11,12 There are only few clinical reports dealing with clinical aspects of HMSC. Since we recently experienced the HMSC case treated with surgical excision and postoperative radiotherapy, we would like to report the case with literature review focusing on its clinical characteristics.
Case Presentation
A 65-year-old female presented to our clinic with intermittent left-side epistaxis and progressive nasal obstruction. She had no other underlying disease except hypertension. On endoscopic examination, a well-defined, solitary, friable mass was noted on the posterior portion of left nasal cavity. The mass had an irregular surface that easily bled upon contact. (Figure 1) Initial endoscopic findings. (A) A well-defined, solitary, friable mass with an irregular surface that easily bled upon contact was noted on left nasal cavity. (B) A close-up view of the tumor.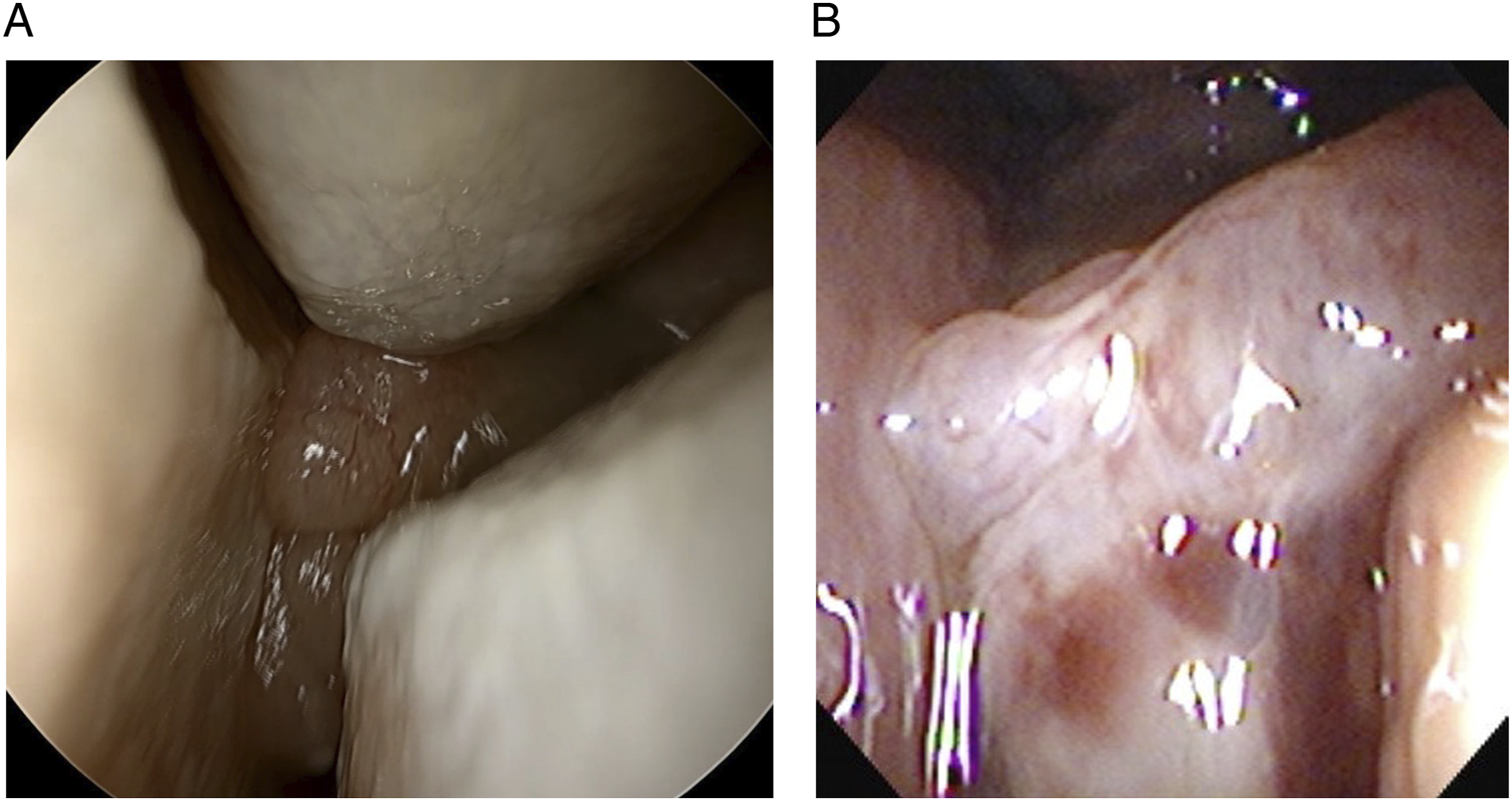
On contrast-enhanced paranasal sinus (PNS) CT, 12.8x12.3mm sized heterogeneously enhancing mass suspected of hemangioma, papilloma or carcinoma was noted at left postero-inferior nasal cavity. (Figure 2) There was no definite invasion of other adjacent structures nor bony destruction. Punch biopsy of the tumor was done immediately at the outpatient clinic. The pathologic result was, “salivary gland type carcinoma, favor solid variant of adenoid cystic carcinoma.” Paranasal sinus CT. 12.8 x 12.3 mm sized heterogeneously enhancing mass was noted at left postero-inferior nasal cavity (an arrow mark).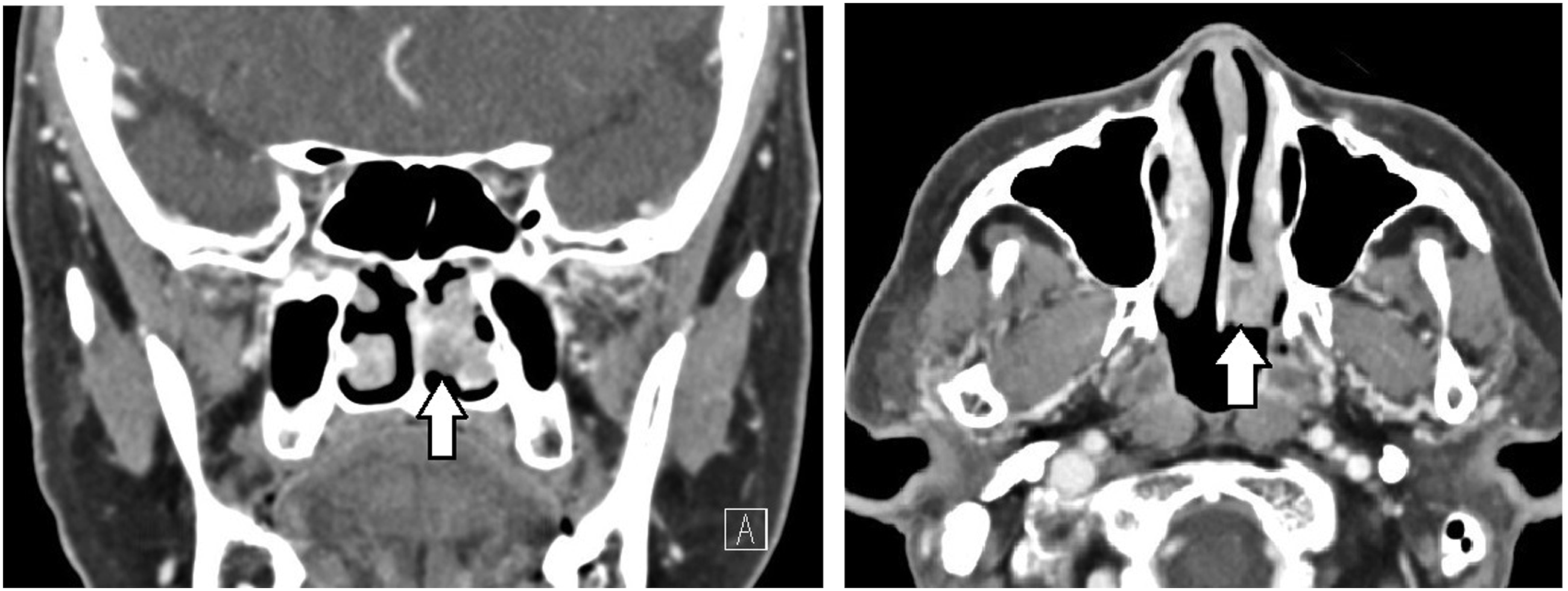
Since there was no evidence of distant metastasis on PET-CT examination, wide excision of nasal cavity tumor was done under sinus endoscopy. First, debulking of the tumor mass was done using forceps and microdebrider. (Figure 3A) The tumor seemed to be originated from the posterior portion of left nasal septum. After debulking surgery, mucosal incision was made at the left septum leaving 1cm safety margin from the tumor origin. (Figure 3B) After careful submucosal dissection, septal mucosa was removed while the remnant tumor was still attached. Perpendicular plate and vomer were also removed so that only opposite side of septal mucosa was remained. There was no gross bony invasion. (Figures 3C and 3D) Intraoperative findings. (A) Debulking surgery. The tumor was originated from left posterior septal mucosa. (B) Incision was done with 1 cm safety margin. (C) Perpendicular plate and vomer was also removed. There was no gross bony invasion. (D) End of surgery. The right side septal mucosa was remained.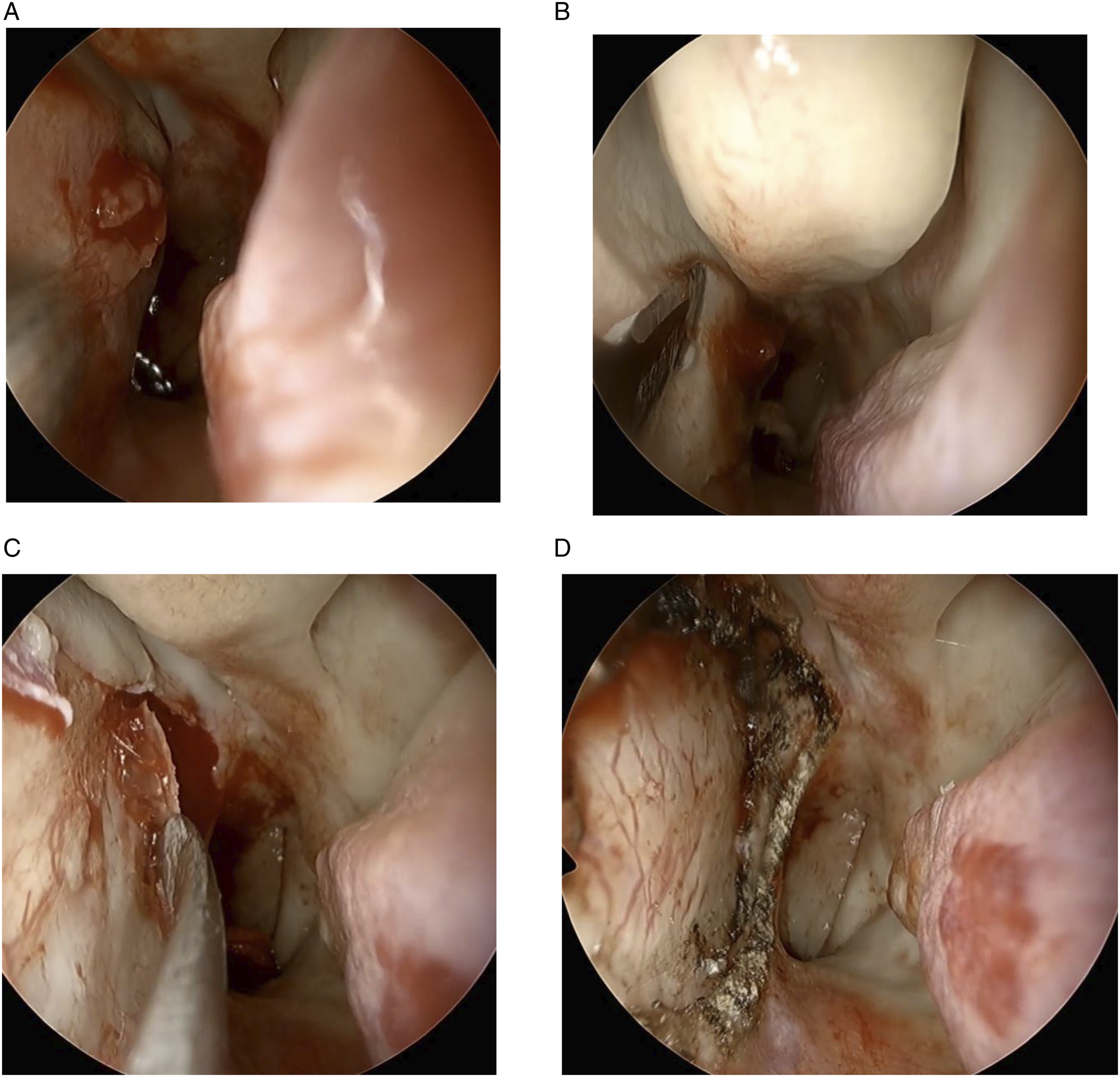
The resected tumor was sent to the pathologic department. The specimen showed biphasic ductal and myoepithelial differentiation on H&E and S100 stain. It also showed positive result on HPV genotyping, especially high-risk type 33. The pathologic result was confirmed as HPV–related multiphenotypic sinonasal carcinoma. (Figure 4) Pathologic result (x100). (A) The tumor shows a proliferation of basaloid cells gathered into the nests on H&E stain. (B) Biphasic ductal and myoepithelial differentiation was evident on S100 stain. (C) Diffuse and strong nuclear and cytoplasmic staining was shown on p16. (D) Positive for the cytokeratin cocktail AE1/AE3. (E) Positive for squamous marker stain with p63.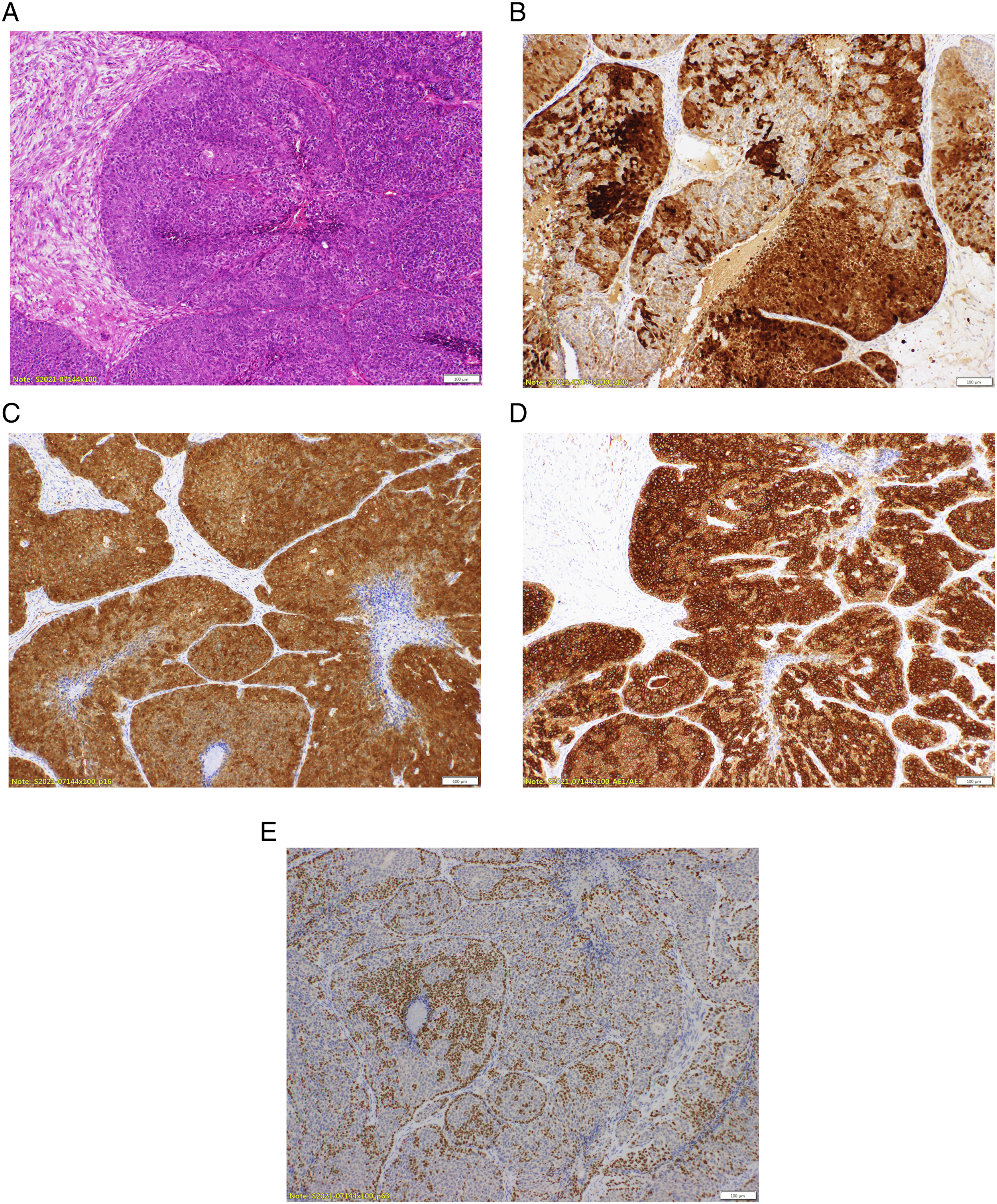
After the operation, the patient underwent definitive radiotherapy; a total of 6300cGy to nasal cavity and 5040cGy to paranasal sinus in 28 fractions. The patient terminated the treatment without significant side effects on surgery and radiation therapy. Since then, the disease has been well controlled without recurrence on both endoscopic exam and PNS CT for 12 months. (Figure 5) The patient did not feel any discomfort on the nasal cavity at all. Post-treatment findings (POD 12 months). There was no crust on nasal mucosa after radiotherapy, and no evidence of recurrence on the endoscopic finding.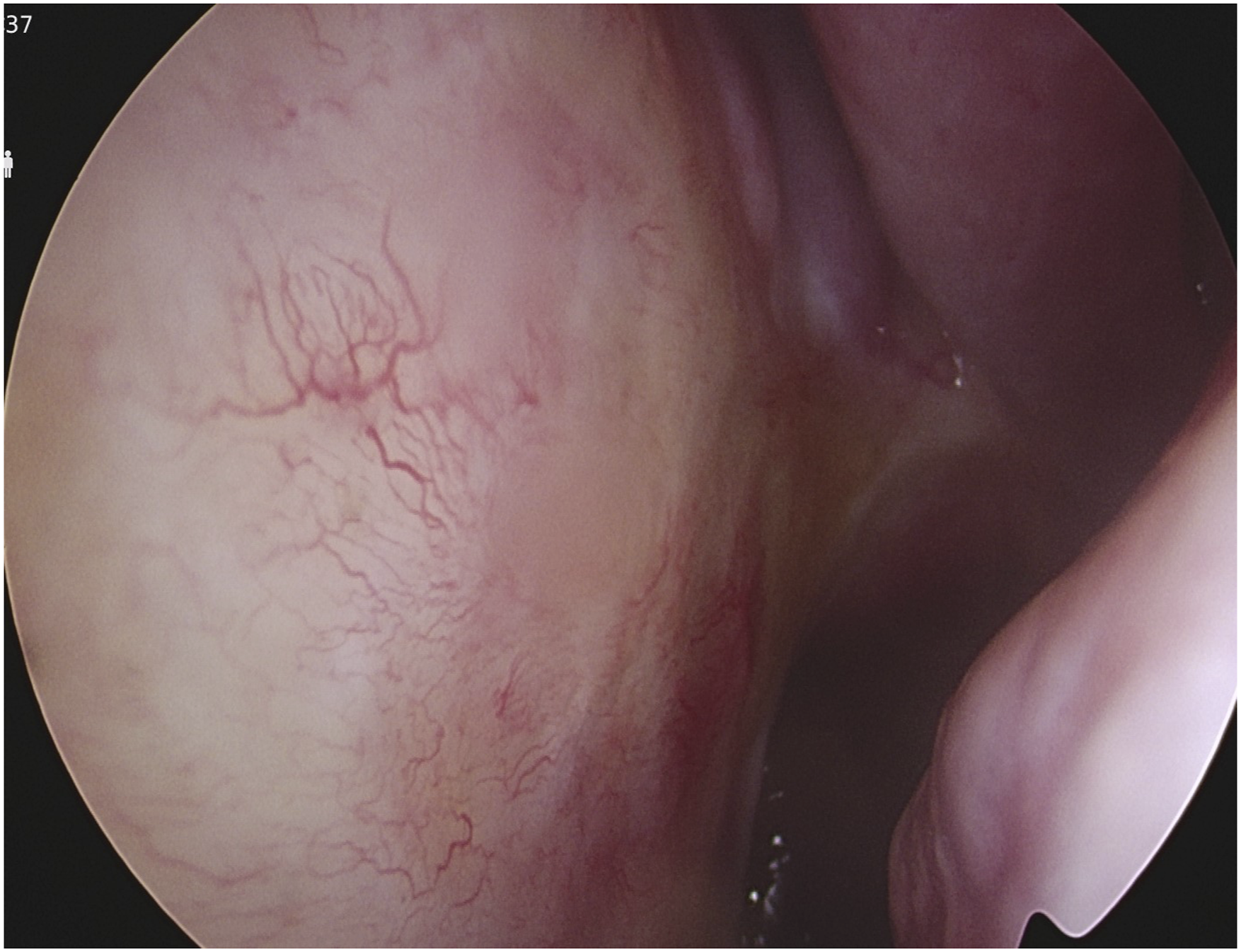
Discussion
Human papillomavirus–related multiphenotypic sinonasal carcinoma is a unique and rare type of malignant neoplasm found in sinonasal tract. Histologically, HMSC displays various features, which is similar to adenoid cystic carcinoma, squamous cell carcinoma, and carcinoma with basaloid appearance. 11,12 HMSC might easily be confused by careless pathologist with these histopathologic mimickers, because it is comprised of a puzzling mixture of cellular elements, as can be inferred from its name “multiphenotypic.” As a definite distinguishing point from these tumors, HMSCs have a strong association with high-risk HPV, specifically HPV type 33.
In the oropharynx, HPV–related squamous cell carcinoma has realized as a distinct type with its own individual demographic, histopathologic, and clinical characteristics. 13 However, it is not clear yet whether HPV-positivity also affects the clinical profiles significantly in sinonasal carcinomas. As HMSC is a recently acknowledged entity, there are only few reports of clinical cases including its behavior, prognosis, and optimal treatment. Nevertheless, most reports revealed that HMSC rarely renders into aggressive behavior. Although majority of the HMSC cases display high-grade histologic features, HMSC paradoxically behaves in a relatively indolent fashion clinically. HMSC is usually limited to the nasal cavity and adjacent paranasal sinuses, and lymph nodes metastasis or distant metastasis were unusual. 14,15 There was one disease-related death reported until now. 16 Bishop JA reported that the hazard rate among the patients of HPV-negative group was 72% higher than HPV-positive group (hazard ratio = 1/72 with 95% CI [0.78, 3.82]). In addition, 5-year survival rate of HPV-positive sinonasal squamous carcinoma was 69.7% (95% CI [27.6%, 86.5%]), whereas HPV-negative group was 50.6% (95% CI [22.5%, 79.5%]). 17
Human papillomavirus–related multiphenotypic sinonasal carcinoma is known to show a relatively good prognosis than other histologically high-grade sinonasal carcinomas, but there is no established standard treatment method and consequent prognosis yet. Complete surgical excision is the main treatment up to date, and postoperative radiotherapy or chemotherapy could be an optional treatment choice. In the report of Bishop JA et al, which did treatment and follow-up in 42 HMSC patients, surgical resection was performed for most of them, and radiation therapy was added in some cases. Sixteen of HMSCs (38%) showed local recurrence and late recurrence was not noted. 17 There was one reported case that showed a local recurrence 31 years after the surgical resection of the primary tumor. 18 In our case, wide excision of the primary tumor under endoscopy and postoperative radiotherapy was performed. These treatment processes were not too much of a burden to the patient and the tumor was well controlled. The distant metastasis and local recurrence was not noted until 12 months later so far.
It is important and meaningful to distinguish HMSC from other histopathologic mimickers as the clinical features and management are significantly different. Accurate diagnosis and pooling of HMSC cases would aid collecting information on clinical features which is essential to clarify this unfamiliar tumor.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.