
Abstract
Metastases to the vocal cord from a distant organ are extremely rare. This case showed metastatic adenocarcinoma on the vocal cord of lung origin in a 75-year-old nonsmoking female with a history of lung adenocarcinoma surgery 2 years earlier. The vocal cord mass was surgically removed, and the biopsy confirmed metastatic adenocarcinoma of lung origin with thyroid transcription factor (TTF)-1 positivity. A further evaluation found recurrence in the lung. The patient received gefitinib. Here, we report an extremely rare case of metastatic adenocarcinoma on the vocal cord from the lung which is the first report to our knowledge.
Introduction
Lung cancer accounts for almost 25% of all cancer deaths. 1 Recent statistics showed that the leading cause of death in men over 40 and women over 60 years was lung cancer. 1 Lung cancer can metastasize to multiple organs such as the lungs, brain, bones, adrenal glands, and lymph nodes.2,3 In contrast, among all laryngeal tumors, only 0.09–0.40% are metastatic laryngeal tumors. 4 Most previous studies were case reports documenting metastatic laryngeal tumors originating from skin melanoma, kidney, breast, lung, prostate, and colon cancer due to its rarity.5-11 Within the larynx, metastatic lesions are located in the supraglottis and subglottis, both known for well-developed lymphatic and blood circulations.5,10,12 Herein, we present a case of metastatic adenocarcinoma from the lung to the vocal cord, which is part of the glottis.
Case Report
A 75-year-old woman was referred to the otorhinolaryngology department with a month-long history of hoarseness. She was a non-smoker and had a history of hypertension and video-associated thoracic surgery (VATS) lobectomy with lymphadenectomy for an adenocarcinoma in the right lower lobe (RLL) at another hospital 2 years earlier. Follow-up chest contrast-enhanced computed tomography (CECT) 6 months postoperatively showed no evidence of recurrence. Flexible laryngoscopy revealed a reddish papillary mass occupying two-thirds of the right vocal cord from the posterior part (Figure 1). Otherwise, the general physical examination was unremarkable. Flexible laryngoscope finding reveals a reddish papillary mass occupying two third of the right vocal cord from posterior part close to vocal process.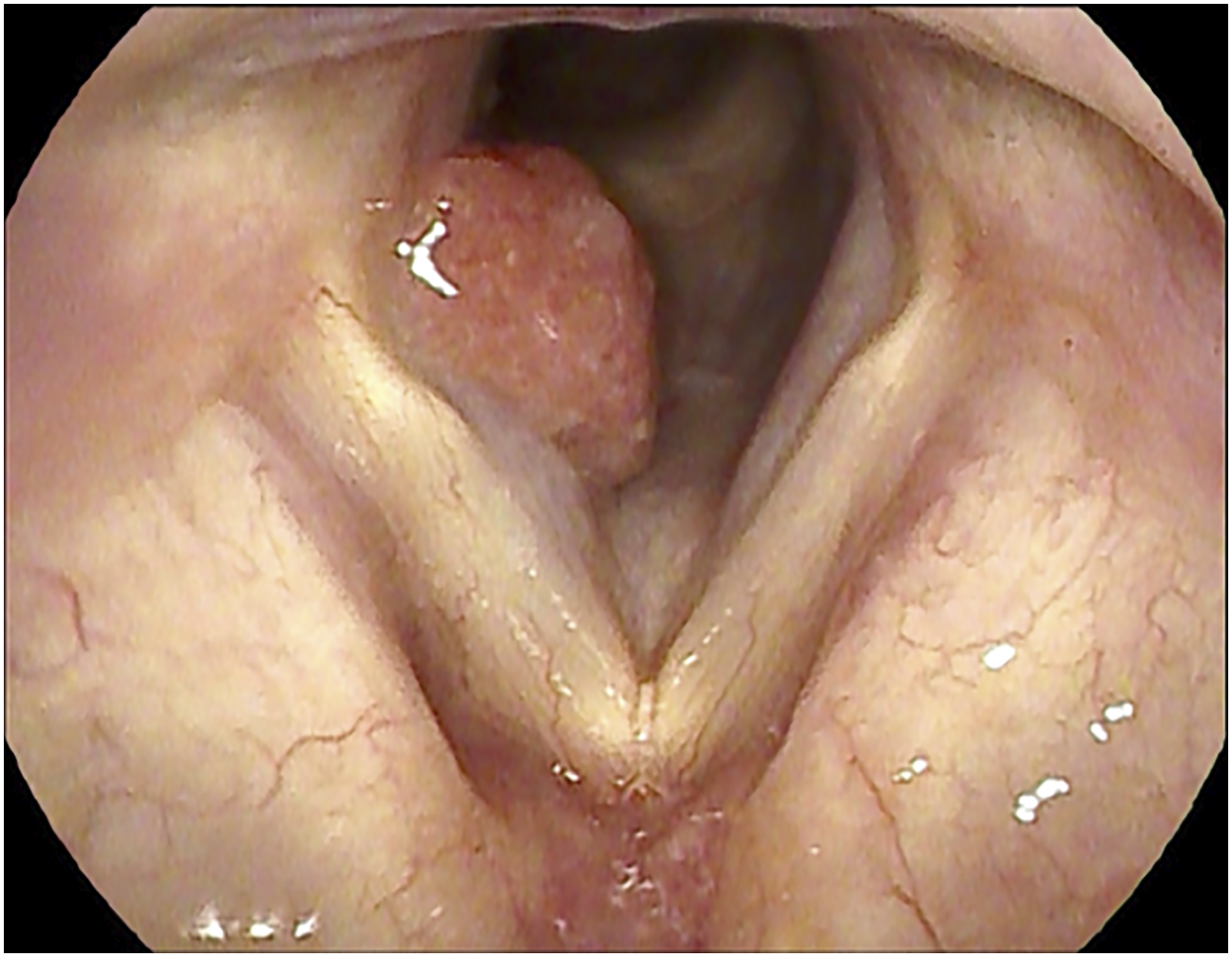
The vocal cord mass was removed under laryngeal microsurgery using a CO2 laser while pulling the mass with a suction tube. The mass was soft and confined to the mucosa of the vocal cord above the vocal process of the arytenoid cartilage. Pathological evaluation revealed a tumor with papillary architecture and moderate nuclear atypia (Figure 2A). Immunohistochemical analysis was positive for thyroid transcription factor-1 (TTF1) but negative for PAX8, suggesting metastatic pulmonary adenocarcinoma. Postoperative flexible laryngoscopy showed no sign of a remnant mass. Features of tumor cells (A) The tumor cells of vocal cord showed predominantly of papillary structures with fibrovascular cores. (Hematoxylin and eosin, x100) (B) The pulmonary tumor tissue was composed of branching papillae and showed the same histologic features as the vocal cord. (Hematoxylin and eosin, x100).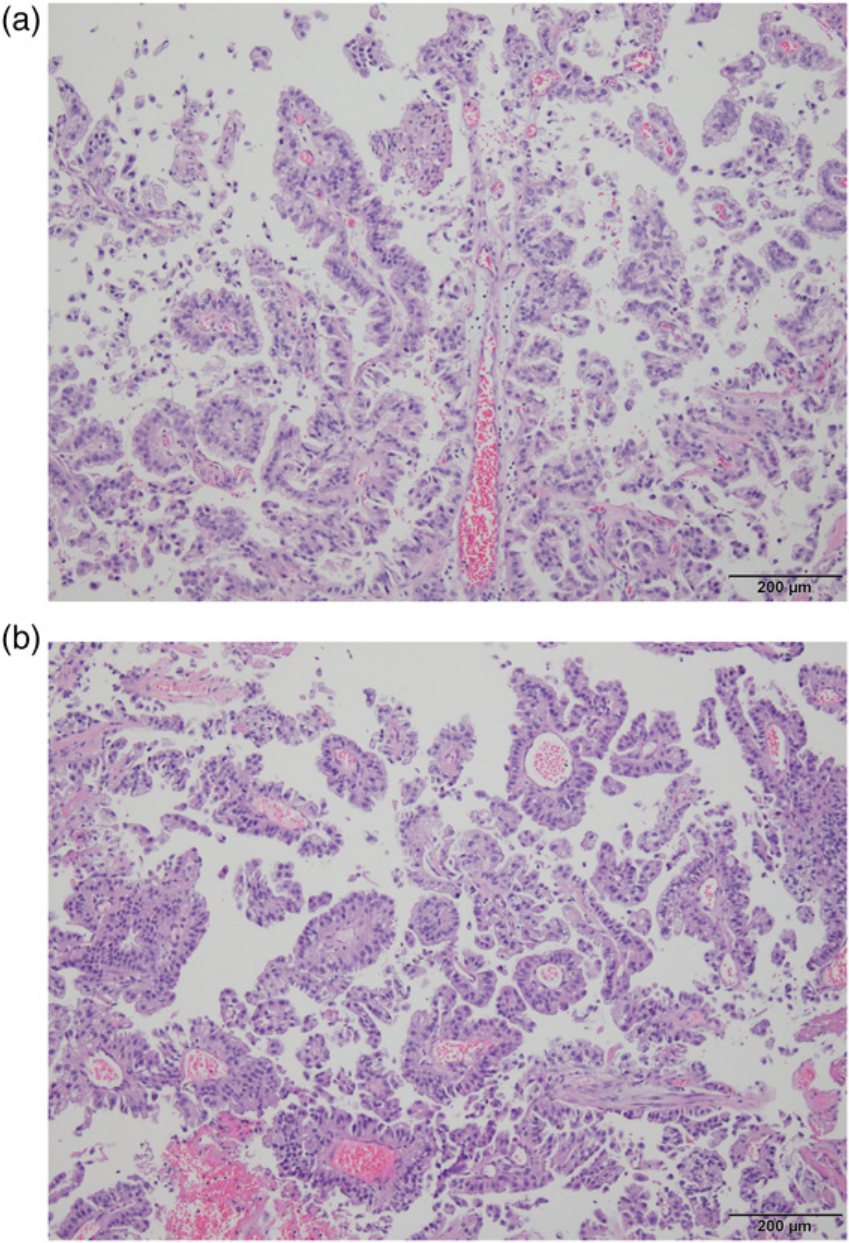
Positron emission tomography (PET) and chest high-resolution computed tomography (HRCT) revealed a high probability of a recurrent tumor in the stump site of the right lower lobe lobectomy. Brain magnetic resonance imaging (MRI) showed no significant metastatic lesion, while a 4.4 × 4.1 × 3 cm extra-axial enhancing mass with calcification in the left anterior falx cerebri considered to be meningioma was persistently present, similar to the brain CT 3 years earlier. Bronchoscopy showed a protruding mass with luminal obstruction at the orifice of the right middle lobe (RML)/RLL stump. Histologically, the pulmonary tumor showed papillary adenocarcinoma (Figure 2B). At the time of writing, the patient was referred to the pulmonary department for targeted therapy with gefitinib.
Discussion
Hoarseness is known as the first symptom of glottic cancer, but when the mass is located at the posterior third of the vocal folds, vocal process granuloma is usually suspected.13-16 However, the flexible laryngoscopy finding of a reddish papillary mass on the posterior part of the vocal cord did not match the typical findings of either disease, which led to prompt surgery for biopsy and removal.
Bones, lungs, brain, adrenals, and the liver are the frequent metastatic sites of lung carcinomas.2,3 Metastases on the larynx from other primary tumors are rare. 4 Some cases of malignant melanoma, renal carcinoma, and even from lung cancer have been reported.5-11,17 Nevertheless, these cases occurred in the supraglottis and subglottis, which have a rich lymphatic and vascular supplies.5,10,12,17 The vocal cord mass in this patient was confined to the vocal cord mucosa, which is the glottis. A CO2 laser was used between the normal mucosa and the mass. The CO2 laser ablation could have vaporized the normal adjacent mucosa, resulting in no pathological evidence of adjacent mucosa and only adenocarcinoma. The preoperative chest X-ray showed no significant lesion. However, after the vocal cord biopsy revealed metastatic pulmonary adenocarcinoma, PET and HRCT were performed, indicating the high probability of recurrence in the lung. The bronchoscopy biopsy confirmed recurrence of the lung cancer. Since recurrence occurred not only in the lung but also at the vocal cord, systemic therapy such as chemotherapy was considered for treatment. Although the vocal cord showed no remnant lesion, patients with metastatic involvement of the larynx seems to have a poor prognosis since the disease is already in an advanced stage.
In non-small cell lung cancer (NSCLC), which includes squamous cell carcinoma, adenocarcinoma, and large cell carcinoma, surgical treatment is the treatment of choice in the early stages. Unfortunately, the long-term survival is below 50% even after surgery.18,19 According to a previous study, 80% of the local and locoregional recurrences occur in the first 2 years. 18 The patient had a postoperative CT performed after 6 months after lobectomy with no signs of recurrence. To detect postoperative recurrence, CT appears to be better than PET in terms of specificity, although the positive predictive value was only 53%.19,20 The clinicopathological characteristics of the patient, which were female, nonsmoking, and adenocarcinoma, have been documented as predictive factors for gefitinib response, a tyrosine kinase inhibitor of the epidermal growth factor receptor (EGFR). 21 Gefitinib was administered to the patient. In addition to improvements in symptoms and radiographical regression of the tumor, gefitinib showed less adverse effects and cytotoxicity than conventional chemotherapy. 22
The vocal cord can be a target for distant metastases from other primary tumors. In particular, when the patient undergoes lobectomy due to lung cancer, radiologic evaluation including chest CT should be considered for a vocal cord mass along with laryngeal microsurgery for biopsy and removal.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Institutional Review Board of Chonnam National University Hwasun Hospital (IRB CNUHH-2022-061).
Statement of Informed Consent
Written informed consent was obtained from the patient(s) for the publication of their anonymized information to be published in this article.