
Abstract
Objective
To describe and analyze the demographics and academic backgrounds of United States otolaryngology program directors (PD) and assess gender disparity in the field.
Methods
This was a cross-sectional study in which an online search using publicly available sources was performed to gather information on PDs for 125 United States otolaryngology programs from May 14, 2021, to May 30, 2021. Data collected included PD appointment year, age, gender, resident gender breakdown, degree, as well as training location and graduation year.
Results
There were 69.6% programs with a male PD and 30.4% with a female PD. Ninety percent of PDs have an MD degree and 9.6% have a DO degree. The current average age of PDs was 49.9 years old (range 35–79). Males were older than females PD (51.0 vs 47.1 years, P = 0.045) and have served a longer time as PD (7.1 vs 4.8 years, P = 0.019). There was no significant difference in other variables collected. There were 27.3% of program directors that held the position of professor, 44.5% associate professor, and 28.2% assistant professor. The most common subspecialty practiced by otolaryngology PDs was head and neck oncology.
Conclusion
Disparity in women’s representation in otolaryngology still exists, but the program director leadership position demonstrates better parity. There is an equal percent representation when examining female PDs and female otolaryngologists in academic medicine. Continued efforts to encourage women to enter and become leaders in otolaryngology are necessary moving forward.
Introduction
Program directors (PD) hold a unique role in serving as residents’ advocates and mentors, as well as supervisors and employers. According to the Accreditation Council for Graduate Medical Education (ACGME), the PD role includes the responsibility and authority of administration and operations, teaching, scholarly activity, resident recruitment and selection, evaluation, promotion of residents, disciplinary action, and resident education in the context of patient care. 1 PDs may therefore influence the “fit,” program culture, and environment that future residents are often assessing when choosing a program. They serve as leaders and “faces” of the residency program and remain one of the most consistent mentors of residents throughout their residency.
Mentorship plays a vital role in career choice, research productivity, and personal and professional development. Women perceive a more difficult time finding a mentor than their male counterparts. 2 While it has been shown that mentorship increases the likelihood of considering a surgical career, there is a relative lack of female mentors due to the lower representation in surgical specialties and leadership positions.3,4 Therefore, this lack of mentorship may impede or affect career development and the opportunity for advancement in leadership for other female physicians.
AAMC statistics for 2020 report that women in otolaryngology comprise 16.4% (89/542) professors, 29.0% (161/556) associate professors, and 39.5% (369/933) assistant professors. 5 While women may be underrepresented in the field, and this shows a slight shift towards women in higher academic positions compared to 2015, which demonstrated 13.0% (66/497) professors, 27.0% (115/431) associate professors, and 34.0% (272/804) assistant professors.6,7 There was limited data regarding the representation of women in otolaryngology before 2015. These observed trends highlight the importance of assessing and reporting women's representation in otolaryngology leadership.
Previous studies in other fields, including surgical subspecialties, have reported descriptive statistics of PDs 8 ; however, there is a paucity of evidence examining otolaryngology residency PDs specifically. As such, we aim to describe and analyze the demographics, training, and academic backgrounds of United States otolaryngology PDs, with a focus on gender equity and gender representation within the field.
Patients and methods
This cross-sectional study utilized publicly available resources polled between May 14, 2021, and May 30, 2021. A list of current otolaryngology programs was determined from Doximity.com and verified with FRIEDA Online (https://freida.ama-assn.org/) to make sure all programs were captured in the analysis. Data were gathered for 125 PDs. Since this data is freely and publicly available, this study was deemed exempt from the Penn State Institutional Review Board (STUDY00017911).
The methods for this study were modeled after a previously published study on a descriptive analysis of ophthalmology PDs. 8 Data gathered included PD appointment year, gender, program resident gender breakdown, type of degree (MD or DO), medical school, residency and fellowship location, graduation year, and fellowship subspecialty. The time to appointment was determined by the number of years from graduating residency to becoming a PD. The duration of appointment was calculated by subtracting the year appointed from the current year. If educational information was not found on Doximity (doximity.com), residency program websites were used for further inquiry. Doximity’s top 50 rankings (2020–2021) (doximity.com) based on residency program reputation were used to rank programs.
PDs’ age and gender were determined by using Healthgrades (https://www.healthgrades.com/). The percentage of female faculty at different institutions was determined from program websites’ faculty pages. Lastly, FREIDA Online (https://freida.ama-assn.org/) was used to assess program type (university-based, community-based, university-affiliated, community-based, or military). PDs with partial information available were still included in the study. Statistical analyses with Kruskal–Wallis Test and Chi square analysis were calculated in IBM SPSS (Armonk, NY, USA) version 27.
Results
Demographic Characteristics and Training of U.S. Otolaryngology Residency Program Directors.
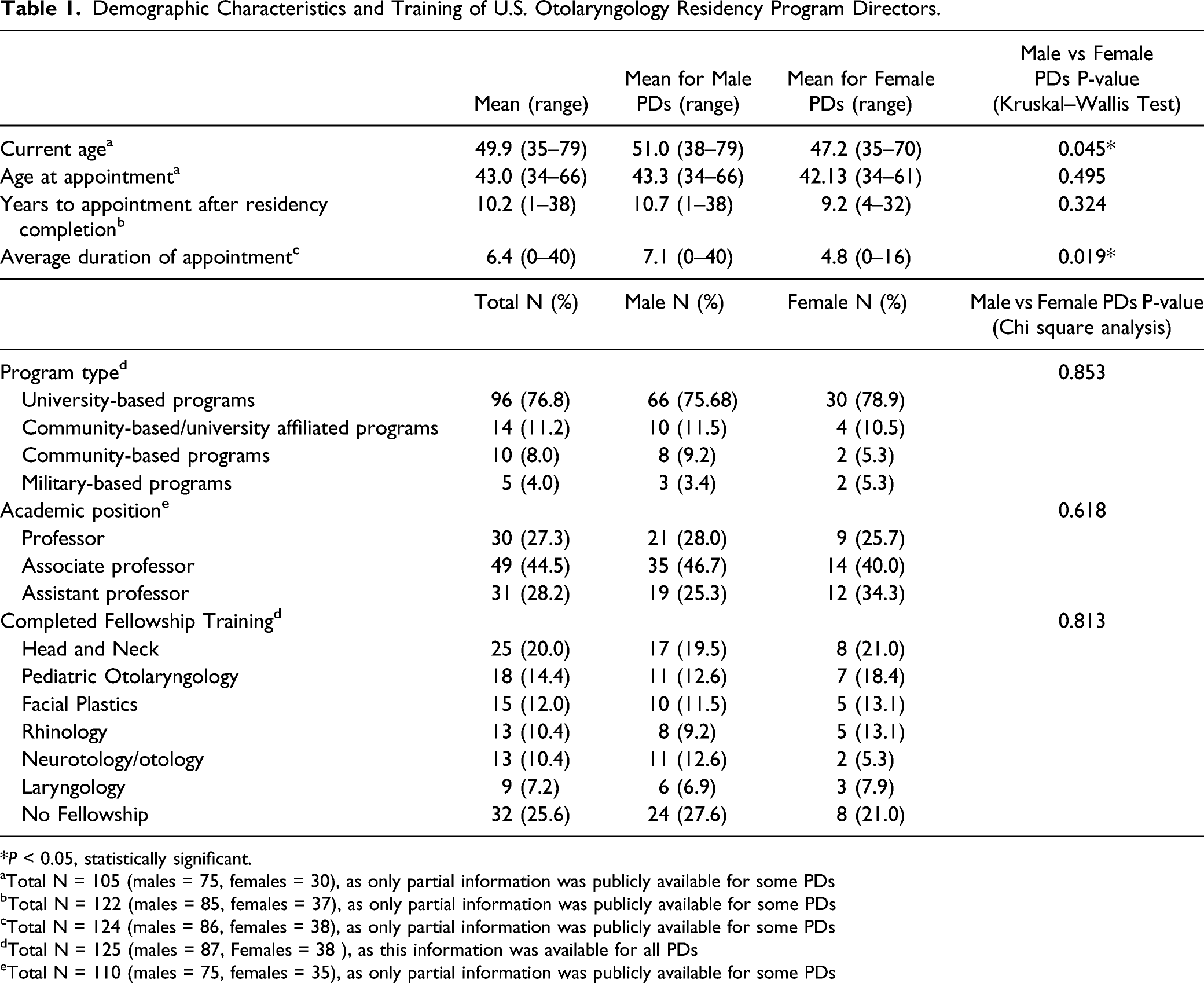
*P < 0.05, statistically significant.
aTotal N = 105 (males = 75, females = 30), as only partial information was publicly available for some PDs
bTotal N = 122 (males = 85, females = 37), as only partial information was publicly available for some PDs
cTotal N = 124 (males = 86, females = 38), as only partial information was publicly available for some PDs
dTotal N = 125 (males = 87, Females = 38 ), as this information was available for all PDs
eTotal N = 110 (males = 75, females = 35), as only partial information was publicly available for some PDs
When assessing program type (community-based, academic, military, etc.), where they serve, and current academic position, there were no differences between male and female PDs (Table 1). Amongst PDs with academic position information publicly available, 27.3% (30/110) currently hold the position of professor, 44.5% (49/110) associate professor, and 28.2% (31/110) assistant professor (Table 1). This data reports the PD’s current academic rank, but data on rank at the time of PD appointment was not available.
U.S. Otolaryngology Residency Program Directors and Residents and Faculty Gender Breakdown.
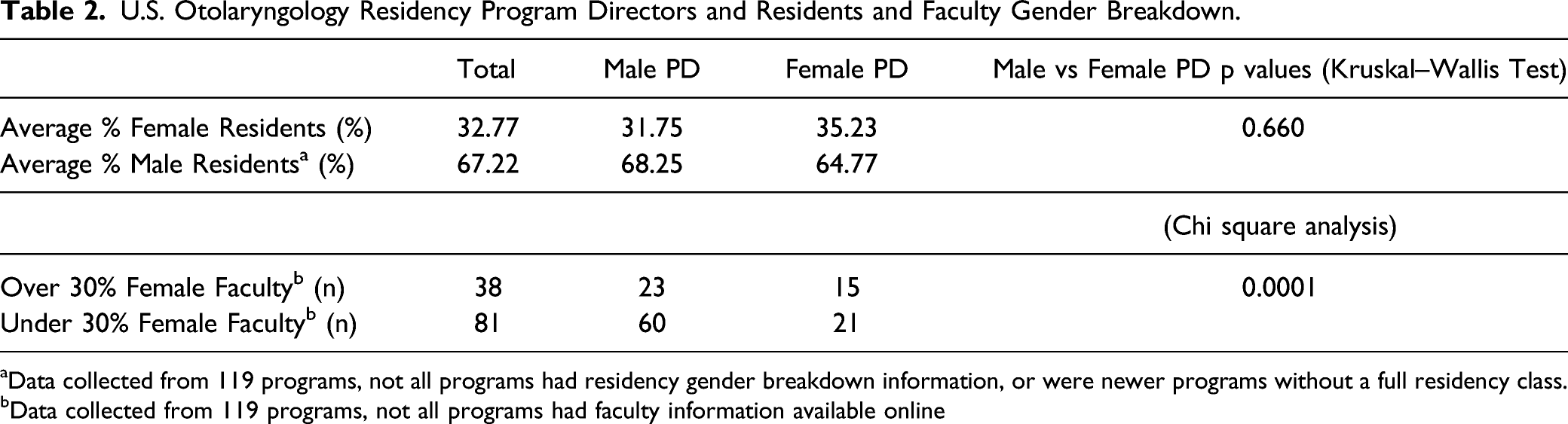
aData collected from 119 programs, not all programs had residency gender breakdown information, or were newer programs without a full residency class.
bData collected from 119 programs, not all programs had faculty information available online
U.S. Otolaryngology Residency Program Directors Similarities in Training and Final PD Location.

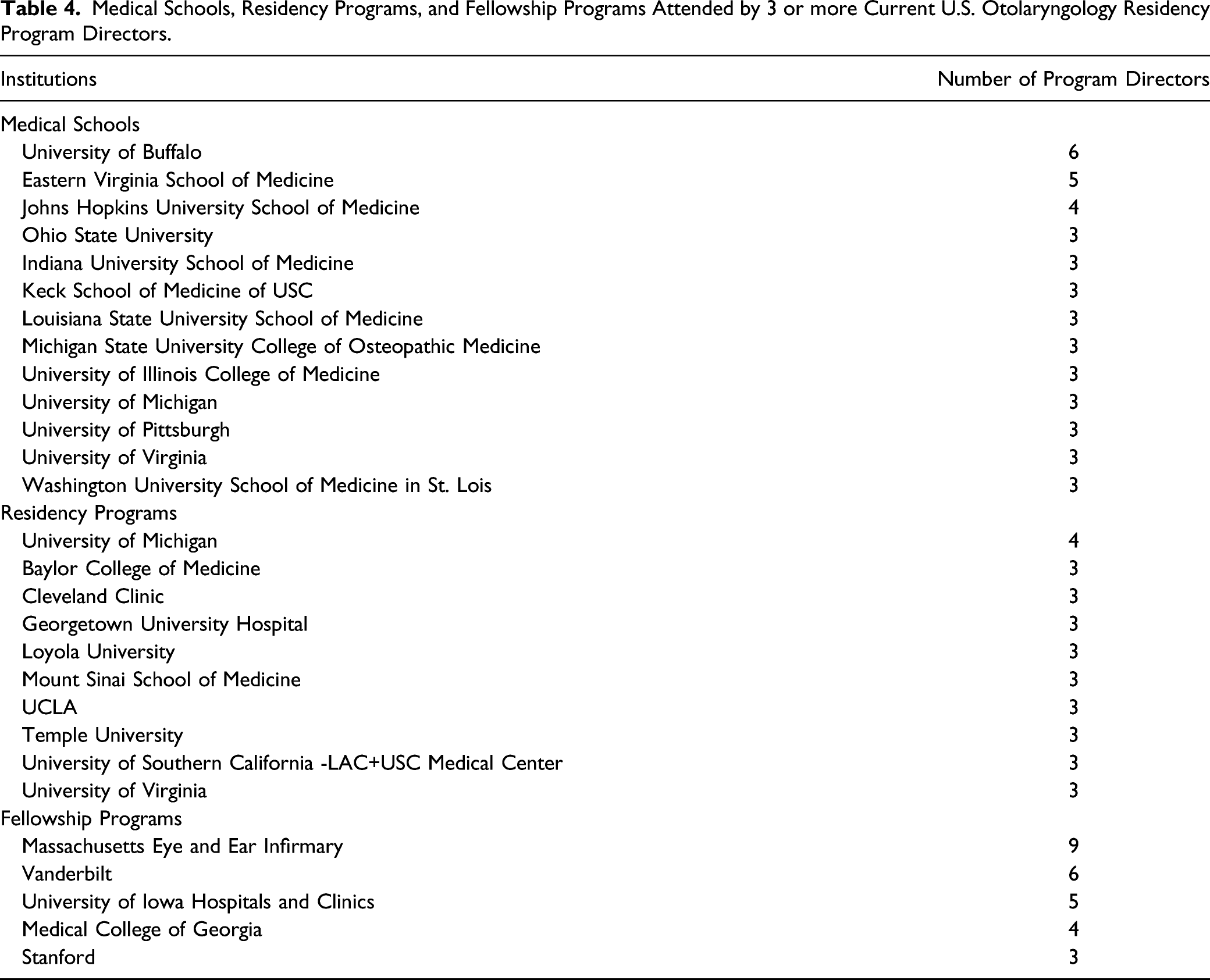
Medical Schools, Residency Programs, and Fellowship Programs Attended by 3 or more Current U.S. Otolaryngology Residency Program Directors.
Educational and Training Backgrounds of U.S. Otolaryngology Residency Program Directors.
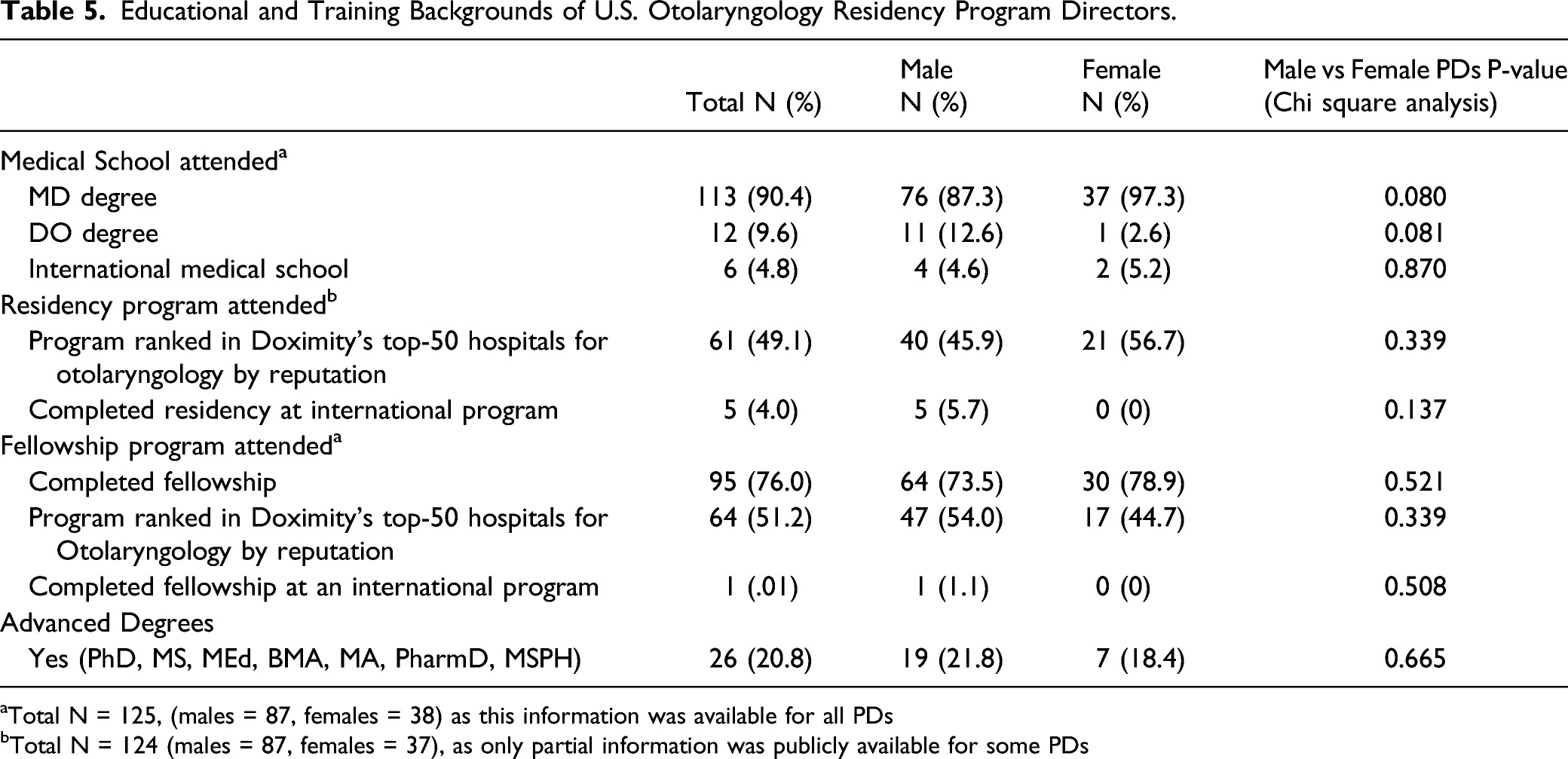
aTotal N = 125, (males = 87, females = 38) as this information was available for all PDs
bTotal N = 124 (males = 87, females = 37), as only partial information was publicly available for some PDs
Discussion
Program directors serve several different roles and are an integral part of shaping resident education and program culture. Therefore, it is essential to analyze PD characteristics to understand the current national standing of leadership within otolaryngology. Discrepancies in representation between men and women in medicine have shown improving trends in recent years. In fact, there are more female than male medical students matriculating. 9 It is important to determine whether these changes translate later to the traditionally male-dominated surgical subspecialties and gender equity and representation in otolaryngology specifically.
The average age of current PDs was 49.9 years old, with female PDs being significantly younger than male PDs. Female PDs have also served a shorter amount of time than male PDs. These findings could reflect the more recent trend of increasing the representation of women in medical leadership. According to the American Medical Association, in 2019, 18.3% of currently practicing otolaryngologists were women. 10 This is much lower than the percentage of female PDs found in this study (30.4%). However, when specifically looking at academic medicine, women similarly represent 30.4% (619/2031) of academic otolaryngologists. 5 This shows that the representation of women in PD leadership reflects the representation of women in academic practice, which both outpace the percentage of women in the specialty overall. The 2020 AAMC report on residents highlights that 38% of current otolaryngology residents are women. 11 The present study found that 32.8% of residents are women. This difference is likely due to incomplete data on publicly available resources. However, females make up 50.5% of current medical school graduates, far exceeding the number entering the specialty. 12 Nonetheless, with increasing numbers of female residents and more women entering medical school, we will hopefully begin to see an increase in women in our specialty and key leadership and mentorship roles throughout the field.
The similar rates of female PDs and women in academic medicine noted in the present study may reflect recent efforts in otolaryngology to encourage women in leadership, such as the AAO-HNS initiating the Women in Otolaryngology (WIO) program.6,7,9 The WIO Section now contains over 2,000 members and aims to assist the career development of female otolaryngologists through networking and mentoring. While this data is promising, women are still underrepresented in the field. Continued efforts and further diligence in fostering and maintaining gender diversity are needed.
A previous survey study completed a 17-year longitudinal follow-up of faculty at medical schools in the United States to identify predictors of female faculty advancement and found that women in academic medicine were less likely to achieve a senior position even after adjusting for publication-related productivity and less likely to achieve the rank of professor compared to men. 13 Research productivity can be used to attain grants, promotions, and leadership positions. Previous evidence shows that female otolaryngologists maintain research productivity throughout their careers and keep pace with their male counterparts. 14 This is in contrast to another study demonstrating that even though women have similar research output compared to men later in their careers, they tended to lag behind at the beginning of their careers. 15 While the reasons for this trend remain unclear, and future studies could seek to address this disparity further.
A recent article by Dr. Abaza discusses the underrepresentation of women in leadership in otolaryngology and addresses the various barriers faced by women. 16 Women in medicine often have a disproportionate share of domestic duties compared to men, which may, in turn, impact advancement.17,18 Additionally, specific characteristics of a leader may be viewed as positive assets in men but not necessarily in women. Throughout this paper, she offers several solutions to this dilemma, such as blinding resumes and letters of recommendation, and uniform implicit bias training. 16 Traditional academic promotion is based on clinical, research, and academic achievements; however, this may not be the most representative assessment of the ideal skill set needed among leaders in academic medicine.
Furthermore, a recent study was published by Tulunay-Ugur et al. investigating gender differences in perceptions of work–life integration among head and neck surgeons. 19 They demonstrated that women were less likely to hold a seniority position in the academic setting, have fewer children per family, more likely to be divorced, and more likely to report mental health issues than their male counterparts. 19 These findings demonstrate that there is still much work to achieve gender equality in the field.
The current study reports that out of all female PDs, 25.7% were professors, 40.0% were associate professors, and 34.3% were assistant professors. A previous study published in 2019 found that out of all female otolaryngologists, 16.0% were professors, 25.0% were associate professors, and 59.0% were assistant professors. These numbers demonstrate that female otolaryngologists who are PDs tend to have a higher current ranking compared to overall academic female otolaryngologists. It is important to note that the present study gathered data on the current rank of PDs. Thus, we cannot be certain that they had these titles at the time of appointment and cannot comment on whether the PD role contributed to promotions or if having a higher rank helped them achieve the PD position.
Some studies have assessed trends in gender, racial, and ethnic minority groups in otolaryngology and determined factors associated with the United States distribution of female residents.20,21 The presence of underrepresented groups in medicine (UiM) among current residents in otolaryngology is increasing. Significant factors associated with greater representation of women include higher-than-average female faculty representation, larger residency programs, and urban programs. Because of this, it was hypothesized that having a female PD may increase the female resident representation. 21 However, in agreement with a previous study, we found no association between female PDs and the percentage of female residents training in a particular program. 21
In 2020, the AAMC reported that 30.4% of academic faculty in otolaryngology were women. 5 At the program level, we found that programs with a female PD tended to have a greater percentage of female faculty than this reported statistic. Some programs may be better at prioritizing diverse representation across all positions within a department, including PD. It is essential to understand these strategies and learn from these programs.
There was no difference between male and female PDs in whether they trained at a top-50 program based on Doximity reputation rankings. When medical students create a residency rank list, program prestige may be an important consideration. A 2018 survey response study among applicants found that 78.0% of respondents found the Doximity rankings “valuable” or “very valuable.” 22 Doximity combines subjective and objective reviews in their ranking system. As a result, the reputation ranking system tends to favor larger programs. 23 There was also no difference between male and female PDs when looking at the type of degree (MD or DO) and whether they obtained an additional advanced degree.
A previous survey study published in 1999 found that 71.0% of academic otolaryngologists completed a clinical fellowship 24 ; however, this number may have increased in recent years since there has been a shift toward more otolaryngologists completing fellowships. 25 The current study found that 76.4% of PDs completed a fellowship, which closely resembles the percentage of fellowship-trained otolaryngologists practicing in an academic setting. There was no difference between the percentage of male and female fellowship-trained PDs.
Our data demonstrated that more than half of the PDs previously performed some training at the institution at which they hold the PD position, which is likely related to personal connections to the program, residents, and training. For example, 25.6% of PD completed medical school at the same institution, 34.4% completed a residency at the exact location, and 11.2% completed a fellowship at the exact location where they are now PD. A previous study determined that 40% of residency applicants stay in the same geographical region as their medical school for otolaryngology residency, with 28.0% staying in the same state. 26
While this study gives insight into some program directors’ descriptive characteristics and training, there were several limitations. First, some of the publicly available websites may not have the most recent data. However, the data was consistent when checking multiple sources. Second, some PDs only had partial information publicly available online. While most of the information was available, we could not complete a full analysis with data from all 125 PDs. Another limitation is the lack of available race, and cultural data, which we recognize is a significant component of diversity. This type of data is difficult to assess using publicly available resources. Therefore, this study specifically focused on gender equality within the field.
Future studies could investigate the racial and ethnic backgrounds of PDs and their educational backgrounds. Additionally, further understanding of the associate PD position and current PDs who held this position first should be investigated. Lastly, this study determined the current rank of PDs; however, it could be of interest to assess program directors’ rankings when they were first appointed. Overall, this study helps to understand the current demographics of otolaryngology PDs.
This study showed that female program directors tend to be younger and have served less time in the position compared to their male counterparts. The overall specialty continues to have an underrepresentation of women, but female PDs are represented at a higher percentage than the overall percentage of practicing female otolaryngologists and at an equal rate to practicing female academic otolaryngologists. However, it is important to recognize that this percentage remains much lower than the percentage of females graduating from medical school. While data supports some small improvement in gender equity, continued efforts should be implemented to encourage the advancement of women in leadership within the field to promote better parity and provide increased mentorship to encourage and enable more women to enter the specialty.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.