
Abstract

Significance statement
Anatomic variations in the sinonasal region can cause chronic rhinosinusitis. A large projecting mass-like lesion was discovered in a 78-year-old man during a nasal endoscopic examination. Careful inspection of paranasal computed tomography scans indicated that the ethmoid bulla was very large (a maximum diameter of 1.3 cm and a height of 2.6 cm on coronal view). The patient’s symptoms were completely relieved after functional endoscopic sinus surgery, which included complete removal of the bulla.
Main
A 78-year-old man visited our hospital with the chief complaint of nasal obstruction for the previous 1-month period. He had no history of nasal trauma or surgery, and his symptoms did not improve despite 2 weeks of antibiotic treatment. Anterior rhinoscopy revealed a large swelling mass-like lesion extending anteriorly in the left nasal cavity. Paranasal computed tomography (PNS CT) demonstrated a large ethmoid bulla (with a maximum diameter of 1.5 cm and a height of 3 cm) filled with low-density material. Septal deviation to the right side was also noted (Figure 1). (A) Coronal paranasal CT (PNS CT) revealed a large ethmoid bulla occupying the entire left nasal cavity. (B) Contrast-enhanced coronal PNS CT demonstrated a hyperaerated ethmoid bulla filled with low-density material. (C) Axial PNS CT. (D) Sagittal PNS CT.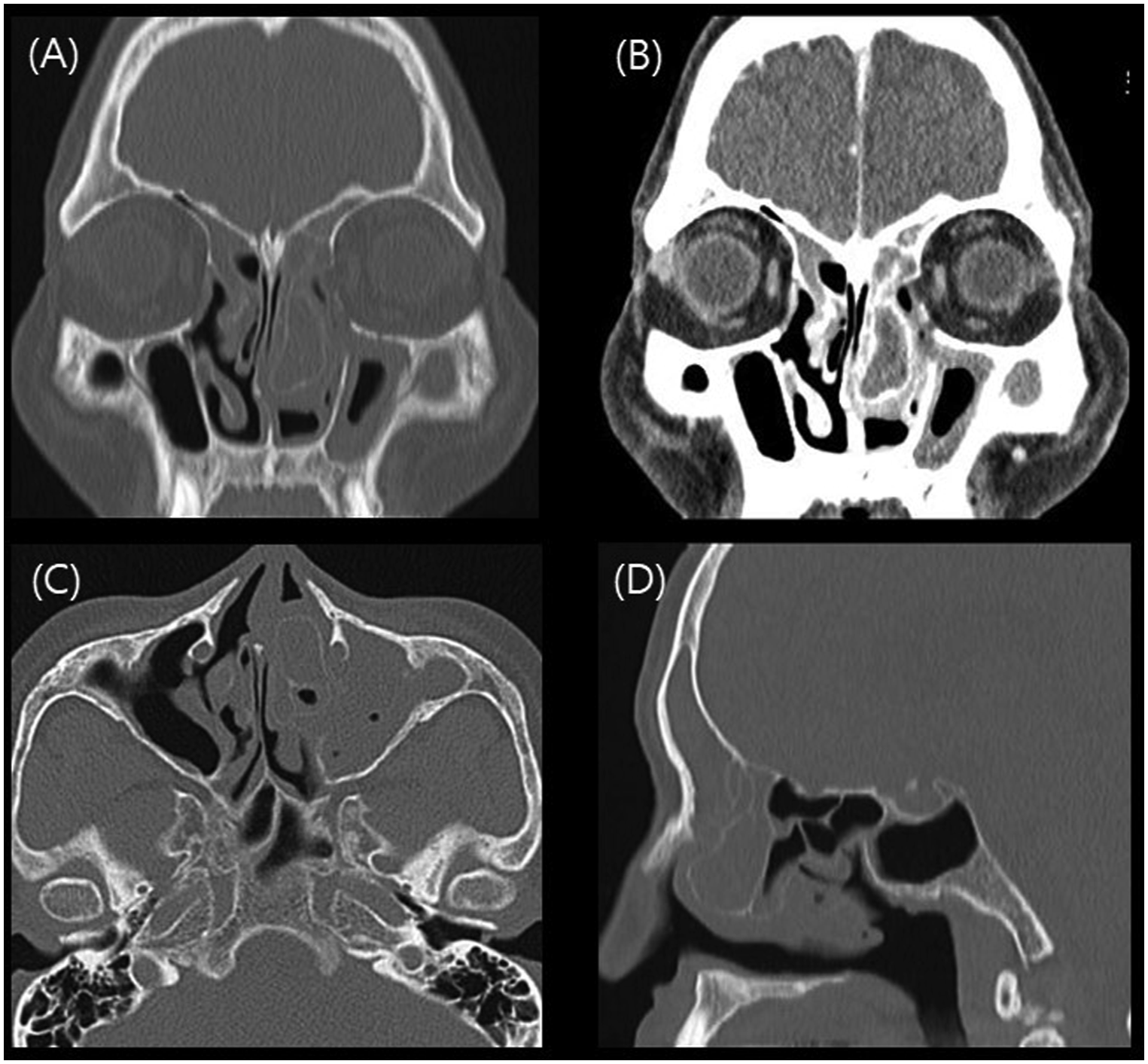
After 3 weeks, the patient underwent elective endoscopic sinus surgery. During surgery, nasal endoscopy detected a large ethmoid bulla, which extended outside the middle meatus and pushed the middle turbinate out posteriorly and the inferior turbinate laterally reducing the size of these two conchae (Figure 2). The bulla was resected by curette and cutting forceps; then, a microdebrider was used to remove all of the ethmoid bone (Figure 3). Left anterior and posterior ethmoidectomy, middle meatal antrostomy, frontostomy and septoplasty were conducted. After 1 month, his symptoms had disappeared completely, and no recurrence was noted after 6 months of follow-up. (A) Preoperative nasal endoscopy revealed the middle turbinate (white arrow), ethmoid bulla (asterisk) and inferior turbinate (black arrow) in the left nasal cavity. (B) 70-degree nasal endoscopic view after ethmoid bullectomy. The middle turbinate (white arrow) and inferior turbinate (black arrow) were well demarcated after removal of the bulla. Photograph of the resected hyperaerated ethmoid bulla tissue.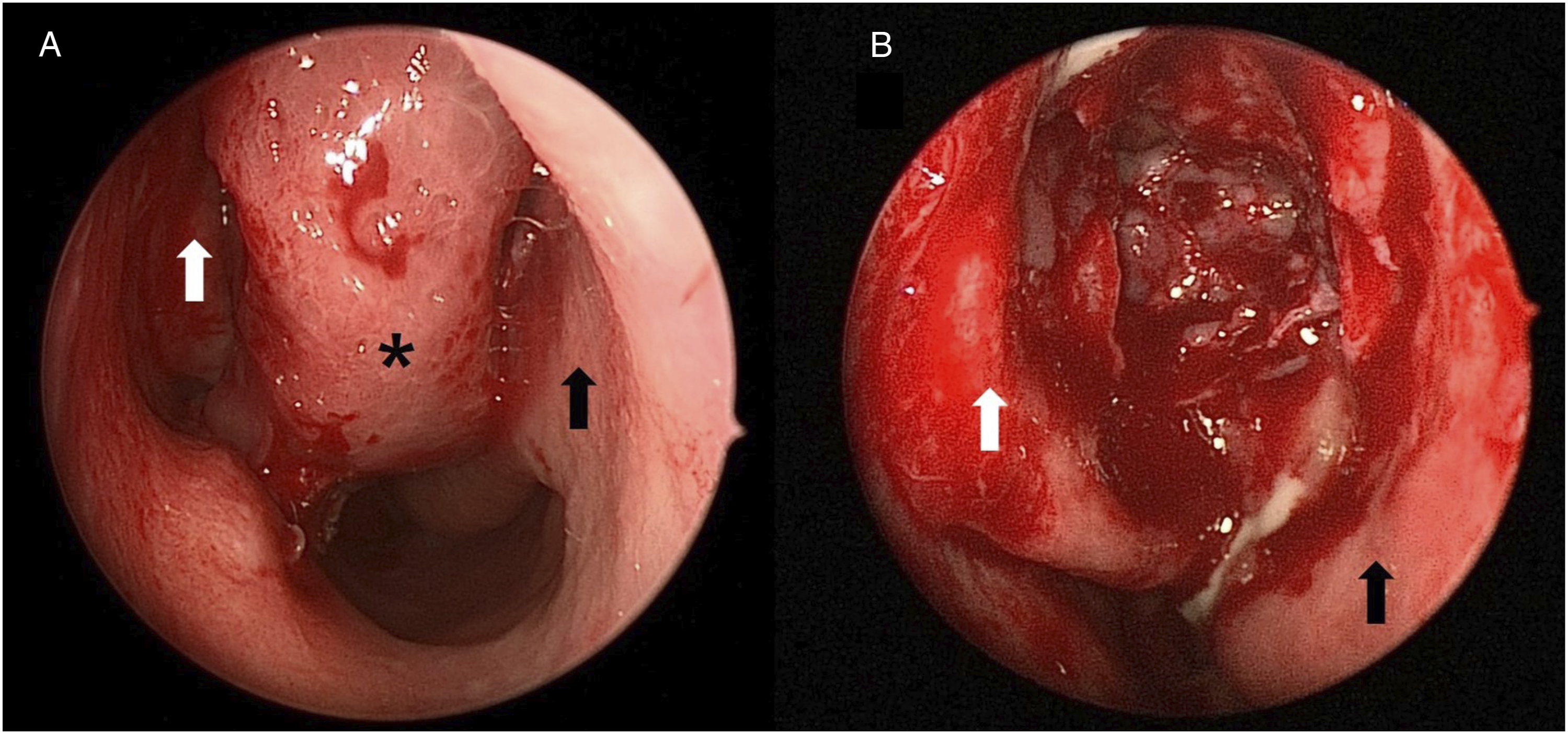

Sinonasal anatomic variations
The ostiomeatal unit (OMU) is the common drainage channel for the frontal, maxillary and anterior ethmoid sinuses and consists of the maxillary ostium, middle meatus and infundibulum.1,2 Any cause obstructing the OMU can hinder sinonasal communication and consequently lead to CRS.
he ethmoid bulla is the largest cell in the anterior ethmoid sinus. If it is sufficiently large, it can push the middle turbinate medially, leading to contact with the nasal septum. Indeed, it may make contact with the septum on its own in rare circumstances and also cause an obstruction in the osteomeatal complex, making the patient susceptible to rhinosinusitis. 3
In our case, a large ethmoid bulla caused obstruction of the OMU and the development of CRS. After surgery, the patient recovered completely from the ethmoid bullectomy.
We report a rare case of a large ethmoid bulla that caused CRS and denominate this hyperaerated ethmoid bulla ‘bulla bullosa’ from the phrase ‘concha bullosa’ (i.e. pneumatized middle turbinate).
The otolaryngologist should be as familiar as possible with any anatomic variations in the sinonasal region to prevent intraoperative complications in endoscopic sinus surgery. As part of this, careful reviewing of preoperative computed tomography scans cannot be overemphasized. We hope our case report will be helpful to otolaryngologists who specialize in the nasal region.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the fund of Biomedical Research Institute, Jeonbuk National University Hospital.