
Abstract
Langerhans Cell Histiocytosis is a rare disorder characterized by an abnormal proliferation of Langerhans cells in one or multiple organs. It rarely presents with a central vestibular involvement. We report a case of a multisystem Langerhans Cell Histiocytosis with mucosal, hepatic, and neurological involvement, presenting with dizziness and balance disorders. A 39-year-old woman with a histopathologically confirmed mucosal palatal Langerhans Cell Histiocytosis presented with a history of dizziness for a year. Vestibular examination revealed a saccadic eyes pursuit, an up beating spontaneous nystagmus, a bilateral gaze nystagmus and a prolonged positional nystagmus, in the supine roll test. Pure tone audiometry showed a slight left sensorineural hearing loss at the 8000 Hz frequency. Computed tomography (CT) scan showed a bilateral maxillary sinus fullness and a peripheral osteosclerosis of the surrounding bony walls. Hepatic magnetic resonance imaging (MRI) showed a typical hepatic involvement with a hepatomegaly with countless cysts. Temporal bone CT scan and MRI were normal. Cerebral MRI showed an hyperintense nodular signal at T2 FLAIR weighted images lateral to the right pons, at the level of the left middle cerebellar peduncle and at the left mesencephalon. Balance disorders can rarely present a sign of a degenerative neurological cerebellar involvement. Such a rare manifestation can present in different neurological disorders such as Langerhans’ cell Histiocytosis.
Introduction
Langerhans Cell Histiocytosis (LCH) or Histiocytosis X is a rare disease of unknown etiology. It mainly affects children and young adults, with a clear male predominance. 1 The most common histological feature is clonal proliferation of abnormal histiocytes. 2 LCH can cause permanent consequences linked to the disease sites in up to 50%. 3 Bone is the most commonly affected organ either in adults or children followed by skin, oral mucosa, lungs, spleen, and lymph nodes.4,5 Oral and maxillofacial region involvement present with orofacial pain and a bony or soft tissue lesion. 2 Hepatic and central neurological system (CNS) abnormalities are rather rarely reported. 4 Tumorous form of central nervous LCH affects most commonly the hypothalamic-pituitary axis while the neurodegenerative form is rather rare and mainly present with a cerebellar deficit.5,6 We report a case of a confirmed multisystem Langerhans Cell Histiocytosis with mucosal and hepatic lesions presenting with dizziness that we think is related to the pontine and cerebellar degenerative lesions.
Case Report
We report a case of a 39-year-old woman with a medical record of mild intermittent allergic rhinitis, who presented to our department with a history of spontaneous dizziness and unsteadiness that had been evolving for a year. She reported that dizziness was exacerbated by head motion, change in position in bed or by complex visual stimulation. In addition, she had sometimes an external vertigo described as a false sense of rotational motion and a false sense of linear motion. The patient did not report a history of a head trauma or familial deafness. She did not complain neither of nausea and vomiting nor of headache, tinnitus, or a sensation of ear fullness.
Examination of the oropharynx and oral cavity showed a right palatal ulceration. Ocular examination showed a saccadic pursuit, a left hypermetria, a spontaneous up beating nystagmus (Figure 1), and a bilateral gaze nystagmus. No convergence insufficiency was found. The head impulse was positive on the left side and the head-shaking test induced a left beating nystagmus Videonystagmography showing a spontaneous up beating nystagmus (A) and a left beating nystagmus at the head-shaking test (B).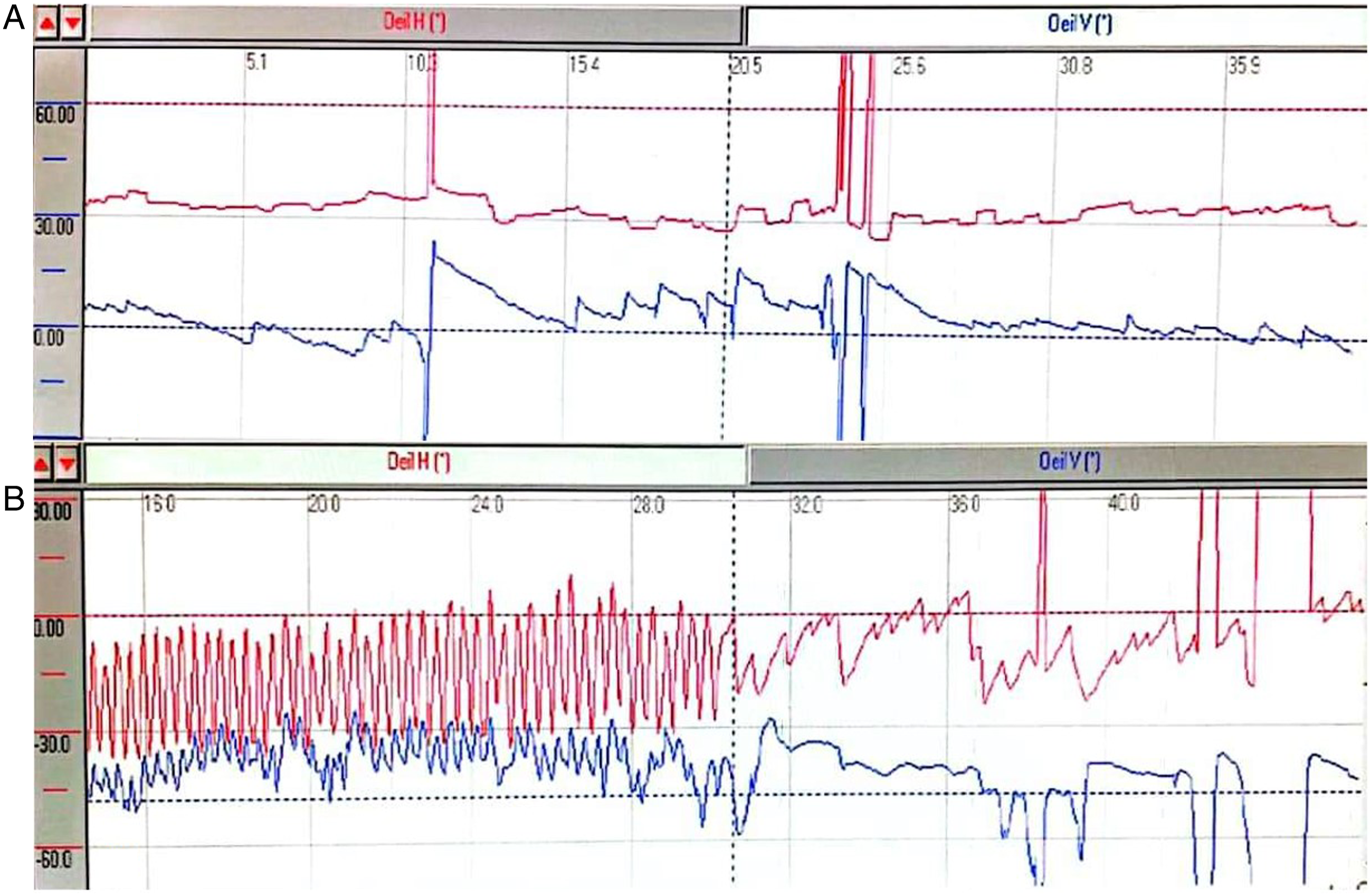
Biopsy of the palatal ulceration was performed; histopathological examination revealed the accumulation of histiocyte-like cells that were positive for CD1a and S-100. (Figure 2) Accordingly, the diagnosis of LCH was confirmed. A whole-body computed tomography (CT) showed a hepatomegaly with innumerable hepatic cystic formations suggestive of simple biliary cysts. It also revealed a filling of the left frontal sinus and the right maxillary sinus with peripheral osteosclerosis and thickening of the surrounding bony walls (Figure 3). A tissue infiltration by clear histiocyte cells and eosinophils (A: H&E *40). At immunohistochemical staining, Langerhans cells were positive for CD1a (B). (A) Axial Computed tomography of paranasal sinuses, bony window, opacification of the right maxillary sinus with an osteosclerosis, and a thickening of its bony walls. (B): Hepatic MRI, T1 weighted sequences, multiple hepatic cystic formations, with variable sizes and a decreased T1 signal. (C): Axial cerebral MRI, T2 FLAIR weighted sequences, ischemic left mesancephalic lesions appearing as high signal nodules (Red arrow). Abbreviation: MRI, magnetic resonance imaging.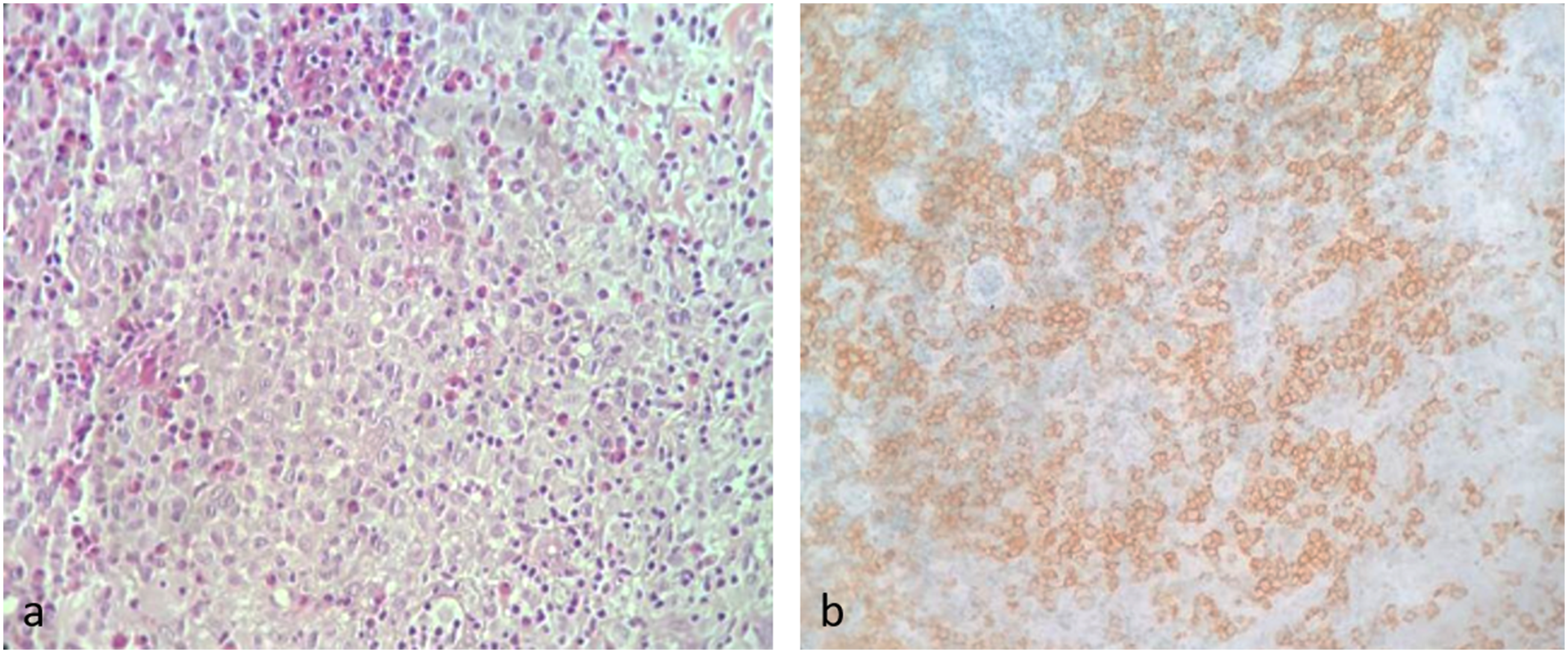
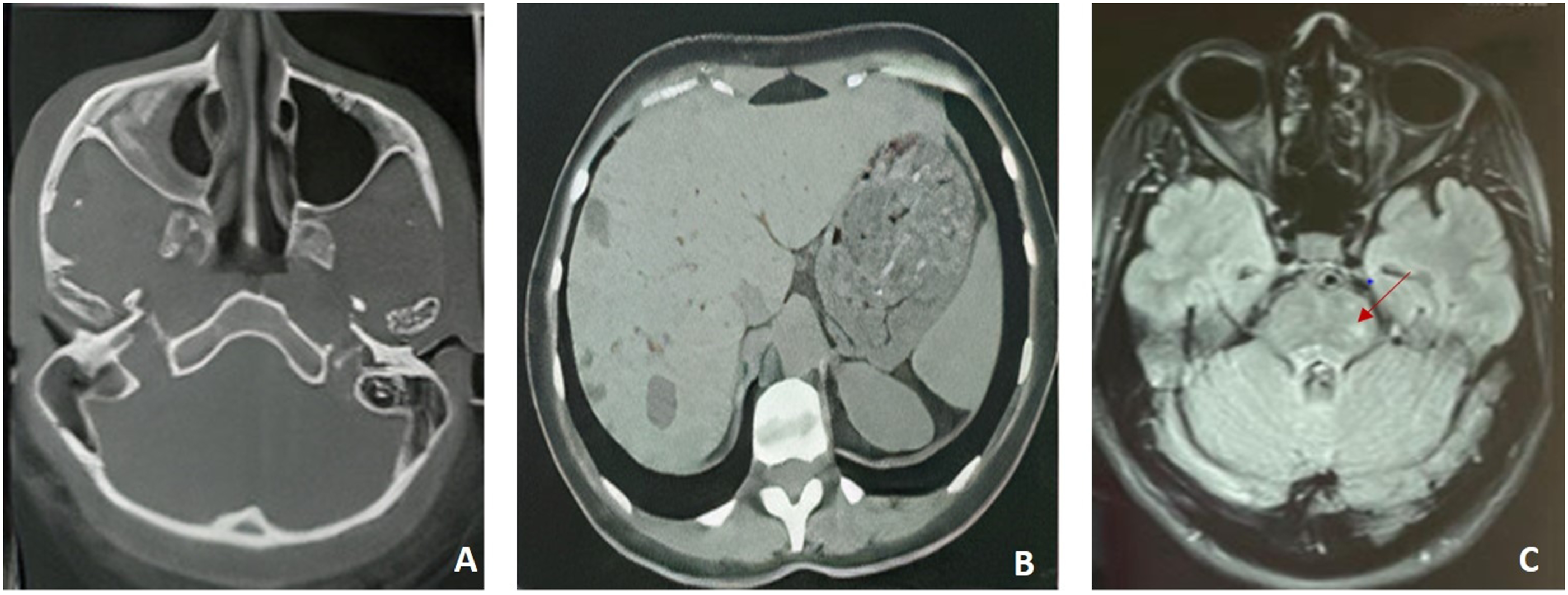
Computed tomography did not reveal pulmonary or cerebral parenchymal abnormalities or bone lesions suggestive of LCH. Hepatic MRI showed hepatomegaly and the presence of countless cysts with variable sizes (Figure 3). Temporal bone MRI was normal and did not reveal any abnormality of the inner ear and the cerebellopontine angle. Cerebral MRI showed a normal pituitary gland and hyperintense nodular signal at T2 FLAIR weighted images lateral to the right pons and at the level of the left middle cerebellar peduncle and mesancephalon, that did not enhance after Gadolinium injection, all suggestive of LCH (Figure 3).
The balance disorder reported by our patient associated with the vestibular abnormalities found at the physical examination were attributed to a central cause, specifically histiocytosis-related cerebellar lesions in the context of a degenerative disease.
Discussion
Langerhans cell histiocytosis (LCH) is a rare disorder defined as the infiltration of one or multiple organs by Langerhans like cells. 4 It mainly occurs as a sporadic form; rare cases of familial forms were reported. 7 LCH can affect patients of very different groups of age. The incidence is reported to be the highest in infants as it decreases with age. 8 LCH presents as a single system disease featuring only one organ in 70% of cases; multi system forms are less common.9,10 LCH mainly presents with bony lesions, whether unique or multiple. 4 It affects the craniofacial skeleton in 30 to 50% of cases, at the level of the arch and at the base of the skull, the facial mass, or the mandible.2,11,12 Cutaneous, mucosal, hypothalamo-pituitary, and endocrine abnormalities are also common. 4 In oral cavity, LCH manifests as single or multiple lesions affecting the alveolar or cortical bone, associated to ulcerated mucosal lesions and periodontal lesions. 13 These lesions can encroach on adjacent structures and cause orbital, gingival, central nervous system (CNS), or middle ear symptoms. 4 Isolated pulmonary forms are mainly seen in adults and are associated to smoking. However, forms with hepatic, gastrointestinal, neurological, and hematological lesions are less commonly declared.4,14
Findings in our case report included a typical mucosal ulceration at the oral cavity with liver lesions suggestive of LCH. Our patient also presented with dizziness which is uncommonly reported in LCH cases in the literature; their causes are still controversial and under discussion. Nakamural et al 15 reported that the 3 main possible causes of disorientation and instability associated with LCH are vestibular dysfunction due to direct involvement of the inner ear, a direct infiltration or compression of the cerebellum, or a brainstem dysfunction associated with paraneoplastic syndrome. In our case, imaging and physical examination findings were not suggestive of inner ear involvement or a paraneoplastic syndrome. However, we noted the presence of pontine and cerebellar nodules at the cerebral MRI that were suggestive of a degenerative disease.
Neurological involvement occurs in 10–25% of LCH patients, either as a tumorous form or less frequently as a neurodegenerative form. 5 Clinical manifestations depend on the affected site with hypothalamic-pituitary-adrenal axis being the most commonly affected region. It manifests in this case with diabetes insipidus (DI) and anterior pituitary dysfunction.5,16 Tumorous forms are known to present with focal neurological signs. 17 In these LCH forms, parenchymal lesions occur most frequently in the posterior fossa especially in the cerebellar peduncles alongside the brainstem. These cases manifest with ataxia, dysarthria, and bulbar deficits. 5 As for neurodegenerative forms, they also mainly affect the posterior fossa. Central cerebellar involvement is more common in children while only few cases were reported in adults. 4 Neurodegenerative forms can be asymptomatic or can manifest with a slowly progressive cerebellar syndrome and cognitive and behavioral dysfunction in adolescents and children while adults rather mainly develop cerebellar ataxia.5,17Cerebellar histiocytosis forms are in fact characterized by a variability in their clinical presentation and could mimic other diseases such as hereditary ataxia. 17 Clinical manifestations range from a subtle tremor to ataxia, dysarthria and psychomotor disorientation. 18 Thus, the diagnosis of cerebellar NCH based on clinical findings is challenging especially in the cases where cerebellar ataxia is the initial symptom presented by the patient. Cerebellar ataxia in LCH mainly appears in association with other symptoms or during the progression of a confirmed LCH. 19
Different MRI patterns and abnormalities of CNS involvement secondary to LCH have been described. The most common is the hypothalamic-pituitary granuloma followed by the neurodegenerative LCH, characterized by bilateral symmetric alterations of variable signal intensity located in the cerebellar gray matter, sometimes extending to the underlying white matter, in the basal ganglia and brainstem. 20 The cerebellar histiocytosis typically presents on MRI with bilateral and symmetrical lesions with an increased signal on T2-weighted images, located in the dentate nucleus, cerebellar peduncles, and cerebellar white matter alongside with signal abnormalities in the posterior pons; Enhancement after Gadolinuim injection is variable.17,18 However, these MRI findings remain not pathognomonic of cerebellar LCH. There is also a great discrepancy between the clinical and the radiological involvement; radiological abnormalities may in fact precede clinical manifestations, while a subtle impairment might not be demonstrated by MRI.5,21
As for our patient, MRI revealed typical hyperintense nodular signal at T2 FLAIR weighted images lateral to the right pons and at the level of the left middle cerebellar peduncle that did not enhance after Gadolinium injection. Thus, based on our vestibular examination, histopathological findings, and MRI, we linked the balance disorders presented by our patient to a multisystemic LCH in the context of a neurodegenerative involvement.
Conclusion
We reported a case of a confirmed multisystem Langerhans Cell Histiocytosis with mucosal, hepatic involvement that presented with dizziness which was attributed to a cerebellar LCH involvement. Central nervous system involvement in Langerhans Cell Histiocytosis is a rare entity. Cerebellar involvement is not common. Diagnosis of cerebellar LCH is challenging. It manifests with a slowly progressive ataxia. Other associated symptoms at initial presentation, a confirmed LCH in another site and MRI findings help to attribute dizziness to LCH.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient for her anonymized information to be published in this article.