
Abstract
Fourth branchial cleft anomalies are rare head and neck congenital lesions seen in children. They present as a neck inflammatory mass and arise essentially on the left side of the neck. We report the case of a 7-month-old female with a mass of the neck associated with respiratory distress. The mass was diagnosed as an incomplete fourth branchial cleft fistula. Surgical revision of the neck abscess from an external approach and plasma coblation of the orifice in the pyriform fossa by an endoscopic approach were performed.
Keywords
Introduction
Fourth branchial cleft anomalies are congenital anomalies of the branchial apparatus. The branchial apparatus arises in the area of the primitive pharynx by the 4th week of embryonic life. Abnormal development of the branchial apparatus gives rise to fistulas (abnormal passageways with inner and outer orifice between the pharynx and the skin), sinuses (formations with inner or outer orifice and blind ending tract), and cysts (globular or oval-shaped formations without the orifice). Branchial anomalies are not rare in children, and the most common (80–95% of total) are second branchial cleft and pouch anomalies.1–3 On the other hand, fourth branchial cleft anomalies are rare. Due to their rare occurrence, such anomalies can be misdiagnosed or diagnosed late. In this article, we report the case of a 7-month-old female presenting a mass of the neck associated with respiratory distress and caused by a rare anomaly of the fourth branchial cleft.
Case presentation
A 7-month-old female was referred to the Department of Paediatric Otorhinolaryngology. The patient presented rhonchopathy from birth and 3 days of hoarse breathing with inspiratory stridor, worse when crying or in a position on her right side. Flexible endoscopy was performed, and no signs of laryngomalacia were detected.
Whitin 1 month swelling had by arisen on the left side of the neck. Ultrasound examination revealed a bilobular 25 mm mass, which had pushed the sternocleidomastoid muscle away and had propagated dorsally behind the left lobe of the thyroid gland to the esophagus. Its content was heterogeneous and gas bubbles were suspected. The patient was admitted to the pediatric department. Laboratory findings indicated leukocytosis, mild anemia with thrombocytosis, and low CRP. Microbiological examination of a throat swab revealed extended-spectrum beta-lactamase (ESBL) E. coli. The stridor was present only when crying. A magnetic resonance imaging (MRI) scan of the neck (Figure 1(a)) revealed the mass expanding to the hypopharynx, larynx, esophagus, and carotid sheath. According to the findings, a tumor was suspected, and the multidisciplinary commission decided to perform a biopsy. The material was sent for histopathological exam and the content was sent for cultivation. The result of the cultivation was negative. The patient was treated by antibiotic therapy and was dismissed in good condition on the 5th day after the surgery. Imaging of the fourth branchial cleft sinus. (a) Coronal MRI scan (T2-weighted image). (b) Imaging of the fourth branchial cleft sinus – video fluoroscopy. (c) Injection of the contrast agent through orifice of the fourth branchial cleft sinus.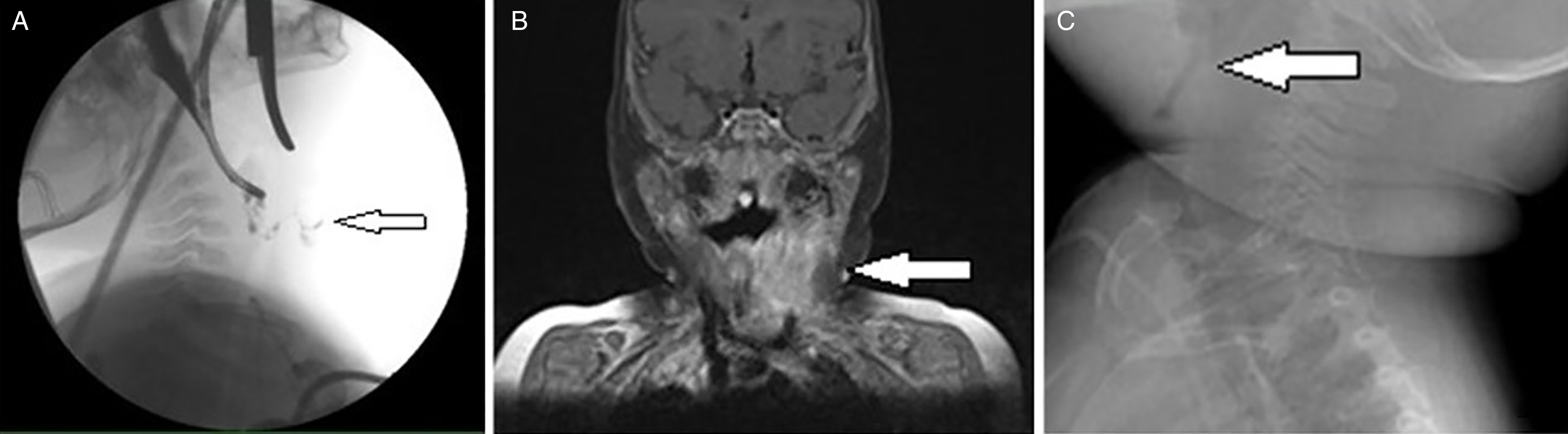
The histopathological examination confirmed a parapharyngeal abscess, containing varied mixture of cells and the foreign nourishment material.
Suddenly, the neck mass started to grow progressively. An abscess formation with pus and visible through the skin appeared on the left side of the neck. A video fluoroscopy exam revealed a fistula between the pyriform recess and the mass on the left side of the neck (Figure 1(b)). Hypopharyngoscopy and laryngoscopy were performed under general anesthesia, revealing an orifice in the left piriform recess and the fistula bounding to the neck mass. Subsequently, the fistula was examined and fistulography was performed using contrast agent (Figure 1(c)).
The orifice of the sinus was closed by plasma coblation using a Coblator II device and laryngeal probe. At the same time, incision and drainage of the subcutaneous abscess formation was performed from the external approach. The patient presented no complication and she was discharged on the 7th day after surgery. Revision surgery was performed 2 months after the primary surgery. The area in the pyriform recess had healed completely. At the 6-month follow-up (with check-up every month), there was no evidence of recurrence (Figure 2). Orifice of the fourth branchial cleft sinus (arrow), viewed by video laryngoscope. (a) Orifice before plasma coblation – open. (b) Orifice after coblation – closed. (c) Orifice 2 months after coblation – completely healed.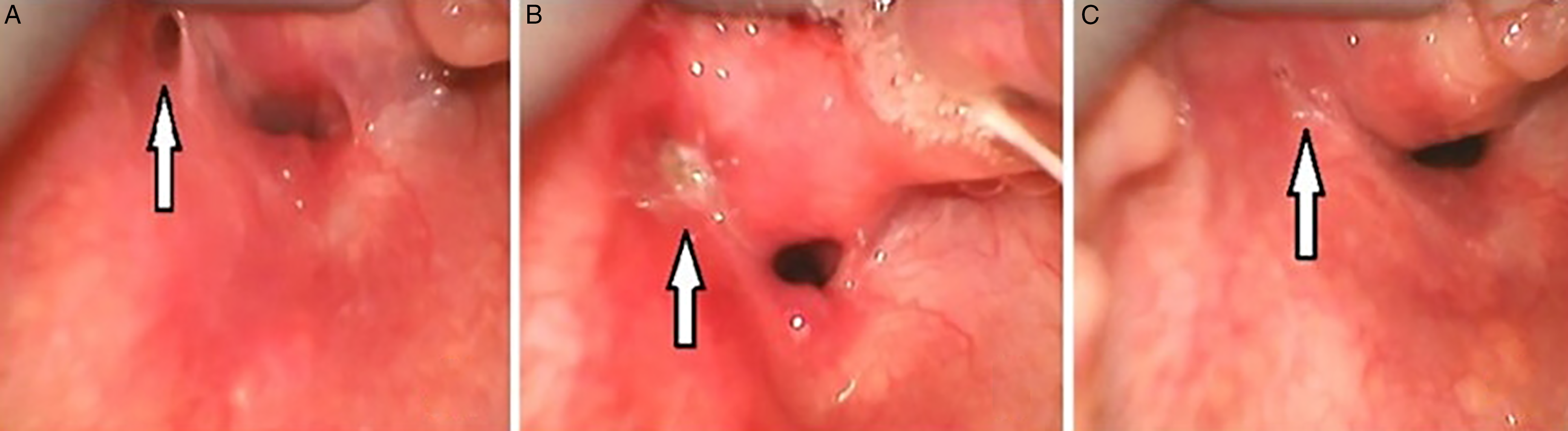
Discussion
Fourth branchial cleft anomalies are extremely rare pathologies. To date, just over 100 such cases have been described 4 . They usually are found on the left side of the neck, probably due to the asymmetric vascular development of the adjacent arches. They manifest predominantly as a sinus with the internal orifice in the apex of the pyriform recess and a blind-ending tract reaching to any point of its theoretical course.
Those anomalies occur in different age groups and their clinical manifestations are diverse.4,5 Approximately 9% of cases appear in neonates, presenting as neck mass. Manifestations can be asymptomatic or they can present as respiratory or swallowing problems caused by compression of the upper respiratory or digestive tract. 6
Most authors consider ultrasound examination most helpful. A CT scan usually does not provide more information than does ultrasonography. 2 Although MRI can be used to measure the anomaly and depict its course, its result can be misleading, as in our case. For these reasons neither CT nor MRI scan can be recommended as the first-line imaging modality. 7
Video fluoroscopy with iodinated contrast agent was used for swallowing contrast study in our case. Although some authors recommend barium swallow study, this is contraindicated in our opinion, and especially when the diagnostic process is ongoing and digestive continuity disorder cannot yet be excluded.
In our opinion, laryngoscopy with flexible or rigid endoscope is the most useful method for diagnosis of the anomaly.
The curative treatment is surgical, and both open and endoscopic approaches have been described. One option is complete surgical excision from an external approach and eventually to perform partial or total thyroidectomy.
A second option is endoscopic closure of the internal orifice. Most commonly, this is done by cauterizing with, for example, CO2 laser,8,9 monopolar diathermy, KTP laser, fibrin glue, 10 10% trichloroacetic acid, 11 or silver nitrate. 11
Attitudes regarding the best therapeutic procedure in such cases are not uniform. Li et al. conducted a study with 10 patients and preferred complete surgical excision. In their view, the results of cauterization were not convincing. 12 Watson et al. treated 5 patients by cauterizing the internal orifice of the sinus. At 25-month follow-up, no complications or recurrences were detected. 11 In a meta-analysis, Derks et al. compared the efficacy of cauterization versus open surgery. They found that the success rate of cauterization in terms of preventing recurrence was comparable to that for surgical treatment. They prefer endoscopic cauterization of the internal orifice as the primary treatment, because the risk of peri- and postoperative complications is then lower.3,10
Due to the small numbers of patients in the studies described above, it is difficult to compare the methods. Both general methods bear risk of injuring the surrounding structures. Hoarseness is the most common complication after surgery. 13
In our case, we performed coblation of the internal orifice by plasma, using the Coblator II device and a special probe that creates a plasma field at its end and operates in the range 40–70°C. The incision and drainage of the inflammatory neck mass were performed in a single operation. We observed no complications related to healing or recurrence. Cases in which endoscopic cauterization is combined with drainage of the neck abscess are described but rarely and the number of patients in such studies is low (maximally 3 patients in a group). Different recurrence rates have been detected in the range of 0–100%.14,15
Conclusion
Fourth branchial cleft anomalies are rare congenital anomalies of the branchial apparatus. The diagnosis is based upon endoscopic demonstration of the internal orifice and the fistula or sinus using contrast agent. Closure of the internal orifice by plasma coblation in combination with treating the abscess formation from an external approach constitutes a successful treatment method.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Health, Czech Republic - conceptual development of research organization (FNBr, 65269705) and Masaryk University Brno (MUNI/A/1132/2021).
Informed consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.