
Abstract
Chronic airway foreign bodies represent a rare and challenging entity faced by otolaryngologists. Herein, we describe the case of an adult woman found to have a 17 cm-long internalized tracheostomy stay suture retained 2 years after decannulation. Thorough evaluation and contingency planning allowed for safe and successful removal of this novel airway foreign body. The selective use of stay sutures in adult tracheostomies and proper peri-operative care may have prevented its incidence.
Introduction
Although more common in pediatric patients, foreign bodies in the adult tracheobronchial tree may be encountered in at-risk populations. Similar to children, the acute onset of symptoms associated with a suspicious aspiratory event is the strongest clinical predictor for their presence. 1 Chronic, or occult, tracheobronchial foreign bodies represent a rare and challenging entity that often present with non-specific symptoms like prolonged cough or dyspnea. As a result, their diagnosis may be delayed and lead to serious complications including granulation formation, endobronchial stenosis, or recurrent pneumonias.1-3
The placement of temporary stay sutures during tracheostomy procedures are designed to assist with intraoperative exposure and management of unplanned post-operative decannulation events. While their utility in pediatric tracheostomies is well supported, others advocate for routine stay suture placement in adult tracheostomies.4,5 Herein, we describe a case of a retained, internalized tracheostomy stay suture presenting as a chronic airway foreign body in an adult and discuss the nuances related to its removal.
Case Report
A 64-year-old female was referred to our clinic for symptoms of dysphagia, hoarseness, and globus sensation of 2 years. Relevant history includes a motor vehicle accident trauma, for which she required both tracheostomy and percutaneous endoscopic gastrostomy (PEG) at an outside hospital. After adequate recovery, she was decannulated and the PEG tube was removed, but her dysphagia and globus persisted. In-office flexible fiberoptic laryngoscopy revealed a crusted suture-like material (∼5 cm) coiled in the supraglottis. The terminal ends of the material could not be identified as they were embedded in the mucosa of both the hypopharynx and subglottis. Outside records were obtained and the operative reports from the tracheostomy and PEG described the placement of “bilateral 2-0 tracheal sutures” to “provide tracheal exposure.” No additional documentation regarding tracheostomy care or decannulation was available.
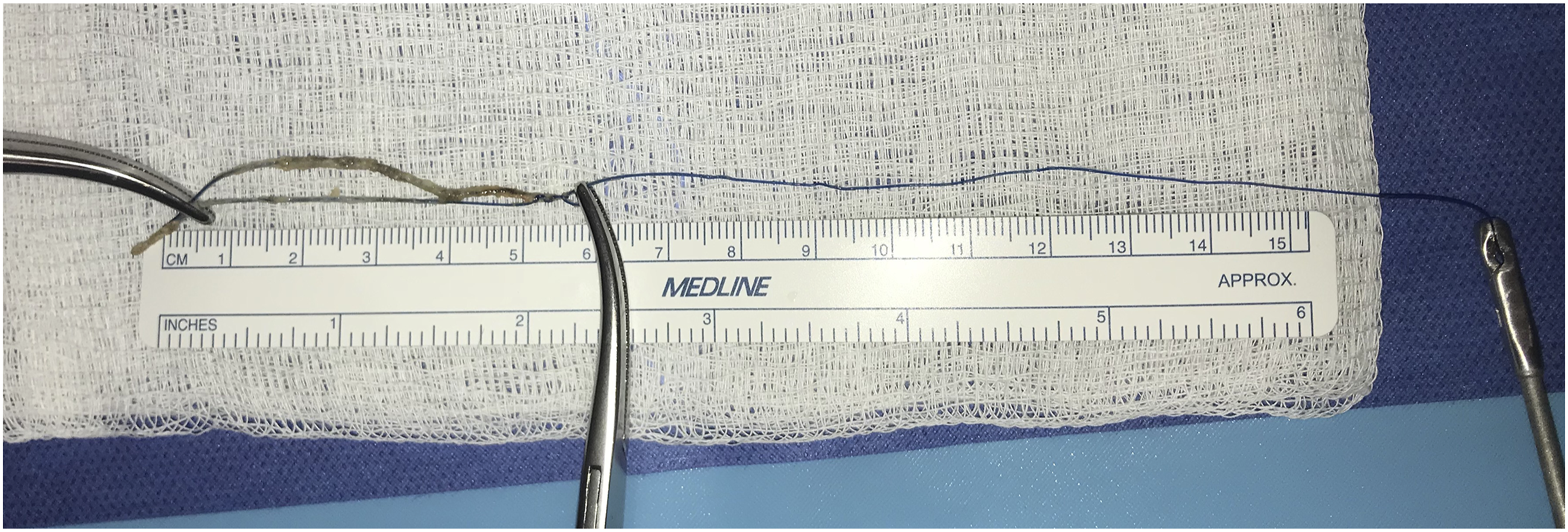
We proceeded with urgent direct laryngoscopy, rigid esophagoscopy, and bronchoscopy using the operative telescope. Intraoperative exposure revealed blue Prolene-like suture material coiled in the supraglottis with transglottic, subglottic, and esophageal extension (Figure 1A). Rigid esophagoscopy demonstrated that the material ended freely in the proximal esophagus. Bronchoscopy showed that the foreign body was held by a loop through the anterolateral tracheal wall (Figure 1B). No tracheal and bronchial irregularities or additional material were seen distally. To release it from the trachea, one limb of the loop was cut with using microlaryngeal scissors and the other limb was pulled out of the operative laryngoscope. Inspection of the removed foreign body showed a Prolene suture of over 17 cm in length (Figure 2). The patient tolerated the procedure well and was discharged home the same day. At her 1-month follow up appointment, she reported complete resolution of her symptoms without evidence of long-term sequelae on flexible fiberoptic laryngoscopy. (A) Intraoperative view using the operative telescope revealing blue suture material traversing the glottis and extending into the subglottis and trachea. (B) The looped suture material with a single trans-mucosal adherence to the anterolateral tracheal wall. Removed foreign body placed over a surgical sponge and stretched using surgical instruments to demonstrate its length of roughly 17 cm.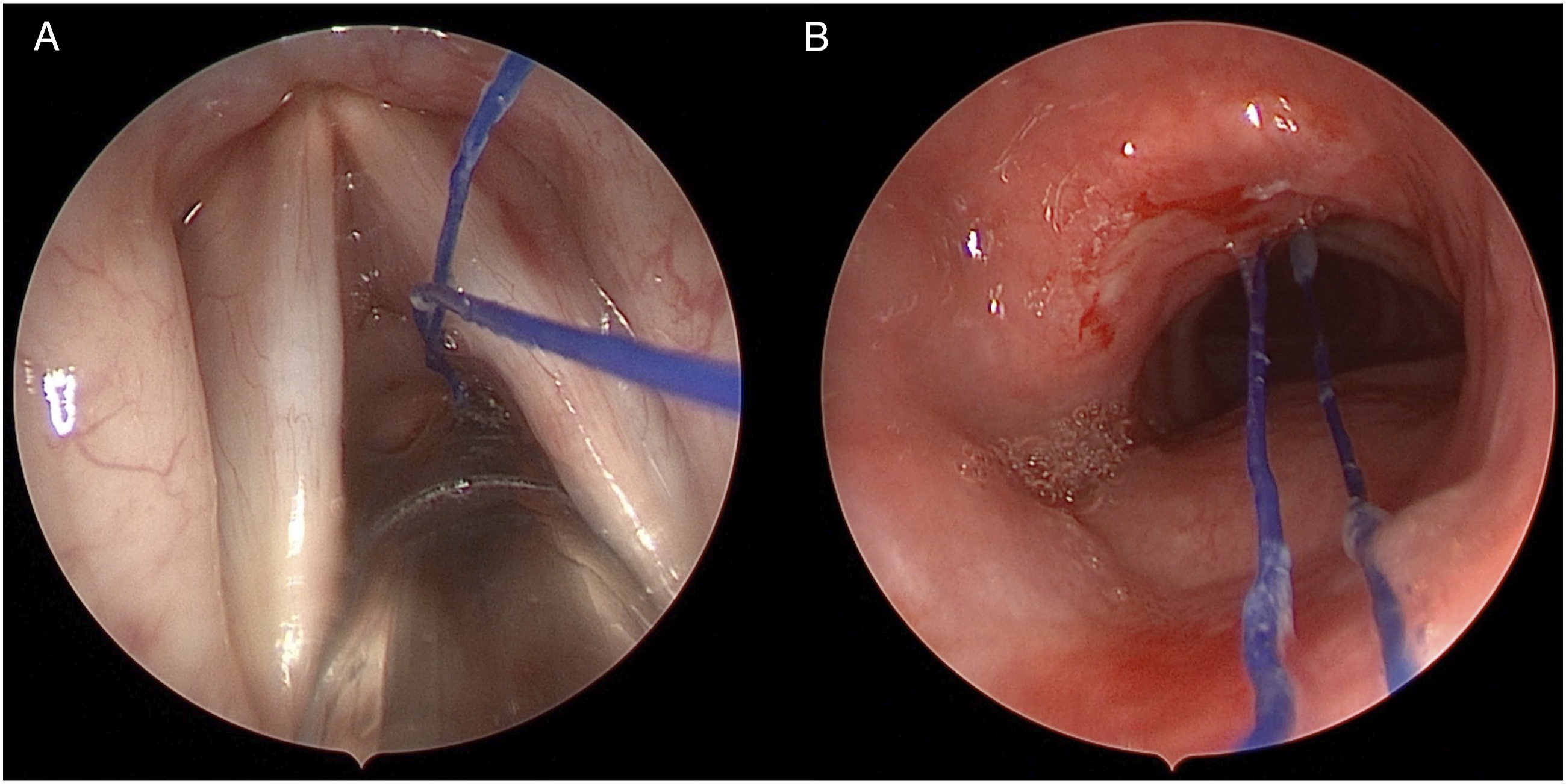
Discussion
To the authors’ knowledge, this is the first reported case of a retained tracheostomy stay suture presenting as an airway foreign body. Our team hypothesizes that the suture was internalized during the tracheostomy placement or initial tracheostomy change. After decannulation, the internalized suture remained in the granulated tracheostomy site and the patient likely coughed it proximally where it resided in the supraglottis and extended into the esophagus during swallowing.
Although stay sutures are not frequently placed during adult tracheostomies, several reports have proposed their routine use.4,5 The authors of this paper discourage the regular deployment of this technique in adult patients and instead recommend alternative options, such as Bjork flap creation, when problematic anatomy is encountered. Ancillary strategies including standardized tracheostomy care protocols and nursing education have been shown to reduce the incidence of accidental decannulation, diminishing the advantages of stay sutures. 6 When sparingly used, institutional practices like head-of-bed signs and on-person labeling should be employed to mitigate this problem from occurring again.
In addition to describing a novel airway foreign body, this case highlight many tenants of foreign body removal, peri-operative tracheostomy care, and preparation for decannulation that have the potential to go overlooked. With an uncertain preoperative etiology, complete laryngeal, esophageal, and bronchial evaluation were paramount. Amid symptoms of dysphagia and a history of a PEG, an intra-esophageal or intra-gastric suture was among the preoperative differential. Both trauma and thoracic surgery teams were available in the event intraoperative complications were encountered. The patient was counseled and consented for an open approach (neck exploration and thoracotomy) for emergency precautions. Adverse outcomes have been reported from the removal of endobronchial sutures from prior cardiothoracic surgery.1-3 Thus, we advocate that the removal of chronic airway foreign bodies should only be performed at centers with broad surgical subspecialty capabilities. Further, retrieval of any airway foreign body should not be attempted in an awake patient in the office or bedside setting to avoid life-threatening complications of dislodgement and distal advancement.
This case emphasizes the importance of flexible tracheosbronchoscopy following tracheostomy placement, which is standard of practice at our institution. In addition to confirming appropriate tracheostomy position, tracheosbronchoscopy provides direct visualization of the distal airway and may exclude the presence of iatrogenic foreign bodies. This may prove even more valuable in critically-ill or unresponsive patients unable to communicate abnormal symptoms, as was likely in this case. Finally, this underlines the importance of laryngeal examination during the decannulation process, as clinicians should evaluate vocal cord mobility and the presence subglottic stenosis. If laryngeal evaluation is out of the scope of practice for physicians performing tracheostomies (i.e., in the critical care setting), institutional protocols for proper referral should be implemented. The utility of this practice will continue to gain significance with the rising incidence of percutaneous tracheostomies being performed.
Footnotes
Author Note
Exemption was obtained from the Cooper Health System Institutional Review Board for the material herein.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.