
Abstract
Significance Statement
The literature describing oropharyngeal papillary squamous cell carcinoma (OPSCC) is limited, and when coupled with this patient’s lack of risk factors and unusual location in the scar of the distant cleft palate, repair makes for a very interesting clinical presentation. This report will support previous literature and signal further investigation into the pathophysiology of papillary squamous cell carcinoma arising within the oropharynx.
Clinical Report
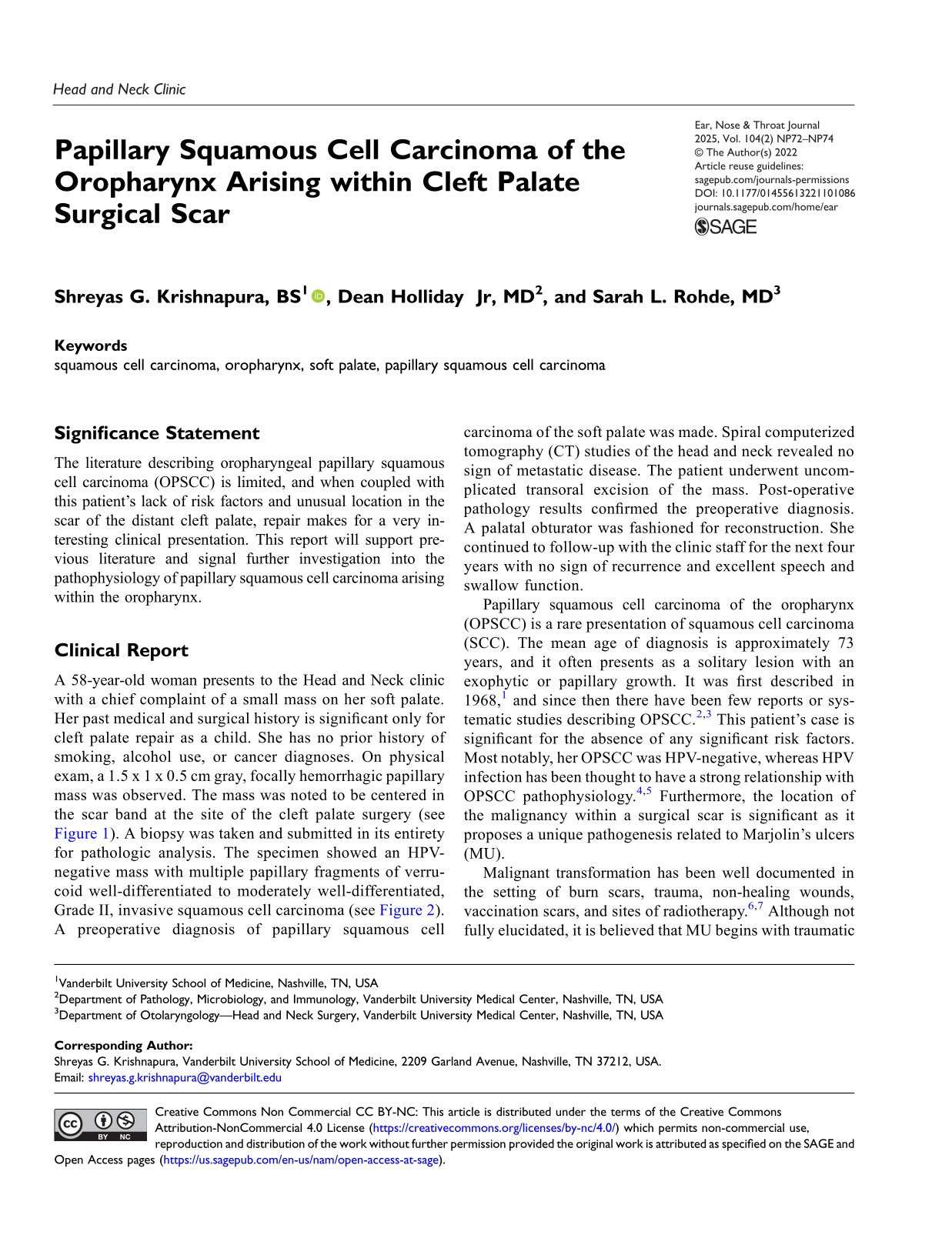
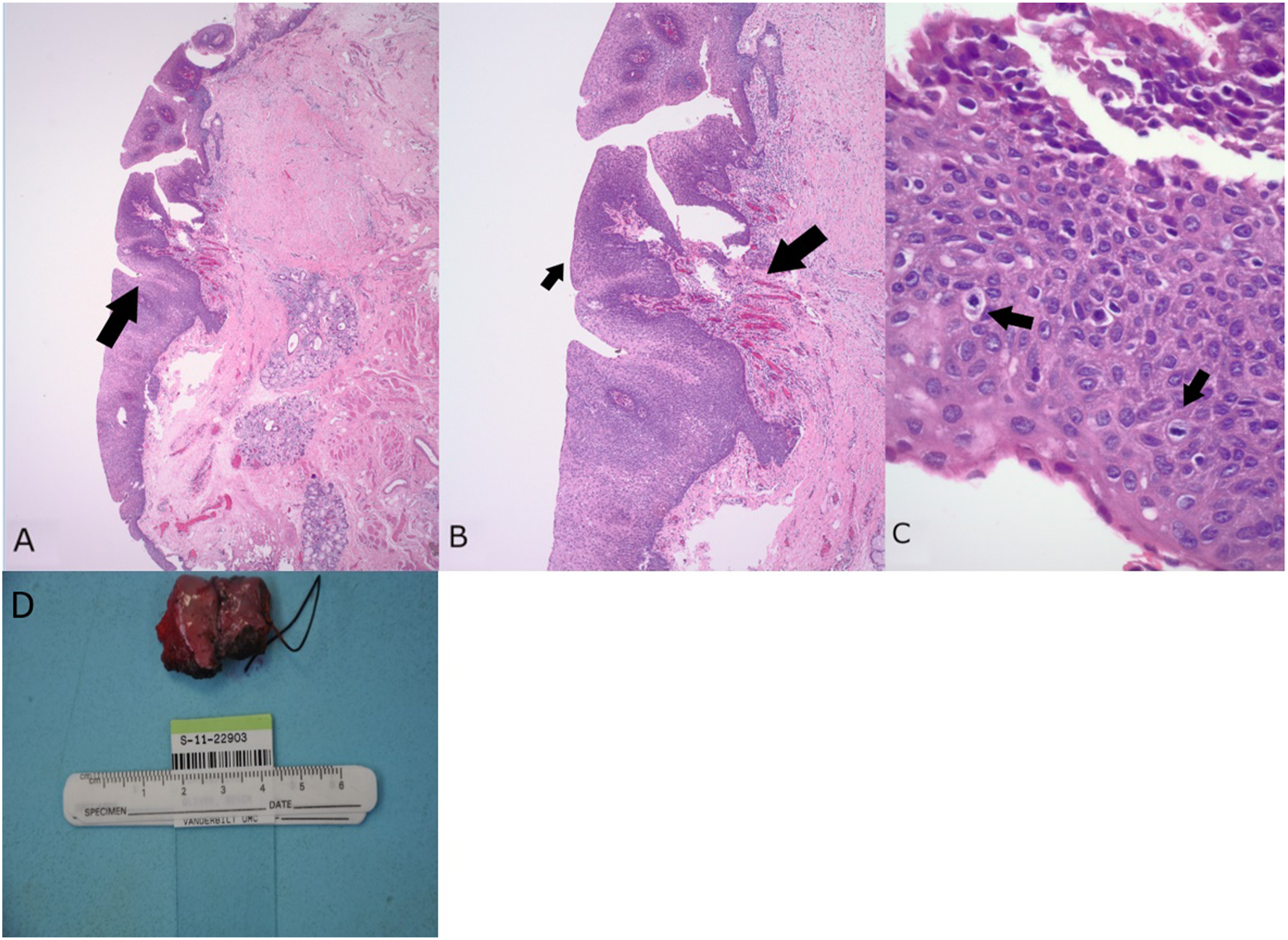
A 58-year-old woman presents to the Head and Neck clinic with a chief complaint of a small mass on her soft palate. Her past medical and surgical history is significant only for cleft palate repair as a child. She has no prior history of smoking, alcohol use, or cancer diagnoses. On physical exam, a 1.5 x 1 x 0.5 cm gray, focally hemorrhagic papillary mass was observed. The mass was noted to be centered in the scar band at the site of the cleft palate surgery (see Figure 1). A biopsy was taken and submitted in its entirety for pathologic analysis. The specimen showed an HPV-negative mass with multiple papillary fragments of verrucoid well-differentiated to moderately well-differentiated, Grade II, invasive squamous cell carcinoma (see Figure 2). A preoperative diagnosis of papillary squamous cell carcinoma of the soft palate was made. Spiral computerized tomography (CT) studies of the head and neck revealed no sign of metastatic disease. The patient underwent uncomplicated transoral excision of the mass. Post-operative pathology results confirmed the preoperative diagnosis. A palatal obturator was fashioned for reconstruction. She continued to follow-up with the clinic staff for the next four years with no sign of recurrence and excellent speech and swallow function. (A) Preoperative endoscopic image of the mass on the soft palate with (B) showing scarring at the site of the cleft palate repair (white arrow) and the mass as seen from the epipharyngeal surface of the palate (bordered by green). (C) Closer view of the scar base and a portion of the mass extending posteriorly (green arrow). (D) Nasopharynx (black asterisk) and mass (green asterisk) visible on midline nasal surface. (A) Low-power magnification of H&E section demonstrating an exophytic lesion (arrow) of the soft palate. (B) Medium-power magnification of exophytic lesion with prominent fibrovascular cores (larger arrow) and outer layer of atypical squamous epithelial cells (smaller arrow). (C) High-power magnification of papillary lesion highlighting squamous epithelial cells with significant nuclear atypia, disorganized growth (left arrow), and the presence of mitotic figures (right arrow). (D) Post-operative gross pathology specimen.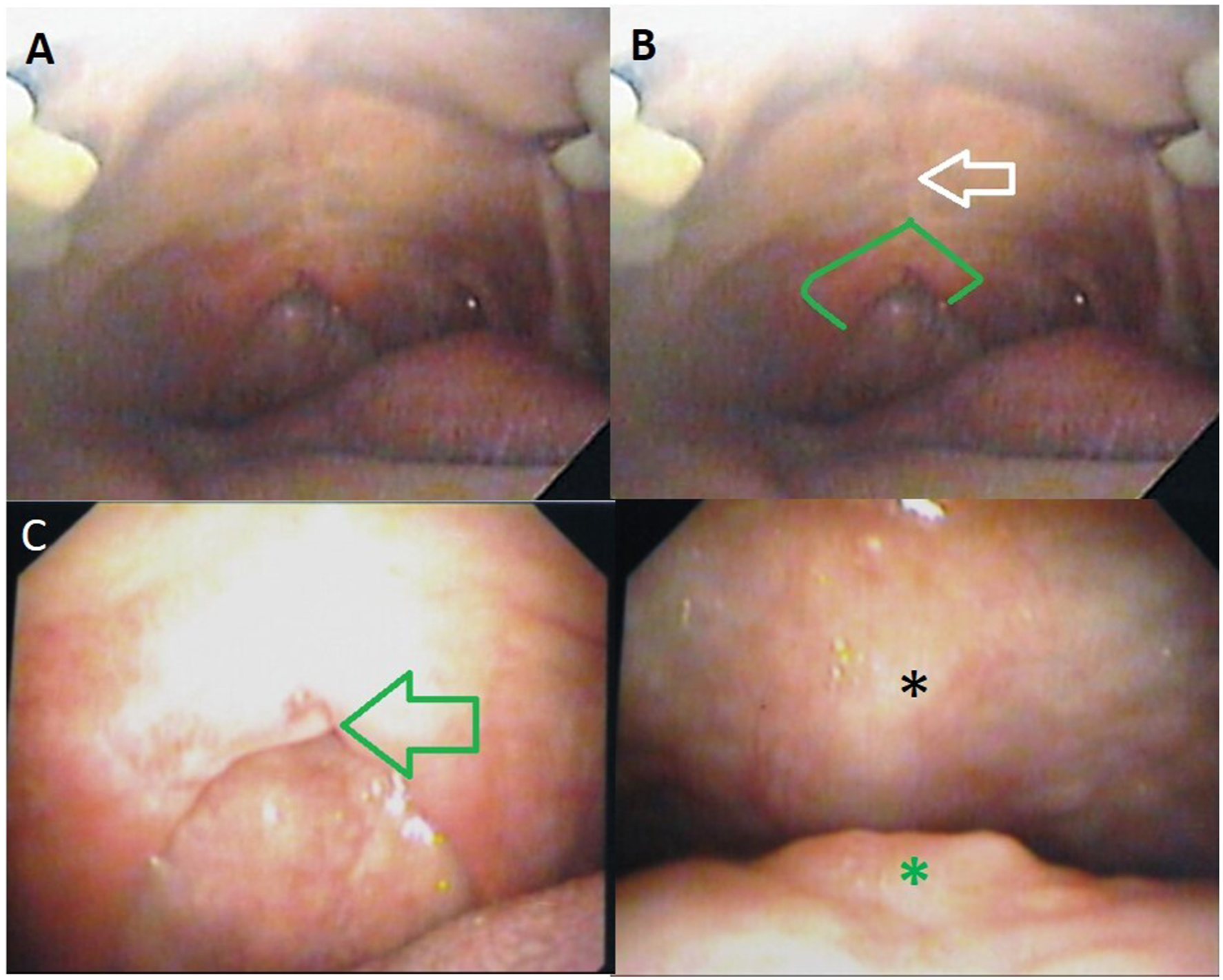
Papillary squamous cell carcinoma of the oropharynx (OPSCC) is a rare presentation of squamous cell carcinoma (SCC). The mean age of diagnosis is approximately 73 years, and it often presents as a solitary lesion with an exophytic or papillary growth. It was first described in 1968, 1 and since then there have been few reports or systematic studies describing OPSCC.2,3 This patient’s case is significant for the absence of any significant risk factors. Most notably, her OPSCC was HPV-negative, whereas HPV infection has been thought to have a strong relationship with OPSCC pathophysiology.4,5 Furthermore, the location of the malignancy within a surgical scar is significant as it proposes a unique pathogenesis related to Marjolin’s ulcers (MU).
Malignant transformation has been well documented in the setting of burn scars, trauma, non-healing wounds, vaccination scars, and sites of radiotherapy.6,7 Although not fully elucidated, it is believed that MU begins with traumatic insult to the skin that forms a chronic scar. Over time, after existence as a scar, persistent cell turnover from irritation leads to ulcer formation and eventual malignant transformation to SCC. The period between the initial insult and ulceration/malignant transformation is such that insults earlier in life often have long latency periods (50 years or more). 8 Another hypothesis is based on the recognition that the same cellular processes required for surgical wound healing (angiogenesis and cell migration) 9 are also required for cancer growth. 10
The clinical picture in this patient’s case could be explained by an MU-like pathogenesis. Her cleft palate surgery in childhood was the initial insult to the oral mucosa, and she presents approximately 50 years later with biopsy-confirmed OPSCC, mirroring the proposed latency period for MU. Additionally, the oral mucosa is consistently exposed to irritation and trauma from food and mastication which fits the proposed etiology of MU.
We present a rare case of OPSCC within a cleft palate surgical scar. This unique clinical presentation prompts further investigation into understanding the role of chronic irritation and MU-like pathogenesis in squamous cell carcinoma of the oropharynx.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.