
Abstract
Objectives
Childhood adenotonsillar hypertrophy (ATH) with sleep-disordered breathing (SDB) frequently occurs concomitant with asthma. Adenotonsillectomy and reduction in asthma severity association has been reported. We describe changes in asthma control in nonobese or normal weight and obese/overweight children undergoing adenotonsillectomy for SDB.
Methods
This prospective, nonrandomized cohort trial with 6-month follow-up at a tertiary children’s hospital enrolled 41 children with persistent asthma undergoing adenotonsillectomy for SDB. Children with significant chronic medical conditions, premature birth (< 28 weeks), or recent respiratory infection were excluded. Patients were stratified by baseline BMI into nonobese or normal weight (BMI
Results
Baseline characteristics were similar except for anthropometric measures and mean PACQLQ (P = .03). Children with nonobese or normal weight (n = 26) had statistically significant improvement in change in cACT at 3 (22.80 ± 2.33 vs. 17.86 ± 3.53, P < .001) and 6 (20.71±3.29 vs. 18.24 ± 4.16, P = .044) months compared with baseline. PACQLQ scores also improved at 3 (6.20 ± 0.87 vs. 4.56 ± 1.12, P < .001) and 6 (6.36 ± 0.72 vs. 4.93 ± 0.96, P < .001) months. Obese/overweight children (n = 10) had significant improvement in cACT scores at 6 months (20.00 ± 3.90 vs. 15.00 ± 6.90, P = .048). Change of cACT scores at 3 months (17.86 ± 3.53 vs. 14.86 ± 6.31, P = .272) was not significantly different. PACQLQ scores improved at 3 (5.47 ± 1.09 vs. 3.70 ± 0.85, P < .001) and 6 (5.75 ± 2.19 vs. 3.67 ± 1.04, P = .016) months.
Conclusion
Nonobese or normal-weight children undergoing adenotonsillectomy demonstrated significant improvement in asthma control scores at 3 and 6 and obese/overweight children at 6 months. Using the PACQLQ, caregiver quality of life improved for all children at 3 and 6 months. Surgical management of ATH in children with comorbid SBD and asthma is a good treatment option.
Introduction
Asthma is one of the most common pediatric chronic medical conditions affecting over 5 million children in the United States. 1 Poor asthma control in children results in impaired activity, missed school days, and reduced quality of life for patients and their caregivers. 2 Additionally, asthma has a massive economic burden, with tens of millions of outpatient and emergency room visits each year and estimates of over $50 billion in annual direct healthcare-related costs. 3,4 Studies also demonstrate nearly five times the yearly cost per patient in those with poorly controlled asthma compared with those with well-controlled asthma. 2
Obstructive sleep apnea (OSA) affects 1 to 3% of children in the United States, with many more children affected when more subtle forms of sleep-disordered breathing (SDB) are considered. 5 There is a growing body of evidence supporting an association between asthma and SDB. Julien et al. demonstrate children with asthma had a higher prevalence of OSA compared with controls. Additionally, children with severe asthma had a higher prevalence of OSA than those with moderate asthma. 6 Similarly, obesity is associated with reduced asthma control and markers of asthma severity. 7
The standard treatment for pediatric SDB is adenotonsillectomy, and many asthmatic children undergo adenotonsillectomy for comorbid SDB. 4 The impact of adenotonsillectomy on asthma control in these patients appears to be favorable; however, there are conflicting reports regarding asthma response that may be due to effect modifiers such as obesity. The purpose of this study was to measure the impact of adenotonsillectomy on asthma control in both nonobese or normal-weight children and obese/overweight children who have SDB, as well as to measure the effect of adenotonsillectomy on caregiver quality of life of these children.
Patients and methods
This is a prospective, nonrandomized, nonblinded cohort trial in asthmatic children undergoing adenotonsillectomy for treatment of SDB. The study was approved by the Nemours Institutional Review Board, approval number 394625. Study participants undergoing adenotonsillectomy between 2016 and 2018 were recruited. Parental consent was obtained for all participants enrolled; consent was also obtained from all patients who were between the ages of 7 and 11 years. Children of ages 2 to 11 years with a diagnosis of asthma, reactive airway disease, or airway hyper-responsiveness and concomitant SDB were included. Asthma was diagnosed and managed by the pediatric pulmonology division. Diagnosis of SDB was based on parental reports of snoring with labored or obstructed breathing during sleep plus subcostal retractions during obstructed inspiration, movement arousals, diaphoresis, neck hyperextension during sleep, excessive daytime sleepiness, hyperactivity, aggressive behavior/behavior changes, irritability, inattention, slow growth, morning headaches, or secondary enuresis, with the child’s findings not better explained by another disorder, medication, or substance abuse. Children with significant chronic medical conditions, premature birth (< 28 weeks), or patients with a recent significant respiratory infection within 30 days of surgery were excluded. Adenotonsillectomy was performed by a pediatric otolaryngologist.
Demographic and body habitus information collected included sex, age, ethnicity, body mass index (BMI), height, weight, neck circumference, waist circumference, and waist-to-height ratio. BMI calculations in children are calculated on height and weight, for age and sex. According to the BMI weight status categories on the Centers for Disease Control and Prevention’s pediatric growth charts, any youth with a BMI > 85th percentile but < 95th percentile for age and sex would be classified as being overweight and anyone with a BMI > 95th percentile would be classified as having obesity. Patients were analyzed separately based on BMI status as overweight/obese (BMI percentile > 85%) or normal weight (BMI percentile
The cACT is a seven-item questionnaire for children ages 4 to 11 years that is completed by both the child and caregiver with a 4- to 6-point Likert scale that assesses daytime and nocturnal asthma symptoms and their effect on daily functioning over the preceding 4 weeks. The first 4 items are completed by the child and the last 3 are completed by the caregiver. The score is a summation ranging from 0 (poorest control of asthma) to 27 (highest control of asthma), with a score of 19 or less corresponding to poor control. 8 A change of 2 points on the cACT has been shown to be the minimum clinically important variance. The cACT is the most validated asthma control assessment tool, and is used in large National Institutes of Health–funded asthma trials. 9
The PACQLQ is a 13-item questionnaire for children ages 7 to 17 years that is completed by caregivers with a 7-point Likert scale. Four of the questions concern activity limitations, and 9 are related to emotional function. The average score for all responses is taken to produce a score from 1 to 7, with 1 indicating severe impairment and 7 indicating no impairment. A change of 0.5 is the minimum clinically significant difference. The PACQLQ has moderate correlation with clinical asthma control and strong correlation with caregiver illness burden. 10
When comparing the outcomes at 3 and 6 months for both the cACT and the PACQLQ in both the nonobese or normal weight and obese/overweight populations, a paired t-test was used to determine significance. A P < .05 was considered significant.
Results
Demographic and Baseline Characteristics
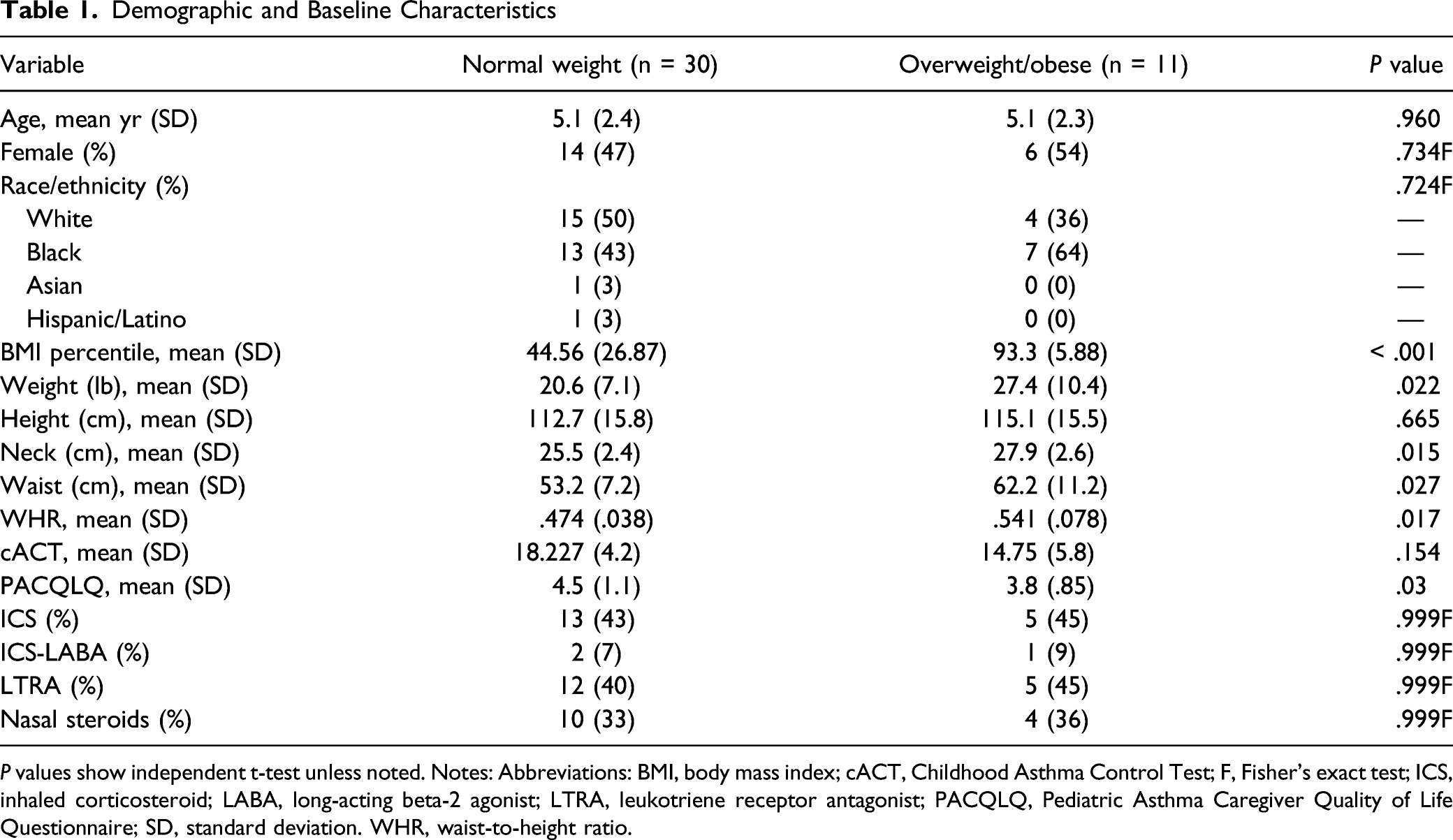
P values show independent t-test unless noted. Notes: Abbreviations: BMI, body mass index; cACT, Childhood Asthma Control Test; F, Fisher’s exact test; ICS, inhaled corticosteroid; LABA, long-acting beta-2 agonist; LTRA, leukotriene receptor antagonist; PACQLQ, Pediatric Asthma Caregiver Quality of Life Questionnaire; SD, standard deviation. WHR, waist-to-height ratio.
Changes in cACT and PACQLQ Scores at 3 and 6 Months Postoperatively
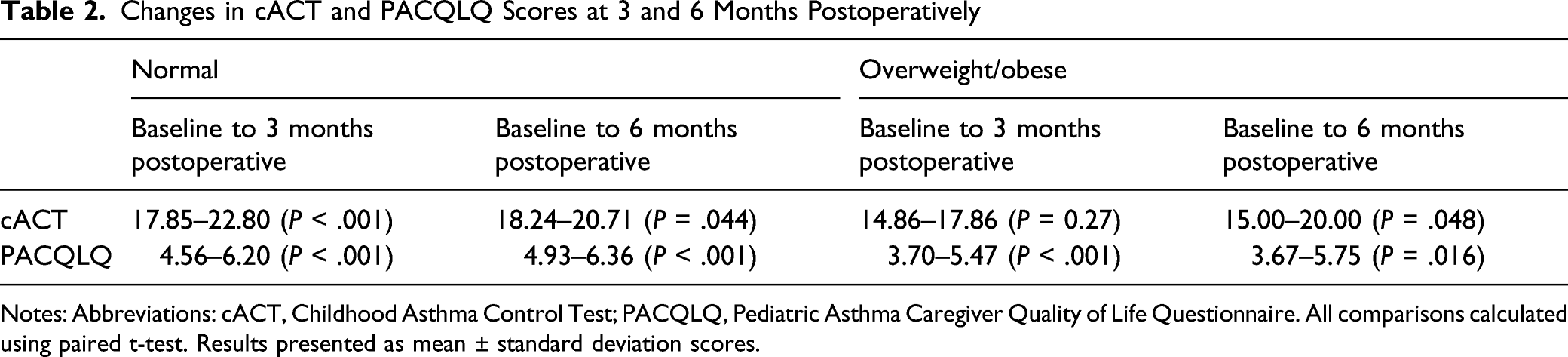
Notes: Abbreviations: cACT, Childhood Asthma Control Test; PACQLQ, Pediatric Asthma Caregiver Quality of Life Questionnaire. All comparisons calculated using paired t-test. Results presented as mean ± standard deviation scores.
Discussion
Preliminary studies as well as 2 systematic reviews examine the impact of adenotonsillectomy on children with asthma. These studies demonstrate an improvement in asthma control following adenotonsillectomy. 11 -17 A previous longitudinal database analysis of over 40,000 patients demonstrates that asthmatic children who had undergone adenotonsillectomy had a significant reduction in acute asthma exacerbation, acute status asthmaticus, asthma-related emergency room visits, and asthma-related hospitalizations. 4 Additionally, adenotonsillectomy was associated with significant reductions in most asthma prescription refills (bronchodilators, inhaled corticosteroids, leukotriene receptor antagonists, and systemic steroids). 4 Goldstein et al. examined a cohort of 80 asthmatic children who underwent adenotonsillectomy for SDB and 62 asthmatic controls. In the adenotonsillectomy cohort, cACT scores improved from 21.86 to 25.15 at 6-month follow-up, whereas in controls, cACT scores improved from 22.42 to 23.59 at 6-month follow-up; although both cohorts reached significance, the improvement was more substantial in children undergoing adenotonsillectomy. 12 Similar findings were identified by Levin et al. with a mean cACT improvement of 3 points in 60 asthmatic children who underwent adenotonsillectomy. 13
Our results are concordant with the asthma symptoms, medication usage, and cACT improvements seen in these studies. Baseline cACT measurements demonstrated that both nonobese or normal weight children and obese/overweight children had poorly controlled asthma (cACT
Despite concordance between our data and available literature examining improvement in cACT following adenotonsillectomy, other studies failed to show improvement in clinical asthma after adenotonsillectomy. An analysis of over 10,000 children with asthma in a Korean health database found no significant improvement in status asthmaticus or asthma admission with adenotonsillectomy compared with controls at 1, 2, and 3 years following surgery. 18 A second Korean national sample cohort study identified increased asthma incidence in children who had previously undergone adenotonsillectomy. 19
Torretta et al. reviewed multiple studies examining the effect of adenotonsillectomy on patient quality of life in the pediatric population. 20 The literature generally supports an improvement in quality of life following adenotonsillectomy. To our knowledge, no previous studies have evaluated the changes in quality of life of caregivers of asthmatic children following adenotonsillectomy. The PACQLQ scores increased by 1.4 and 2.1 in nonobese or normal weight children and obese/overweight children, respectively. Our results demonstrate a significant improvement in caregiver quality of life in both nonobese or normal weight children and obese/overweight children at both 3 and 6 months postoperatively. Though previously overlooked, we believe caregiver quality of life has crucial importance, and this finding bears clinical relevance when counseling caregivers and families on adenotonsillectomy in the asthmatic population.
This is the first study to examine improvements in asthma control and caregiver quality of life stratified by body habitus. This prospective cohort analysis offers new insight into the improvement in both study groups. This study is limited by a short 6-month follow-up, limiting generalizability over time for a chronic illness. Some participants were excluded from cACT analysis due to age. In our series, 2 and 6 children were lost to follow-up at 3 and 6 months, respectively. The weight percentile was skewed toward individuals with normal weight resulting in a smaller number of children with overweight/obesity. Additional multicenter trials examining the impact of habitus and ethnic disparities will further elucidate the improvement in asthma control after adenotonsillectomy.
In conclusion, children with asthma and concomitant SDB demonstrate improved asthma control and caregiver quality of life following adenotonsillectomy. Improvement in asthma measures is concordant with prior studies. In our study, adenotonsillectomy for SDB in children with asthma improved asthma control regardless of body habitus. Adenotonsillectomy was beneficial for both nonobese or normal weight children and obese/overweight children. Larger scale studies may clarify the dose effect of BMI and improvement in symptoms.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Lang receives funding from NHLBI, Regeneron Pharmaceuticals, the Thrasher Foundation, and the American Lung Association. The remaining authors declare that they have no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Previous Presentation Nemours Foundation (internal grant program).