
Abstract
Laryngeal chondrosarcomas are rare tumors that account for only 0.2% of malignant tumors of the larynx. Approximately 80% of these tumors are low grade and well differentiated and are associated with a good long-term prognosis. Herein, we report a case of a 77-year-old male presenting with acute hypoxic respiratory failure that required intubation and mechanical ventilation. Chest CT showed multiple pulmonary nodules and cavities. He then required a tracheostomy, and a soft tissue mass in the subglottic mass was discovered. A laryngoscopy-guided excisional biopsy of the mass was performed. Histopathological examination confirmed the diagnosis of laryngeal chondrosarcoma. Clinicians should consider metastatic laryngeal chondrosarcoma as a differential diagnosis for lung cavities. Overall, we believe this to be the first case of aggressive laryngeal chondrosarcoma with mediastinal and pulmonary metastasis mimicking necrotizing pneumonia.
Introduction
Laryngeal chondrosarcomas are rare tumors that account for only 0.2% of malignant tumors of the larynx. Despite the rarity of the entity, it is the third most frequently occurring laryngeal malignancy after the most common squamous cell carcinoma and then adenocarcinoma. 1 These tumors are typically localized to the posterior lamina of the cricoid cartilage (75%), 2 thyroid glands (20%), and the arytenoids (3%) 3 and rarely can occur in the epiglottis. 4 The rarity of these tumors in these locations is probably since the arytenoid is hyaline and exhibits a miniscule amount of elastic cartilage, whereas the epiglottis does not ossify throughout life. 5 Laryngeal chondrosarcomas are predominantly seen in males in their 6th to 7th decade of life. 6 Around 80% of laryngeal chondrosarcomas are low grade and well differentiated, with good long-term prognosis. 1 The pathogenesis of these entities is still unknown; however, they are hypothesized to be due to radiotherapy, medullary cervical trauma and vertebral instability, repetitive laryngeal trauma, and distorted ossification of the cartilage. 7 The presenting symptoms are variable including that patients’ may be asymptomatic, and on the other hand, they may present with dysphagia, hoarseness, stridor, and dyspnea depending on the location of the mass. Herein, we report a case of metastatic laryngeal chondrosarcoma mimicking bilateral necrotizing pneumonia.
Case presentation
A 77-year-old male with past medical history of chronic obstructive pulmonary disease, deep vein thrombosis, diabetes mellitus, hypertension, hyperlipidemia, history of incarceration 5 years ago, and an extensive smoking history presented with a 3-day history of shortness of breath and hemoptysis. The shortness of breath was associated with orthopnea and was exertional in nature. The hemoptysis occurred 2–3 times per day and was about 2 oz total a day.
On initial encounter, his temperature was 98.2 degrees Fahrenheit, blood pressure 102/49 mm Hg, heart rate 83 bpm, respiratory rate 28 breaths/min, and he was saturating at 89% on bilevel positive airway pressure (BiPAP) ventilation. Physical exam was significant for diminished breath sounds in the right lung with bilateral scattered rales and rhonchi.
Chest X-ray revealed extensive airspace disease in both lungs and infiltrates suspicious for pneumonia (Figure 1). Computed tomography scan of the chest showed large cavitary lesions with mediastinal and hilar lymphadenopathy (Figure 2, 3). Chest X-ray displayed a large confluent focus of density in each of the lungs, involving the middle and possibly lower lobes of the right lung, and the lower portion of the left lung. Large cavitary lesions at the right middle lobe and left lower lobe with additional regional areas of ground glass opacification and consolidation. Mediastinal and hilar lymphadenopathy.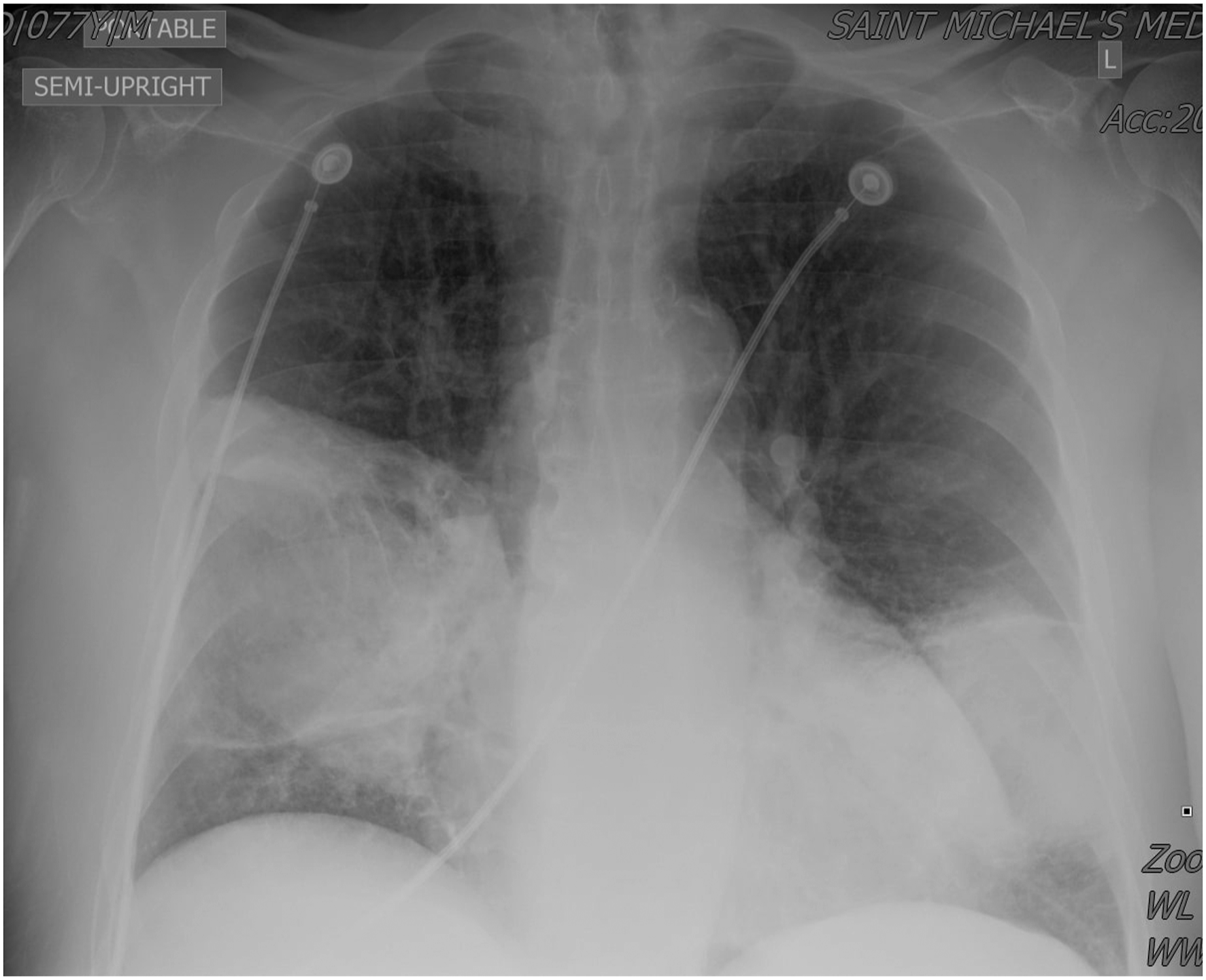

The patient was admitted to the intensive care unit for worsening respiratory distress since he continued to desaturate on BiPAP. Patient was treated with intravenous vancomycin and piperacillin-tazobactam. Blood cultures, rapid influenza tests, SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) RT-PCR (reverse transcriptase-polymerase chain reaction) Legionella Ag, Streptococcus pneumoiae Ag, and Mycoplasma pneumoniae antibody were all negative. Due to the patient’s cavitary lesions on CT chest, he was placed on airborne precautions to rule out tuberculosis. A QuantiFERON gold test was ordered; however, the result was indeterminate. Three acid-fast bacilli (AFB) smears were performed and were negative for any acid-fast bacilli. Thus, tuberculosis was ruled out. The sputum cultures were positive for Staphylococcus aureus.
A few days after admission, the patient underwent intubation and ventilatory support for hypoxemia with increasing oxygen requirements and altered mental status. Intubation was difficult since the patient had subglottic stenosis and was unable to pass a 7.5 mm tube. Thus, a 6.0 mm tube was placed. Five days after intubation, he still had increasing oxygen requirements and saturation was in the low 80s on an FiO2 of 100%; thus, a tracheostomy with laryngoscopy and biopsy was performed. There was a soft tissue mass at the subglottic space just inferior to the anterior commissure of the true vocal cord. The soft tissue mass was removed for biopsy. There was another firm mass in the right subglottic area below the posterior two thirds of the right vocal cord that was also biopsied. The epiglottis, piriform sinuses, false and true vocal cords, aryepiglottic folds, and ventricles were clear of any masses or ulcers. Histopathology report was significant for a lobulated cartilaginous tumor representing a low-grade chondrosarcoma. The hematoxylin and eosin stained sections showed mild increased cellularity and mild pleomorphism, scattered binucleated forms were present, and occasional mitotic figures were seen (Figure 4, 5). Despite the tracheostomy, the respiratory status of the patient did not improve. He subsequently died of septic shock and multi-organ failure. H & E, 400x: Mild increased cellularity and mild pleomorphism, scattered binucleated forms, and occasional mitotic figures.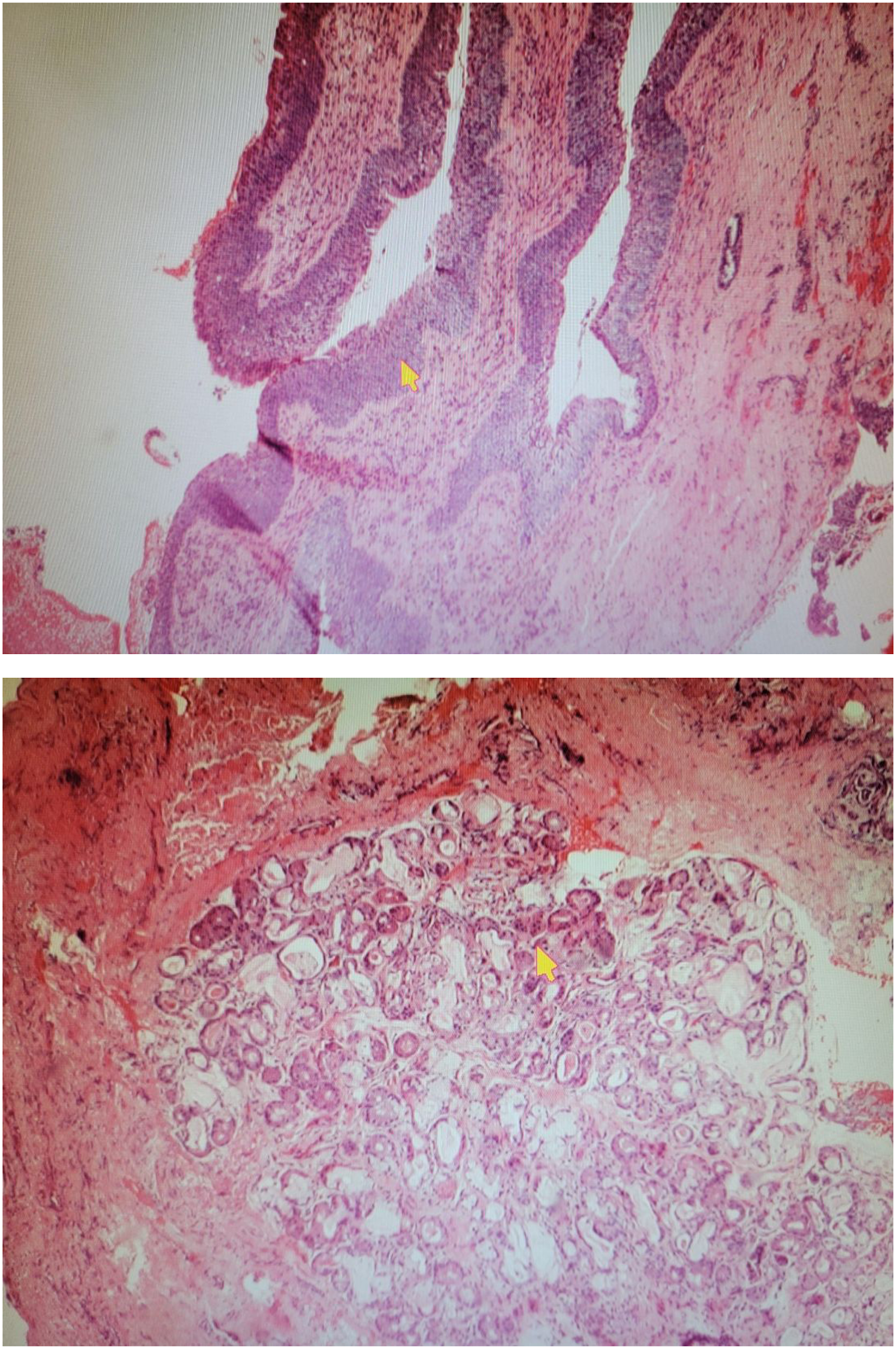
Discussion
Laryngeal chondrosarcomas account for approximately 0.5% of all primary laryngeal tumors 1 . It is the third most common tumor of the larynx after squamous cell carcinomas and laryngeal adenocarcinomas. 1 Laryngeal chondrosarcomas, which arise from disorganized ossification of the hyaline cartilage, are commonly localized to the posterior lamina of the cricoid cartilage (75%). 2 The posterior lamina is prone to increased mechanical stress which results in increased ossification of this cartilage. The high rate of ossification increases the risk of laryngeal chondrosarcoma development. 1 Less commonly, the thyroid gland (20%), the arytenoids (3%), 3 and the epiglottis are involved. 4
Laryngeal chondrosarcomas have a predilection towards males, with a male to female ratio of approximately 3:1. 1 They are seven times more likely to occur in Caucasians 8 and usually present between the sixth and the seventh decade of life. 5 Laryngeal chondrosarcomas are often low-grade tumors which are slow growing with an indolent course. If a lesion is found to have an accelerated growth, a high-grade chondrosarcoma should be suspected. 6
Patients with laryngeal chondrosarcomas can present with an array of different symptoms which vary depending on the location of the lesion. Lesions involving the cricoid cartilage typically present with dyspnea, hoarseness, and dysphagia. 1 However, thyroid cartilage involvement may present as an asymptomatic neck mass. According to a systematic review by Chin et al., hoarseness was present in 47.2% of the cases, dyspnea in 25.8%, and a palpable tumor in the neck in 9.5% of the cases. 1 Patients can also present with cough, stridor, dysphonia, and hemoptysis 1 . The duration from onset of symptoms to presentation can vary drastically, with some patients presenting as late as 18 years from the onset of their symptoms. 1
Metastasis is rare since the tumor usually causes local tissue destruction before invading adjacent tissue. In rare cases, laryngeal chondrosarcomas were found to metastasize to distant sites such as the lungs and bone. The rate of metastasis to distant sites was found to be as low as 8.5%. 7
The incidence of laryngeal chondrosarcomas is less than 1% and the etiology is still unknown. The most common risk factors include smoking 3 , prior exposure to radiation, 1 and injection of polytetrafluoroethylene. 7 These factors increase the risk of disorganized ossification which is believed to cause the growth of these chondrosarcomas. Hyaline cartilage can ossify at increasing rates with age; hence, the peak age of onset is usually in the sixth decade of life. 1 Concurrent malignancies and pre-existing laryngeal chondromas are also believed to be precursors for laryngeal chondrosarcomas. 1
Laryngeal chondrosarcomas can commonly be visualized on CT scans, presenting as well-defined hypodense lesions with “popcorn” calcifications, confined within its cartilaginous margins, or extending beyond into adjacent tissue. 7 However, MRI scans have a greater sensitivity in depicting tumor margins within adjacent soft tissues. 9 Although rare, some cases have reported dedifferentiation within a laryngeal chondrosarcoma. Unlike low-grade tumors, dedifferentiated laryngeal chondrosarcomas are associated with a poorer prognosis, higher rate of recurrence, and increased risk of distant metastases. In such cases, a hybrid of positron emission tomography/magnetic resonance imaging (PET/MRI) has shown to provide additional functional information to support the morphological mapping of these tumors. 10
Laryngeal chondrosarcomas are most commonly diagnosed by a laryngoscopy biopsy. 11 However, procedural limitations, such as difficulty in intubating patients with larger tumors 11 or presence of submucosal chondrosarcoma, 6 can make it difficult to obtain a suitable sample for biopsy.
Macroscopically, these tumors appear to be smooth, lobular, and often times translucent. Histologically, they are differentiated into different grades based on the criteria proposed by Lichtenstein and Jaffe in 1943. 12 A grade 1 tumor is similar to a chondroma with more than 2 nuclei, no mitoses, and presence of calcifications. A grade 2 lesion presents with low nuclear to cytoplasmic ratio and minimal mitoses. A grade 3 lesion has further cellular atypia with high number of mitoses, increased nuclear to cytoplasmic ratio, and presence of multinucleated cells. 12 Grade 1 chondrosarcomas account for approximately 64% of the cases. 13 Many low-grade laryngeal chondrosarcomas are erroneously diagnosed as a chondroma. 14
In cases where an orotracheal approach for tumor biopsy is limited or contraindicated, an ultrasound-guided biopsy can be considered. In a prospective study involving 66 participants, the specificity and the positive-predictive value of the procedure were both 100%. 11 This makes it a suitable option in cases where orotracheal intubation is difficult to achieve. This approach also helps avoid exposure to general anesthesia, making it a minimally invasive, cost-effective modality. However, the use of ultrasound-guided biopsy is limited in patients who have had radiotherapy in the past. This is attributed to the fact that recurrence after radiotherapy may be submucosal and at multicentric foci, making it difficult to detect the lesion on imaging studies. 11
Laser endoscopic surgery with macroscopic resection of the lesion can also be used to gain a histological diagnosis before drastic steps are taken with radical treatments. However, tumor-free surgical margins 2 are difficult to achieve with this method and recurrence of tumors can be as high as 50%.4,11
Since most laryngeal chondrosarcomas are either low or intermediate grade, 2 conservative surgery is recommended for most of these tumors. The most important factor for conservative surgery is the site of tumor origin.4,15 Depending on the location, surgical resection of chondrosarcomas of the thyroid, arytenoids, and epiglottis can be easily performed. On the other hand, cricoid chondrosarcomas are challenging to resect. 15 This is amenable to the fact that resection of a part of cricoid lamina can cause laryngeal stenosis and collapse of the glottis.4,15 Therefore, guidelines suggest preserving at least one cricoarytenoid unit for functional and anatomic support, the corresponding recurrent laryngeal nerve, and structural support for airway at the level of the crico-tracheal junction. 2 For this reason, total laryngectomy is the procedure most practiced for laryngeal chondrosarcomas that are large and involve the cricoid cartilage. 15
Radical treatments are considered in patients with high grade 1 or large tumors, in whom conservative surgery could potentially cause destabilization of the cricoid ring. 16 In 1973, Jones reported the indications for total laryngectomy as follows: large tumors and inability to maintain a patent airway, tumor recurrence, and anaplastic features on histology. 17 Total laryngectomy has been found to be performed in cases where the tumor has invaded more than 50% into the cartilage.9,17 The rate of survival was 86% in patients where it was used as primary treatment, and 77% in cases of recurrence. 14
The use of radiotherapy is controversial due to the tumor’s low radiosensitivity. It is, therefore, reserved for inoperable cases or used as a palliative treatment in patients who present with single tumors less than 14 mm in diameter. 18 Radiofrequency ablation used in combination with chemotherapy or radiotherapy may be another palliative measure. 18
In patients with laryngeal chondrosarcomas with no definitive treatment, management is aimed at preserving a patent airway via emergency tracheostomy, laser debulking, or emergency laryngectomy. 19 Emergency tracheostomy can be used to relieve airway obstruction and improve nutritional status in patients with large laryngeal masses, while providing an access for biopsy. However, it can increase the risk for peristomal recurrence of tumor with an incidence of 5%–15% after a total laryngectomy.19,20 Management of airway obstruction can also be achieved with laser debulking, especially in cases where the tumor is obstructing the glottic and supraglottic regions. Although risk of infections and peristomal recurrence is lower with this technique, compared to emergency tracheostomy, the risk of postoperative bleeding, laryngeal edema, and aspiration pneumonia is increased. 19 Emergency laryngectomy may be performed in the first 24 hours of hospital admission in a patient with no prior treatments and undiagnosed malignancy. It is recommended in patients where the tumor is causing glottic obstruction and has invaded the trachea. The risk of infection and peristomal invasion of tumor cells is minimal with this technique. 19
Conclusion
While most patients with localized laryngeal chondrosarcoma may be cured with excellent prognosis, metastasis occurs in only 8.5% of cases, with the lungs being the most frequent location. 21 Diagnosis of these tumors is typically made by laryngoscopy with biopsy. 11 The mainstay of treatment for these lesions if localized includes surgical excision, with excellent prognosis. 21 Overall, we believe this to be the first case of aggressive laryngeal chondrosarcoma with mediastinal and pulmonary metastasis disguised as necrotizing pneumonia. There is no standard of management for this high-grade chondrosarcoma of the larynx. There is a need for treatment guidelines for patients with metastatic disease.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.