
Abstract
Background
Recently, endoscopic endonasal approaches (EEA) have been used for skull base defect reconstruction surgeries. The nasoseptal flap (NSF), a vascular pedicled flap, was introduced to decrease postoperative cerebrospinal fluid (CSF) leakage.
Purposes
This study aimed to outline the authors’ institutional experience using NSF and rigid implants in anterior skull base defect reconstruction surgeries following EEA.
Design
A retrospective cohort review of patients who underwent NSF reconstruction following EEA in the Otorhinolaryngology and Neurosurgery Departments at King Saud University Medical City, Riyadh, Saudi Arabia, from January 2015 to May 2021, divided into 2 time periods according to the reconstruction technique.
Result
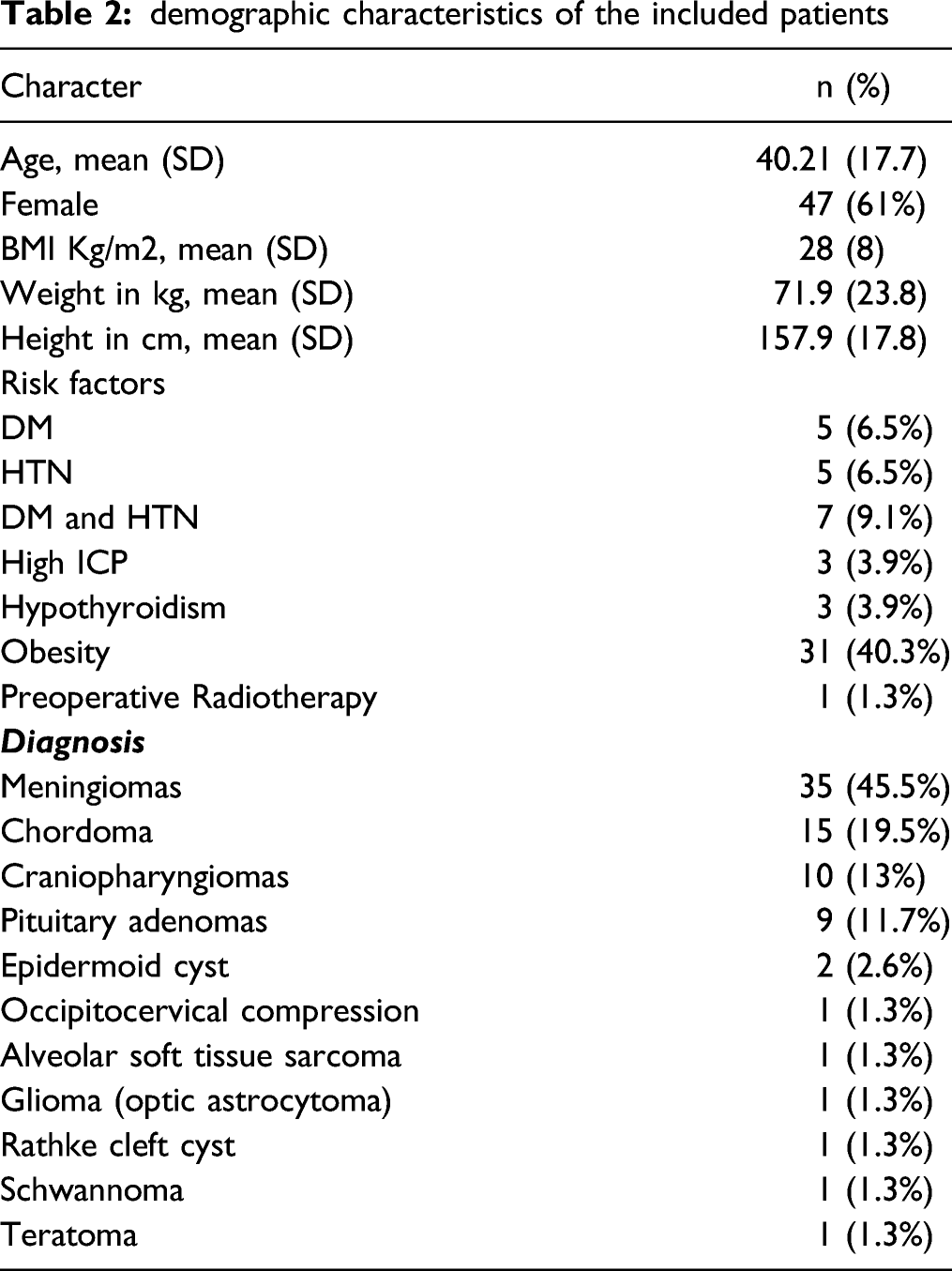
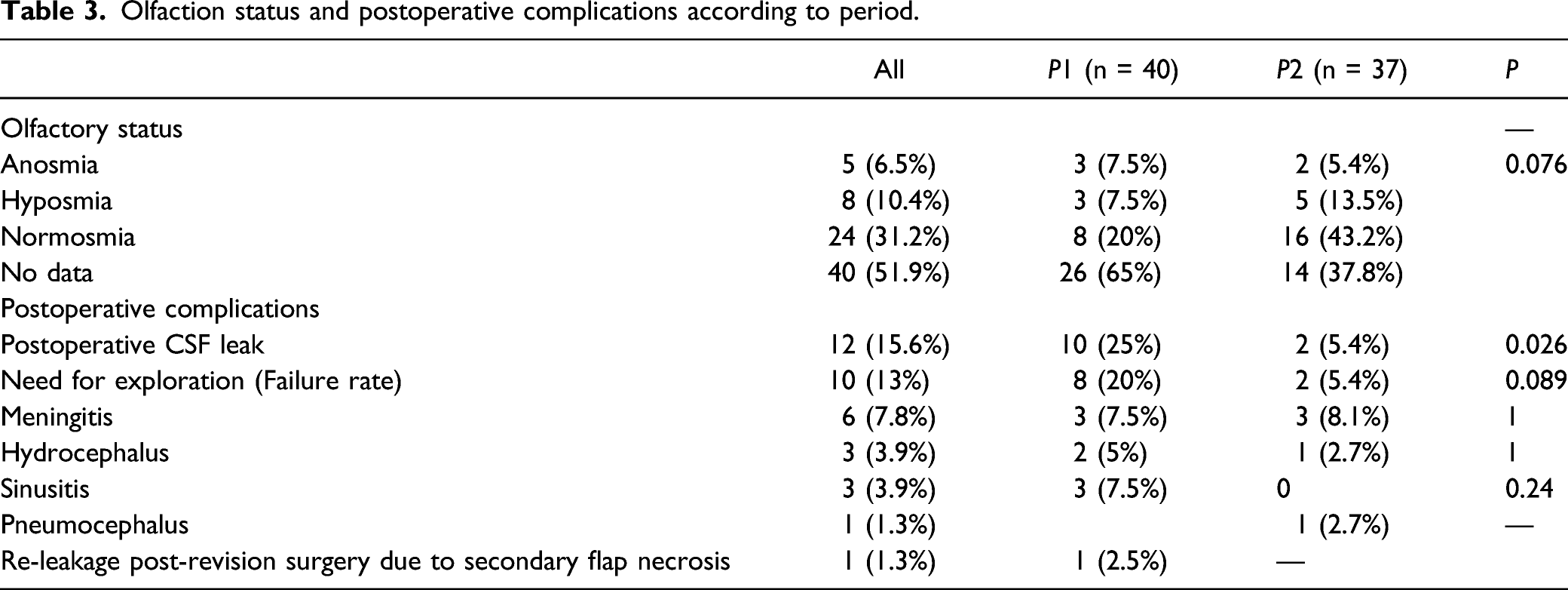
Out of the 106 patients who underwent EEA, 77 underwent NSF reconstruction. The majority had expanded EEA (94.8%). The mean age was 40.21 ± 17.7 years, and the female gender represented 61% of the sample. More than half of the sample underwent right NSF (57.1%). Meningioma was the most common diagnosis (45.5%). The clivus was the most frequent site of lesions (23.4%). The overall rate of postoperative CSF leakage and lumbar drainage (LD) insertion was 15.6% and 51.9%, respectively. The duration of LD was a median of four days. The overall failure rate was 13%, declining from 20% in the first period to 5.4% in the second period. Rigid implants were used significantly more in the first period than in the second period (67.5% versus 16.2%, P < 0.001). Meningitis, the highest postoperative complication, was reported in 6 patients (7.8%). One patient died three weeks postoperatively after massive nasal bleeding. No significant difference was found between either side of the NFS regarding the CSF leakage and failure rate.
Conclusion
In the authors’ experience, there has been an overt decline in failure rates and complications of EEA over the last three years due to increased experience among surgeons and a standardization of reconstruction techniques. Minimal reconstruction may provide satisfactory results by decreasing the use of rigid implants. An endoscopic endonasal approach with an NSF for anterior skull base defect reconstruction is considered a safe procedure with no significant difference between the sides of the flap.
Introduction
EEA have been widely used for skull base surgeries that allow minimal intervention. Endoscopic skull base surgeries are required for many cranial lesions, benign and malignant neoplasms (extradural and intradural). These approaches were limited to the pituitary fossa, as in standard EEA, but with improvements in anatomical understanding and biotechnology, EEA were expanded to regions beyond the pituitary fossa (expanded EEA), 1 such as transplanum/transtuberculum and transcribriform. Postoperative CSF leakage is one of the most serious complications after endoscopic skull base reconstruction surgery; it may lead to meningitis, pneumocephalus, and the need for revision surgery. 2 Due to the inevitable disruption of the barrier between the subarachnoid space and the sinonasal cavity in some types of surgeries, CSF leakage could develop. 3 Therefore, recent advanced instruments, reconstruction techniques, and image-based navigation systems have been developed to reduce postoperative complications and overcome flap failures.
In 2006, Hadad et al. were the first to describe the development of the NSF, a vascular pedicled flap from the mucoperichondrium and mucoperiosteum of the nasal septum known as the Hadad-Bassagasteguy flap (HBF), which is used for anterior, middle, clival, and parasellar skull base defects. 4 The technique involves NSF, fibrin glue, and nasal packing with or without collagen inlay graft and fat graft. 4
Several studies that have used endoscopic endonasal NSF have reported a remarkable decline in postoperative CSF leakage, 5 even with some modifications to the technique, such as using dual-layer fascia lata grafts, 6 gasket seal closures, 7 and the 3F technique (fat graft, NSF, and flash mobilization) 8 .
Furthermore, it was also found that high-flow intraoperative CSF leaks and large defect sizes are associated with an increased risk of reconstruction failure; thus, pedicled vascularized flaps (NSF) have been recommended to achieve higher success rates.9-11
However, there is a lack of available clinical data to optimize the reconstruction for each skull base defect, site, and pathology. Therefore, this study aimed to analyze authors’ institutional experience in the endoscopic reconstruction of skull base defects as a result of an endoscopic endonasal approach to NSF to identify the prevalence of CSF leakage, other postoperative complications, and potential risk factors that may contribute to unfavorable complications or outcomes.
Methods
Study design
This retrospective review of patients who underwent EEA with NSF reconstruction performed in the Otorhinolaryngology and Neurosurgery Departments at King Saud University Medical City, Riyadh, Saudi Arabia between January 2015 and May 2021 was divided into 2 time periods according to the reconstruction technique: the first period (P1) was from January 2015 to December 2018, and the second period (P2) was from January 2019 to May 2021. All the medical records for the patients who underwent EEA were reviewed. We included all patients on whom NSF was performed, with no restrictions for gender, age, and residency. Patients who underwent combined external and endoscopic approaches or transcranial surgery were excluded. Patients with defects other than anterior skull base defects, such as middle and posterior cranial fossa defects, were also excluded. The study design was approved by the Review Board of Ethics at King Saud University Medical City (16/0164/IRB).
Data collection
The patient’s medical records were reviewed to extract and collect the following: patients’ demographic information (age, gender, height, weight, body mass index, comorbidities, and previous history of radiotherapy), indication for surgery, the site of the lesion, the side of the flap, the type of rigid implants if used, the insertion of a lumbar drain, postoperative complications, and the length of hospital stay. Preoperative radiological scans (CT and MRI) and clinical examinations were also reviewed.
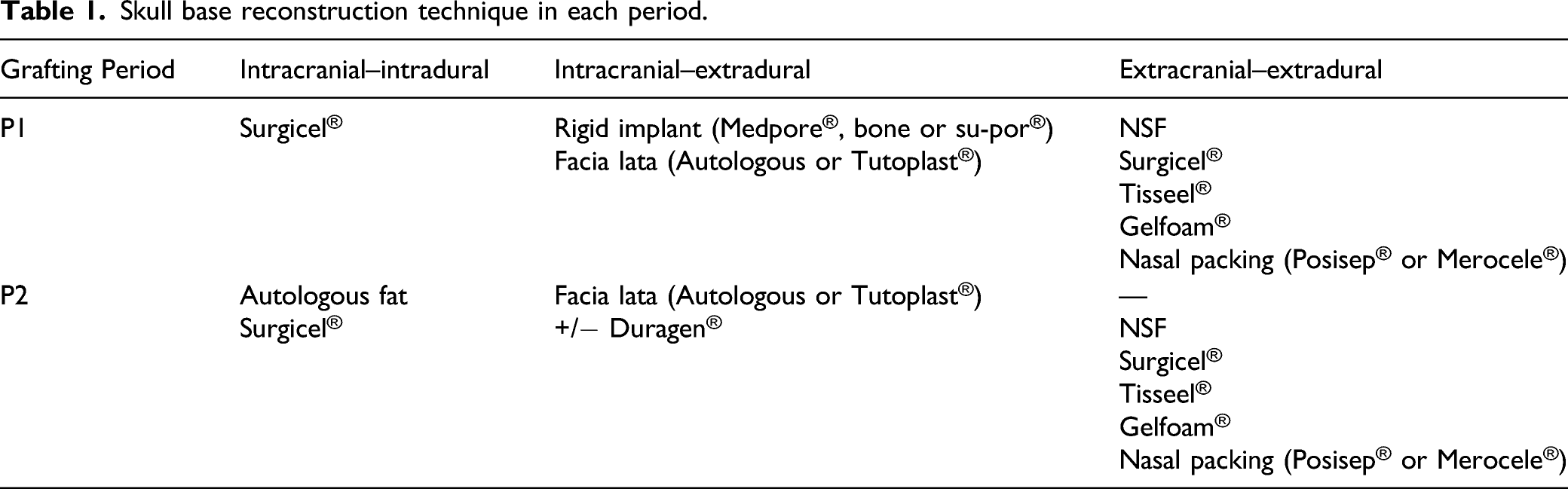
Surgical procedure
Skull base reconstruction technique in each period.
Statistical analysis
Data analyses were performed using SPSS Version 19 software. Categorical variables were reported in a descriptive evaluation by frequencies (percentage) and mean (standard deviation). A chi-squared test or a Fisher’s exact test was used when appropriate with a 5% significance level to test the difference in each category.
Results
demographic characteristics of the included patients
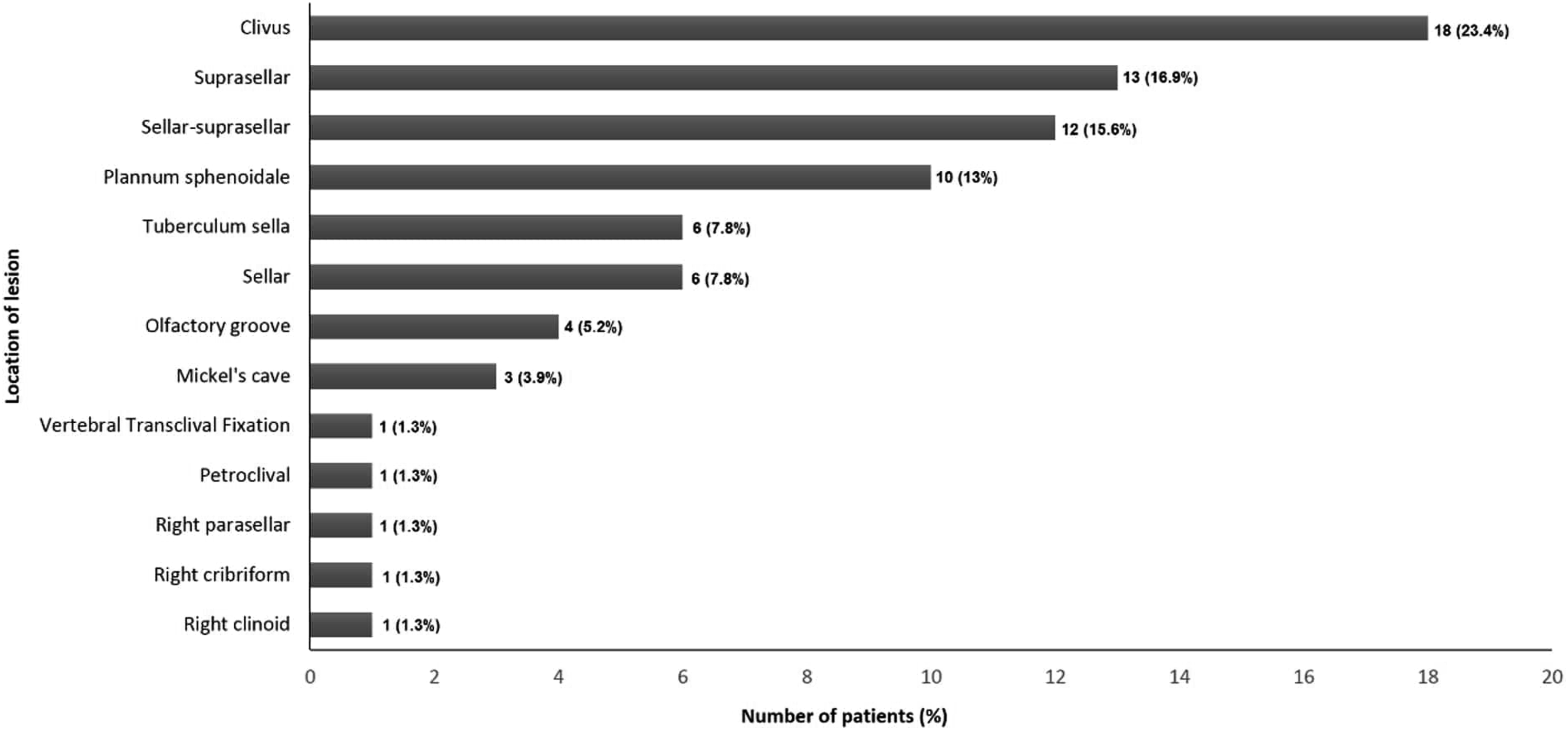
Locations of the lesions.
Olfaction status and postoperative complications according to period.
Discussion
The efficacy of endoscopic endonasal NSF reconstruction for skull base defects that occurred post–skull base surgery was studied in 77 patients. The rate of postoperative CSF leakage was 15.6%. Revision surgery was needed in 10 cases (13%). A decline in both postoperative CSF leaks and the need for revision was observed over seven years of clinical experience. The rate of postoperative CSF leakage in this study is in a comparable range to the rate of 8.5% CSF leakage arrived at by a systematic review of 22 studies, including 673 patients.
2
In the second period of the study, CSF leakage and a failure rate of 5.4% were noted. This rate may be explained by the severe clinical heterogeneity that the patients had on several sites of lesions, such as the clivus, sellar, sellar–suprasellar, and suprasella, alongside a wide range of diseases, including different types of tumors. Another systematic review of 193 studies showed that the incidence of CSF leakage was 3.7% with the transsphenoidal approach and it was 9% with the expanded EEA.
12
Although J. K. Liu et al.
13
concluded in their case series of 207 patients with skull base tumors that the use of Medpore® offers a safe option for reconstruction after skull base surgery, the majority of failures (20%) were in P1, when the rigid implant was used in 27 out of 40 patients (67.5%). In January 2019, the failure rate was reviewed by our multidisciplinary team (Rhinology and Neurosurgery) and the decision was made to decrease the use of rigid implants. It is noteworthy that a constant failure rate of only one case per year was observed over the last three years (P2), which dropped to zero in 2021 (Figure 2), but the exact cause of this improvement in outcome could not be determined and it may be due to increasing surgeon experience, standardization of repair technique, and/or reduced use of rigid implants (16.2%). Decline of CSF leaks and the need for revision over time.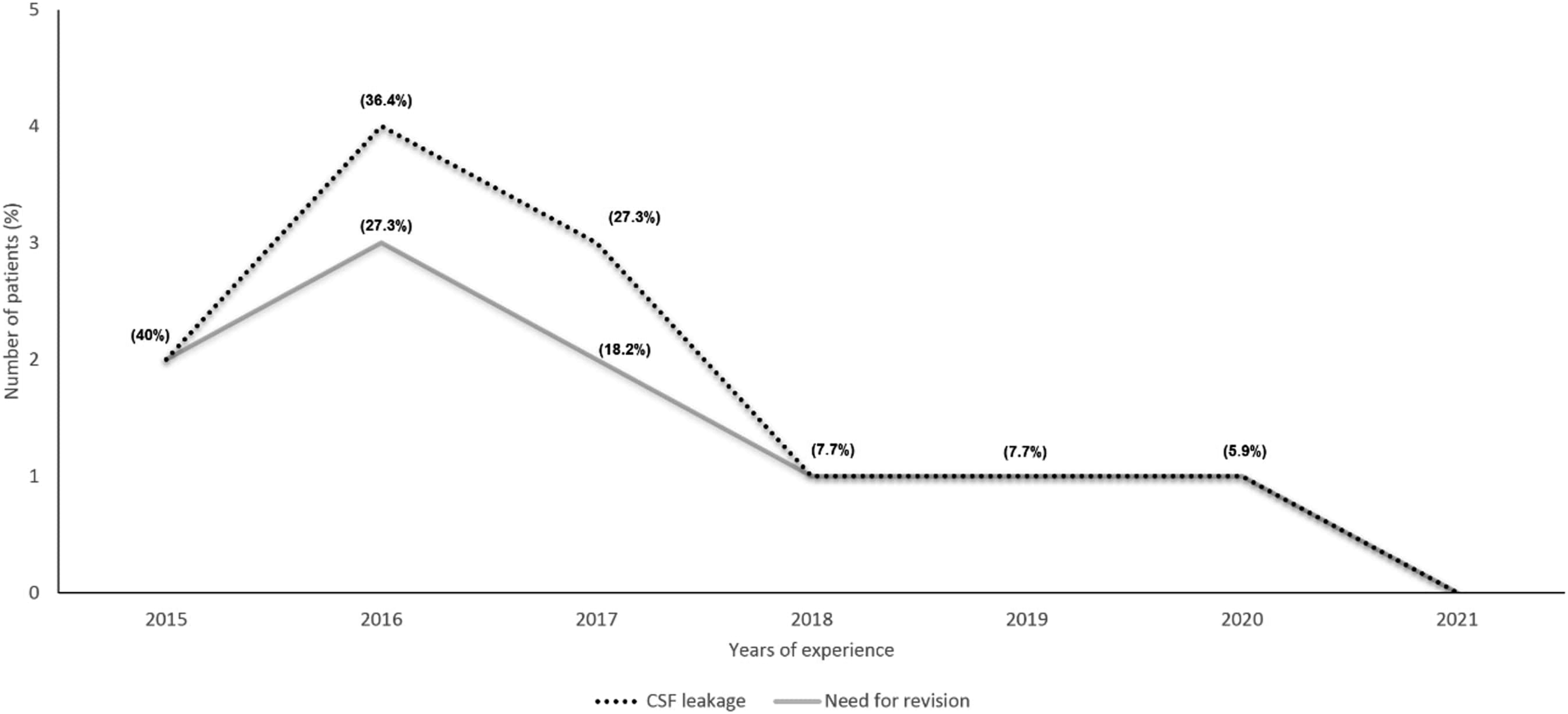
Multilayer skull base reconstruction procedures can be accomplished using a variety of synthetic and/or autologous materials, including: synthetic or allograft dural replacement grafts, absorbable sealants and glues, autologous and synthetic rigid materials, free autograft, and vascularized flaps. Availability, biocompatibility, rapid healing, and low cost are advantages of autografts (tissue, mucosa, or rigid) and vascularized flaps. However, morbidity of donor site and increased operative time must be considered when choosing autologous reconstruction options. 14 The synthetic dural replacement grafts, in addition to their role in the multilayer reconstruction, can promote the healing process through angiogenesis, formation of new collagen and fibroblast ingrowth. S.C. Seaman, et al. 15 described the potential reduction in encephalocele formation and the ability to tailor the graft shape to fit the defects as advantages of rigid material in endoscopic reconstruction and recommended using the rigid material for patients at higher potential risk of postoperative CSF leak.
For a favorable reconstruction, it is first recommended to achieve a stable separation between the nasal cavity and the cranial cavity to prevent a disruption of the barrier between both cavities, which leads to CSF leakage. 3 Second, it is advised to preserve the important neurovascular structures in the field and their functions. Third and lastly, it is suggested to avoid dead spaces and place any material or mucosa between the flap and the skull base bone. In the revision surgeries, Surgicel® was administered over the edges, with or without Tutoplast®, and then Gelfoam® and Tisseel Lyo®.
The reapplication of the NSF was performed in 4 cases. One of the patients experienced a secondary leakage after the revision repair of the CSF leak due to meningitis and sinusitis. The defect was repaired by fat and facia lata from the right thigh with Tisseel® and Gelfoam® and merocele® nasal packing. Before the NSF, skull base defects were reconstructed by multilayer fat grafts or synthetic material, such as inlay and onlay grafts secured with fibrin glue, which resulted in higher rates of CSF leakage and reconstruction failure. 16 However, with the endoscopic endonasal NSF technique, a decline in postoperative CSF leakage and reconstruction failures were demonstrated in several studies and reported in the literature.2,4,5,8,10-12,16 The anatomical site of the skull defect and the flow rate of intraoperative CSF leakage can affect the surgical technique of using free grafts or vascularized flaps. Thus, pedicled vascularized flaps were recommended for cases with high-flow intraoperative CSF leakage, while equal results were noted in cases of low-flow intraoperative CSF leaks when reconstruction was achieved by multilayered free grafts and synthetic materials rather than by vascularized flaps. 2 According to a retrospective cohort of 121 patients, the central skull base defect, for instance, in the sella and clivus, was found to be associated with reconstruction failure. 17 For large defects, such as in the parasellar skull base, the endoscopic endonasal transplanum transtuberculum approach with a pedicled nasoseptal flap showed a decline in postoperative CSF leakage. 9 In addition to intraoperative CSF leakage, a non-ideal BMI was positively associated with an increased risk of postoperative CSF leakage in both expanded and non-expanded endoscopic endonasal surgeries.18,19 A total of 71% of this current study’s sample were above 25 (overweight fc), and 40.3% were above 30 (obesity); however, only 50% of failure cases had a BMI of above 25.
One female patient received preoperative radiotherapy, although she did not experience a CSF leak or any other complications except a need for lumber drainage. However, this patient had DM, hypothyroidism, and pan-hypopituitarism as comorbidities. This is consistent with a review of 152 patients in which 37 cases received radiotherapy. Compared with patients who did not receive radiotherapy, no significant association was found regarding complications except the increased risk for prolonged skull base crusting. 11
In addition to revision surgery, ventriculoperitoneal shunts, and EVD, lumber drainage is a supportive measurement performed following endoscopic endonasal skull base reconstruction. A ventriculoperitoneal shunt was needed in one case that was complicated by hydrocephalus, and EVD was inserted in 7 patients (9.1%). Lumbar drainage was used in 51.9% of patients for a median of four days, with no significant difference in the rate of failure with and without LD insertion. However, there is still controversy regarding the advantages or indications of lumbar drainage because its complications are unpredictable and may exceed the complications arising from CSF leakage. 20 For instance, Caggiano et al. found that lumber drainage is associated with prolonged immobilization and hospital stay and offers no advantage for tumor gross total removal. 21
Olfactory dysfunction is another complication that may be associated with NSF reconstruction. In the current study’s results concerning olfactory function, 13 patients (16.9%) developed olfactory dysfunction, either hyposmia or anosmia. However, these results may be inconclusive since there was no test data for half of the included patients. In a randomized controlled trial on performing endoscopic pituitary surgery with or without a septal flap, olfaction would be affected, and using the NSF could worsen the condition for at least six months postoperative. 22 It was also found that preoperative nasal disease and smoking increase the risk of developing olfactory dysfunction after endoscopic endonasal transsphenoidal approach surgeries. 23
This study has some limitations in that endoscopic NSF reconstruction was performed for the management of a range of diseases with the presence of comorbidities for which the correlation of these factors with the outcome has not been evaluated. Our study was performed in a retrospective manner; thus, we could not observe the different impacts of using the NSF and rigid implants on the failure rate. Further cohort studies with control groups or randomized controlled trials with clear inclusion criteria and without selection bias are necessary to outline the role of such variables in endoscopic NSF reconstruction for skull base defects.
Conclusion
An overt decline in failure rates and complications of EEA has occurred over the last three years due to increasing experience among surgeons and the standardization of repair techniques. Minimal reconstruction may give satisfactory results by decreasing the use of rigid implants. Endoscopic endonasal reconstruction with the NSF for anterior skull base defects is considered a safe procedure with no significant differences between the sides of the flap.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s note
Ahmad Alroqi is a co-first author who contributed equally to the first author.