
Abstract
Congenital anterior skull base defects with meningoencephaloceles causing nasal obstruction and cerebrospinal fluid (CSF) rhinorrhea are rare clinical entities. Traditionally, skull base defects have been repaired via a bifrontal craniotomy. With the introduction of pediatric endoscopic instrumentation, more of these lesions are accessible via an intranasal endoscopic approach, even in the infant population. However, due to the rarity of pediatric meningoencephaloceles, there is a lack of data demonstrating the successful adaptation of endoscopic skull base techniques to the pediatric population. In this report, we present a case of a pediatric frontonasal meningoencephalocele with an anterior skull base defect in a 3-year-old child that was successfully addressed transnasally following 4 failed transcranial approaches. The case highlights the importance of a thorough preoperative evaluation of the surgical approach as well as interdisciplinary management of these patients at a young age. Congenital anterior skull base defects with meningoencephaloceles and CSF leaks are rare clinical entities. Hence, an interdisciplinary approach is vital including experienced pediatricians, otolaryngologists, and neurosurgeons to evaluate the ideal surgical method on an individual basis. The transnasal endoscopic technique has been shown to be minimally invasive, efficient, and safe to apply even to the infant population which could positively be demonstrated in this case.
Keywords
Introduction
A meningocele refers to herniation of the leptomeninges while an encephalocele includes the herniation of brain tissue. A meningoencephalocele is the extracranial herniation of brain tissue with meninges through a defect in the skull with an incidence of 1 of 4000 to 5000 live births. 1 Frontobasal encephaloceles present as either endoscopically visible or as hidden masses within the upper nasal passageways and may even cause external nasal deformity and hypertelorism. Congenital lesions arise due to defective development of the anterior neuropore in the region of the foramen cecum. Traumatic meningoencephalocele usually occurs following head injury or extended skull base surgeries. 2 Sincipital meningoencephalocele may be subclassified into nasofrontal, nasoethmoidal, or naso-orbital types. The nasoethmoidal type is the most common frontobasal encephalocele; 2 it includes the sphenoethmoidal, transsphenoidal, and sphenoorbital subtypes. Pediatric meningoencephaloceles have been traditionally addressed with transcranial approaches, which is a rather risky procedure in this population. However, untreated children may present with recurrent meningitis and/or epilepsy that cannot be controlled with medications. In the past, many neurosurgical routes have been described to treat these lesions. For many years, the bicoronal approach with frontal craniotomy and pericranial flap has been considered the preferred option; though successful, this procedure is not without risks and requires prolonged hospitalization. 1 Following the first report by Wigand in 1981, the transnasal endoscopic approach has evolved tremendously for the repair of cerebrospinal fluid (CSF) rhinorrhea. Advances in surgical instruments and expertise have also led to effective management of meningoencephaloceles via a single-stage, exclusively endoscopic approach in select cases. 2 The nasoseptal flap is a vascular pedicle flap that is supplied by the posterior nasoseptal artery, a branch of the sphenopalatine artery. 3 It has become the workhorse for the reconstruction of the anterior skull base (ASB) defects, resulting in a significantly decreased incidence of postoperative CSF leaks. 4
Case Report
We present the case of a 3-year-old boy with a CSF leak, causing recurrent left sided rhinorrhea since birth. He is a twin who was born prematurely at 24 weeks with a birth weight of 680 g. Due to the rhinorrhea, he underwent a neuroradiological evaluation with magnetic resonance imaging and a computed tomography scan of the cranium and mid-face. Imaging confirmed the fronto-basal skull defect with the detection of a mild prolapse of brain tissue (Figure 1). The simultaneous detection of an increased level of β-trace-protein of the nasal fluid led to the first transcranial surgery approach performed by a pediatric neurosurgical department in Germany in June 2016. Due to recurrent rhinorrhea and the detection of a postoperative subdural hygroma on the left side, the same neurosurgical department performed a transcranial revision and reconstruction of the skull base in October 2017. The surgery was unsuccessful and was directly followed by a second revision via a transcranial approach with an addition of a galeal muscle patch in November 2017. Following the third transcranial operation, the child experienced a single event of a generalized seizure. In January 2018, he presented with relapsing rhinorrhea and a fourth transcranial revision was performed—this time using fascia lata for the reconstruction. Simultaneous, a ventriculoperitoneal (VP) shunt was placed. Unfortunately, the skull base defect persisted after the abovementioned therapy. However, no sign of meningitis was present at any time. In May 2018, the family presented to the Ear, Nose, and Throat department of Tuebingen University Hospital. After an interdisciplinary preoperative discussion with the department of neurosurgery, a navigation system–guided transnasal endoscopic approach was conducted under general anesthesia to remove the residual intranasal meningoencephalocele and seal the defect (Figure 2). An off-label, preoperative intrathecal injection of fluorescein was performed and at no time during the operation was CSF detectable (Figure 3A). After thorough decongestion of the nose, a diagnostic nasal endoscopy was performed. The residual meningoencephalocele was identified and removed with cold steel instruments. The surrounding mucosa of the skull base defect was then denuded and covered with a layer of Tachosil as an onlay graft in combination with a pedicled nasoseptal flap from the left side as an overlay graft (Figure 3B-D). The harvesting of the flap was done via a posterior septal incision starting below the sphenopalatine pedicle to the floor of the nasal fossa and then followed by an anterior incision between the sphenoid ostium and the roof of the nasal fossa. The anterior approach was handled delicately as not to injure the sphenopalatine artery and the pedicle of the flap. The whole flap was then elevated from anterior to posterior, remaining attached to the sphenopalatine pedicle. After the correct placement of the flap, it was reinforced with fibrin glue and gel foam (Figure 3B), and the reconstruction was held in place by a temporarily placed nasal tamponade. After surgery, a third generation weight adapted cephalosporin was used as antibiotic prophylaxis for 5 days. The child recovered quickly without any further detection of rhinorrhea during follow-up of 2 years to this day (Figure 4). In July 2018, the VP shunt- and osteosynthesis material of the neurosurgical procedures were removed.
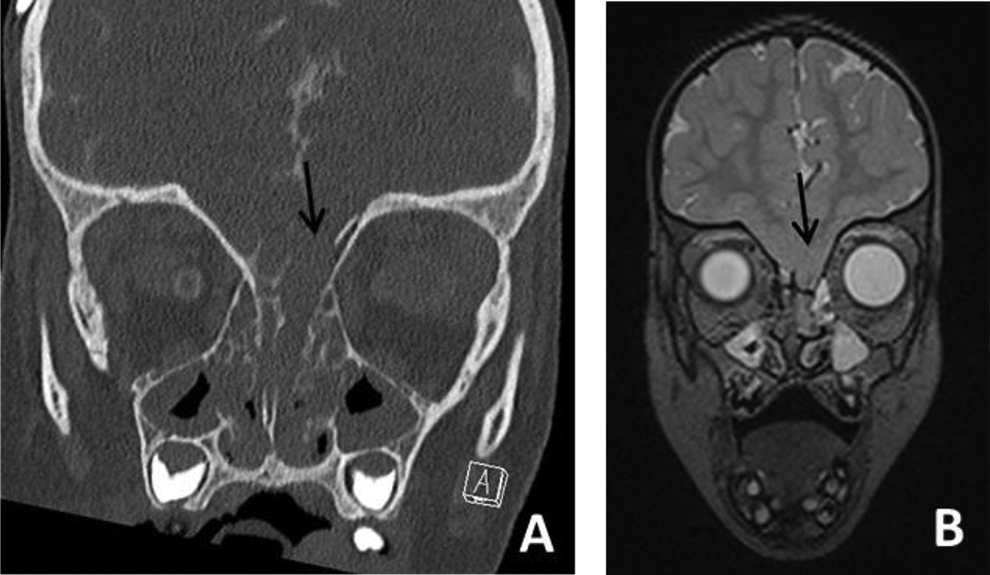
A, Coronal computed tomography scan showing the anterior skull base defect of the left side (B) coronal T2 MRI scan showing the prolapse of brain tissue. MRI indicates magnetic resonance imaging.
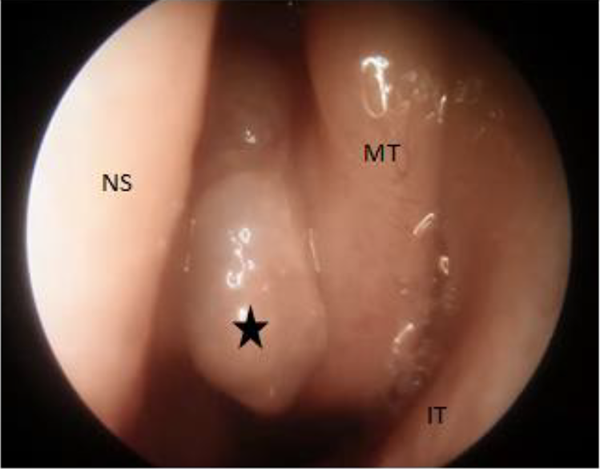
Endoscopic view of the left nasal cavity. NS indicates nasal septum; MT, middle turbinate; IT, inferior turbinate, black star: the meningoencephalocele.
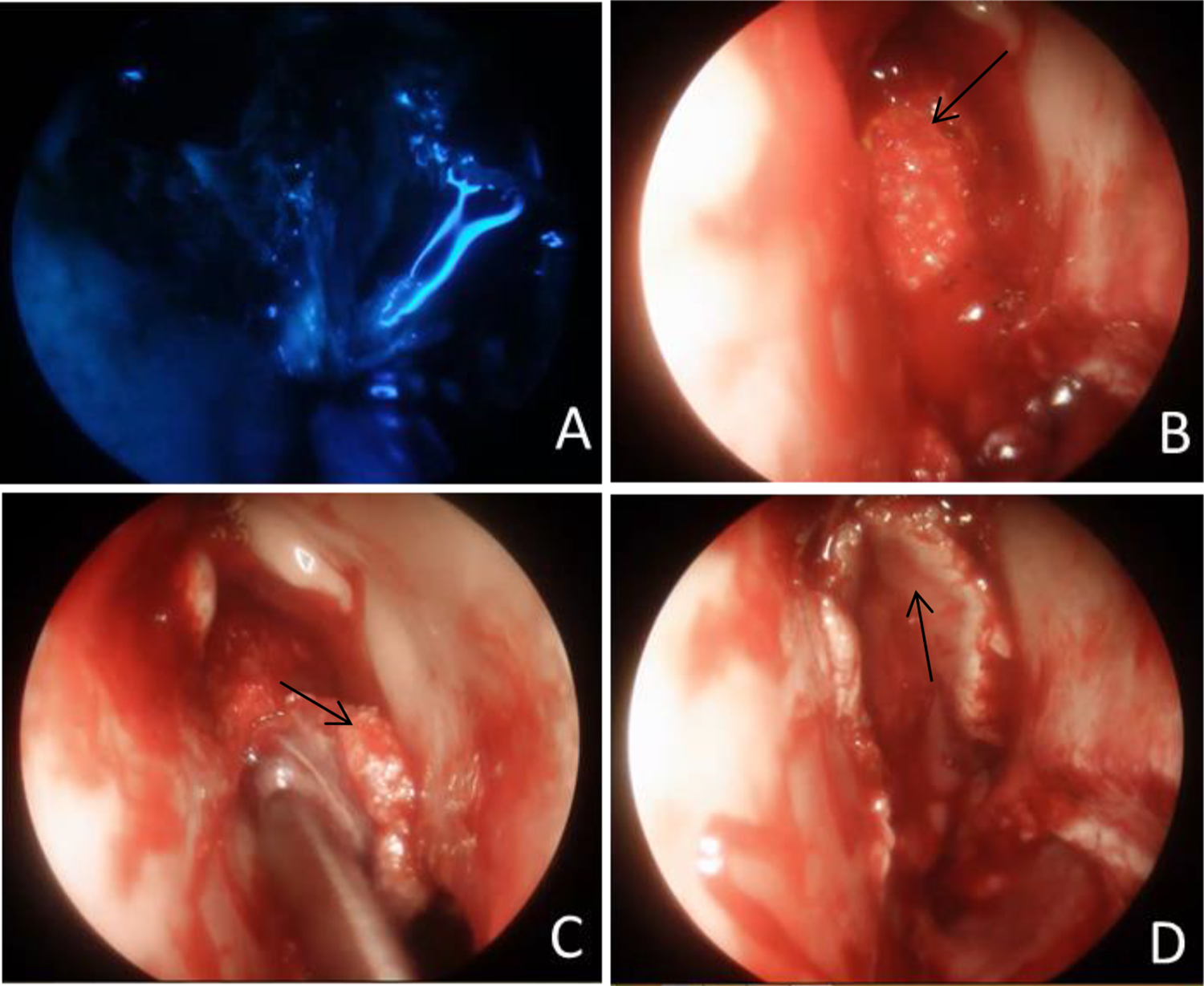
A, Intraoperative fluorescein imaging to detect a potential CSF leak (B) fibrin patches applied to the skull base defect (C) the denuded septum with the pedicled nasoseptal flap (NSF) brought into position for defect coverage (D) the nasoseptal flap rotated in its final position covering the skull base defect.
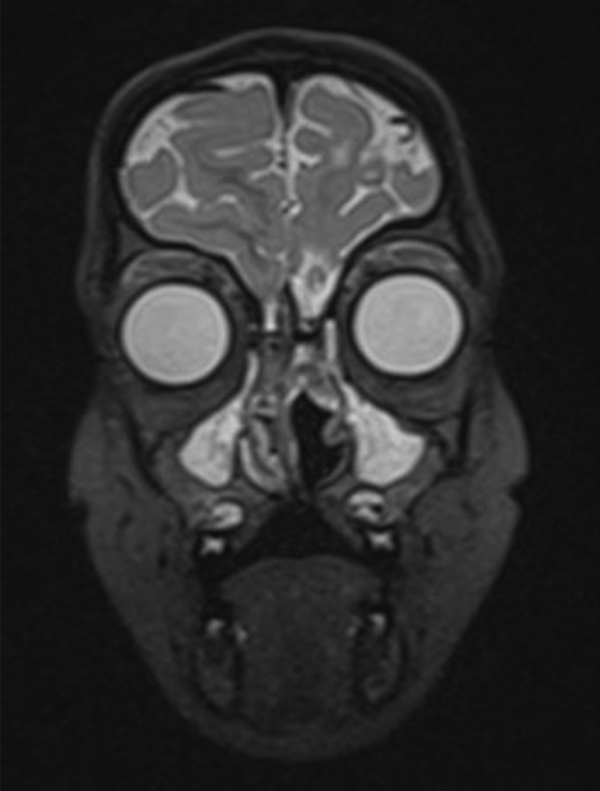
Postoperative coronal T2 MRI scan showing the flap coverage of the skull base and the resection of the middle turbinate of the left nasal cavity. MRI indicates magnetic resonance imaging.
Discussion
The pediatric skull base presents multiple anatomic challenges, including variable patterns of pneumatization, narrow piriform aperture width, and narrow intercarotid distance at the level of the cavernous sinus. 5 These issues may be particularly challenging in patients less than 2 years of age. Shah et al. stated, that based on normal growth trends, and their individual experience, the potential dimensions of the nasoseptal flap (NSF) are insufficient to cover some larger skull base defects early in childhood. It is not until adolescence when septal length approaches the full size and is adequate for endoscopic endonasal approach reconstruction. 6 In opposition, Ghosh et al reported that the NSF was sufficient and provides a reliable coverage option in the reconstruction of suprasellar defects in pediatric patients. 7 They demonstrated that septal lengths in children less than 10 years of age were adequate to cover defects created by suprasellar resections, as younger patients tend to have greater NSF length relative to the length of their sellar defects. Ghosh et al underlined how critical the preoperative radiographic assessment of the nasoseptal flap feasibility is to ensure adequate flap coverage. Nowadays, the nasoseptal flap (or Hadad-Bassagasteguy flap) is the most common pedicled regional flap used for the transnasal reconstruction of the meninges. A NSF vascularized by the sphenopalatine artery was first described in 1952 by Hirsch, 8 but not popularized until 2006 by Hadad and Bassagasteguy. 9 After their successful reintroduction of this technique, the authors could demonstrate the reduction of postoperative CSF leaks down to 5% in a series of 43 adult patients who underwent skull base reconstruction. In the last decade, multiple approaches have been used to apply this technique to the pediatric population. Endoscopic endonasal approaches have been applied to a multitude of conditions and lesions of the anterior pediatric skull base. Open approaches are still necessary in the setting of extensive intracranial or orbital disease, as well as disease lateral to critical neurovascular structures. Furthermore, the difficulty in reconstructing larger defects using this flap as well as the difficulty in obtaining a sufficient length and width for coverage may influence the choice of best surgical procedure.5,10 The primary aim in reconstruction is to reliably close the connection between the intradural and extradural spaces. As the best surgical choice for the treatment of frontoethmoidal meningoencephaloceles is still debated, our case shows the successful transnasal endoscopic resection and closure of the skull base defect. Meticulous planning and consideration are necessary for this surgical approach including the type and size of the encephaloceles as well as the associated hydrocephalus. 11 In our case of a nasofrontal meningoencephalocele, the 3-year-old patient underwent four prior open neurosurgical approaches at an outside hospital. In retrospect, a transnasal approach should have been considered at an earlier stage. The nasoseptal flap satisfies the most reconstructive needs of an endoscopic endonasal surgery at the skull base. A reliable vascular supply promotes rapid healing and is an effective barrier for the prevention of CSF leaks. It has a good arc of rotation and can reach defects of the ventral skull base from the cribriform plate to the foramen magnum. In the literature most examples of endoscopic repairs of skull base defects are focused on the adult population. There is only very limited data demonstrating successful outcomes in pediatric population. Given the inherent difficulties in the diagnosis of these lesions coupled with their rare occurrence, endoscopic management represents a unique challenge to the pediatric otorhinolaryngologist. 12 The anaesthetic impacts also need to be considered. The cranio-orbito-zygomatic skeleton reaches 85% of adult size by 5 years of age. The nasofacial second growth peak occurs at a mean age of 13.1 years for females and 14.7 years for males. 5 Among the essential growth zones, the sphenodorsal center plays a critical role in the development of the bony and cartilaginous skeleton of the midface. Even though there is a concern of damaging and affecting the growth centers of the underdeveloped skull during skull base surgery, recent publications in patients undergoing functional endoscopic sinus surgery demonstrate no impact on the midface growth. 5 Last but not least, our young patient developed a generalized epileptic seizure after the third transcranial procedure, which has to be acknowledged as a severe side effect of repeated open approaches. Even though there are potentially severe complications in endonasal endoscopic approaches as well, these are far less common, and recovery is often much more rapid than after open procedures. 13 A study by Ma et al states that compared to traditional operations, this endoscopic procedure is minimally invasive, efficient, and safe. According to this publication, the endoscopic endonasal approach is the preferred method for repairing CSF leaks with or without an encephalocele in pediatric patients. 14 In conclusion, the importance of an interdisciplinary team approach to skull base surgery cannot be overestimated. It requires specialized knowledge of the 3-dimensional relationships between the region of interest and the critical structures. Research has shown that effective collaboration is improved with increased case volume and consistent roles within the otolaryngological and neurosurgical team. 15
Conclusion
Congenital ASB defects with meningoencephaloceles and CSF leaks are rare clinical entities. An interdisciplinary approach is vital including experienced pediatricians, otolaryngologists, and neurosurgeons to evaluate the ideal surgical method on an individual basis. The transnasal endoscopic technique has been shown to be minimally invasive, efficient, and safe to apply even to the infant population which could positively be demonstrated in this case. With increasing literature describing high success and low complication rates in children, the endoscopic endonasal approach should be considered as a feasible therapeutic option to transcranial surgery in selected cases.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.