
Abstract
Laryngopharyngeal or cervical pain following ingestion of foreign bodies is one of the most frequently encountered emergencies in otolaryngologic practice. Although most of these foreign bodies can be easily removed under laryngoscopic examination without any complications, surgical removal may be required when foreign bodies migrate extraluminally. This report describes two rare cases of ingested fishbones that had migrated, one each to the thyroid gland and submandibular gland. Extraluminal migration fishbones should always be considered in otolaryngologic clinics.
Introduction
Food materials and other substances passing through the oral cavity may act as laryngopharyngeal foreign bodies; fishbones constitute more than 85% of these foreign bodies. Most laryngopharyngeal foreign bodies can be easily identified by thorough history taking, laryngoscopic examination, and simple X-ray. Prompt removal of foreign bodies usually results in full recovery without sequelae, whereas delayed detection and removal can result in serious complications. Moreover, laryngopharyngeal foreign bodies can mimic the symptoms of other conditions, such as chronic sialadenitis. Extraluminal migration of foreign bodies can also occur, even though its incidence is rare. Therefore, the presence of laryngeal foreign bodies cannot be excluded, although foreign bodies may be undetectable on laryngoscopic examination or simple X-rays. Computed tomography (CT) of the neck can be used to diagnose patients with suspected extraluminal migration of foreign bodies.
Case 1
A 60-year-old woman presented to the emergency room with persistent right neck pain, which started one hour earlier after eating fish for dinner. Physical examination showed no signs of neck swelling or mass and normal intra-oral findings. An air-tracheogram and laryngoscopic examination showed no evidence of a foreign body in the pharynx or larynx. A contrast-enhanced neck CT scan revealed a linear high-density lesion, about 2 cm in size, in the hypopharynx and cervical esophagus (Figure 1A and B). Removal was attempted through a gastroesophageal endoscope, but no foreign bodies were visible. Because the patient continued to experience throat pain and odynophagia, a contrast-enhanced neck CT scan was performed, which showed that the fishbone had migrated to the upper part of the right lobe of the thyroid gland (Figure 1C and D). Representative axial (A) and coronal (B) images of preoperative CT scans in Patient 1, showing a linear calcified foreign body-like lesion (arrow) located in the superior portion of the right thyroid lobe. Representative axial (C) and coronal (D) images of preoperative follow-up CT scan in Patient 1, showing that the fishbone (arrow) had migrated to the upper part of the right lobe of the thyroid gland. (E) Representative image of the operating field in Patient 1, showing the fishbone (arrow) in the superior portion of the right thyroid gland. (F) Photograph of the fishbone removed from Patient 1. This fishbone measured 2.5 cm in length. CT, computed tomography.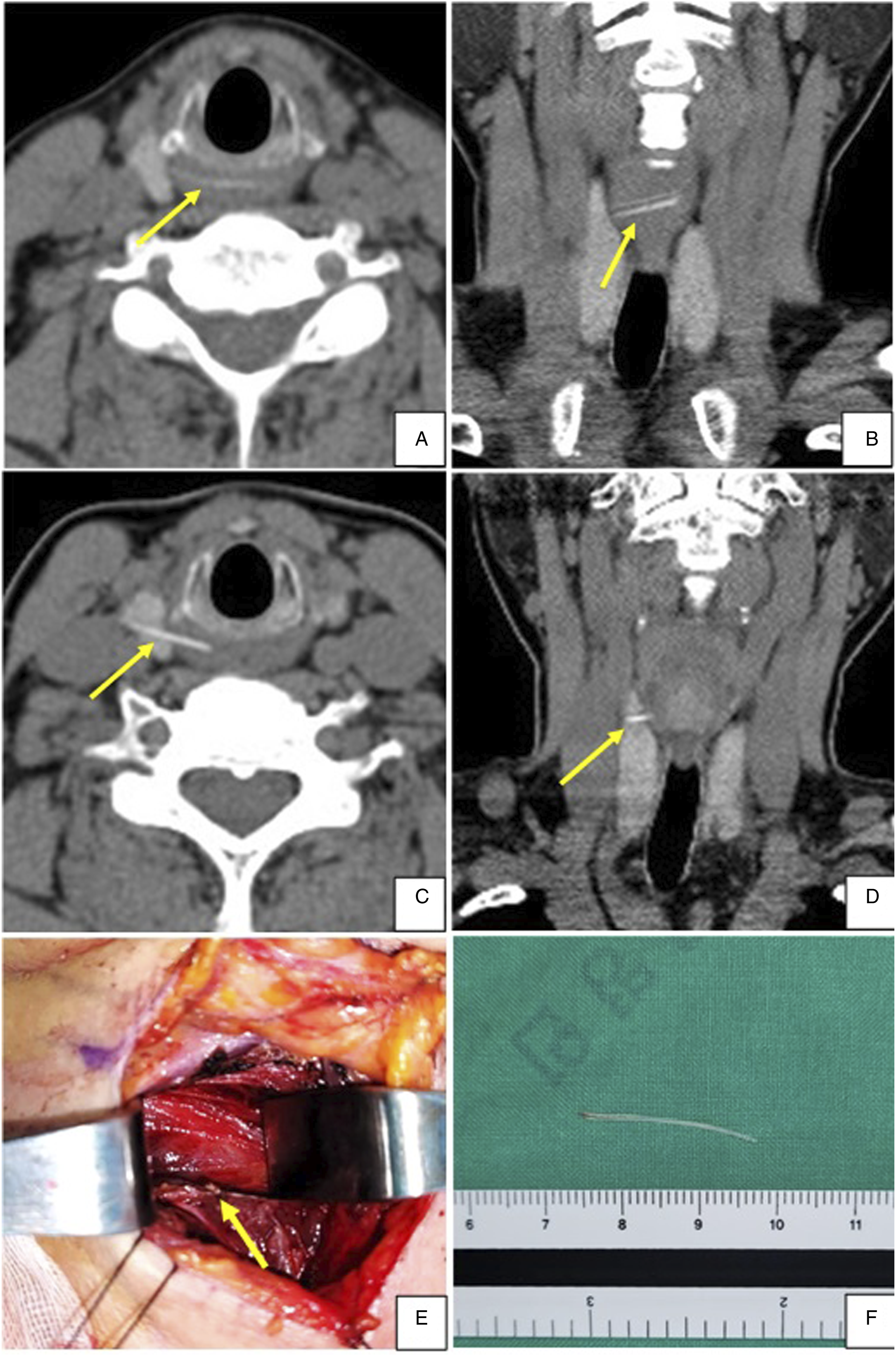
The patient underwent surgical neck exploration through an external approach under general anesthesia to remove the foreign body. After separating the upper part of the right lobe of the thyroid gland from the thyroid cartilage, the tip of the fishbone could be palpated (Figure 1E). The fishbone, which was about 2.5 cm in size, was removed completely (Figure 1F). A follow-up CT scan showed no remaining foreign body.
The patient was discharged one week after surgery without any postoperative complications. Follow-up two months later showed that her postoperative course was uneventful.
Case 2
A 59-year-old woman presented to an outpatient clinic with right submandibular swelling and pain, beginning three months earlier. The patient reported that her submandibular pain tended to worsen after eating. A slightly firm and enlarged right submandibular gland was palpable on physical examination. Laryngoscopic examination showed no pathologic lesions in the oral cavity, pharynx, and larynx. Contrast-enhanced neck CT, however, showed a linear, hyperdense lesion in the right submandibular gland (Figure 2A and B). The patient was initially diagnosed with chronic sialadenitis caused by sialolithiasis and underwent submandibular gland resection under general anesthesia. Although submandibular gland resection was successful without any complications, a 1 cm-sized fishbone was detected inside the right submandibular gland (Figure 2E). The resected submandibular gland showed fibrotic changes and chronic inflammation with lymphoid aggregation, consistent with the histopathologic features of chronic sialadenitis (Figure 2C and D). These findings suggested that fishbone inside the submandibular gland acted as a sialolith. The patient was discharged five days after surgery without any postoperative complications. Her postoperative course was uneventful, and there were no indications of swelling after eating. Representative (A) and coronal (B) images of preoperative computed tomography scans in Patient 2, showing a small, linear hyperdense lesion (arrow) in the right submandibular gland. Submandibular gland of Patient 2, showing replacement of fibrosis (arrow) and lymphoid aggregation (C) H&E ×40; (D) H&E ×200. (E) Photograph of the resected submandibular gland containing the fishbone (arrow) from Patient 2. The submandibular gland measured 1.0 cm in length.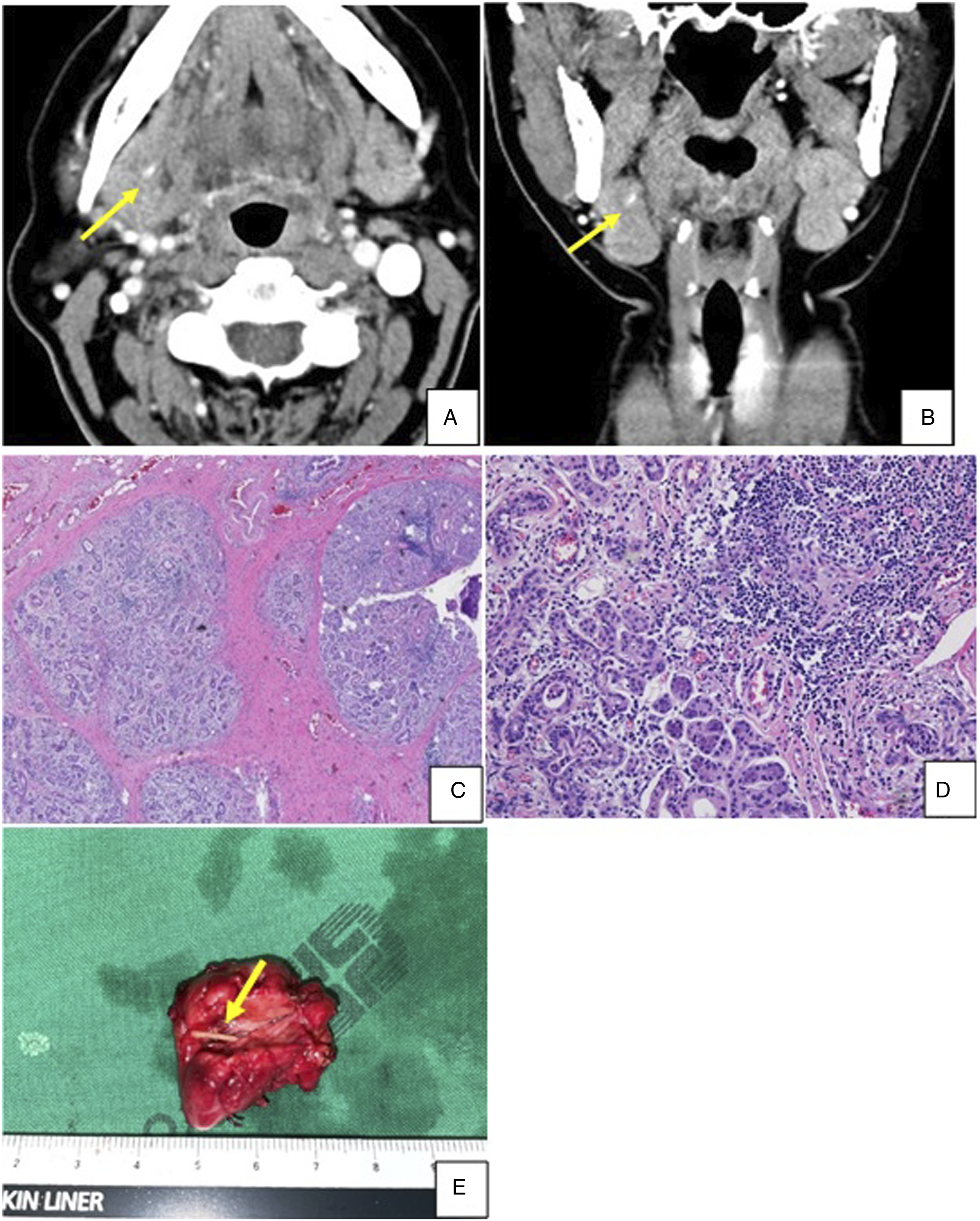
Discussion
Foreign bodies in the laryngopharyngeal area are not uncommon 1 and can occur regardless of sex, age, and ethnicity. 2 Small beans and coins are the foreign bodies most frequently ingested by children, whereas fishbones are most common in adults. 3 Most fishbones can be easily detected by endoscopic examination, suggesting that endoscopic examination should be performed in patients with a history of fishbone ingestion. Because fishbones are long and sharp, they can injure mucosa, perforate the esophagus, and migrate extraluminally. 4 Sites of extraluminal fishbone migration can be diverse space, including salivary glands and deep cervical space. 5 Consequences of extraluminal migration can include various complications, such as sialadenitis with granulation tissue growth, cervical abscess formation, and even rupture or fistula formation of the carotid artery.6-8 Therefore, extraluminal migration of fishbones should be considered in the differential diagnosis of patients with persistent neck pain despite normal findings on endoscopic examination. 9
CT is a highly versatile tool in persons suspected of having extraluminally migrated fishbones, as it can provide a “roadmap” for surgical intervention and help estimate the locations and sizes of foreign bodies, as well as injuries to structures adjacent to the fishbone.10,11 Visible pharyngeal foreign bodies can be removed during the endoscopic examination, 2 whereas surgery is optimal for extraluminally migrated foreign bodies. Sufficient dissection and debridement of adjacent necrotic tissues may also be required. 12 During surgery, however, the foreign body may not be at the same location as on the CT scan. 10 In such cases, C-arm or intraoperative ultrasound can be useful to localize the foreign bodies. 4 Foreign bodies in the thyroid or salivary glands may require removal by thyroidectomy or submandibular gland resection to secure a clearer operative field view.10,13 Intravenous antibiotics following surgery may prevent abscess formation and/or shorten hospitalization time. 14
In conclusion, this report describes two patients who underwent successful surgical removal of ingested fishbones that had migrated extraluminally, one each to the thyroid gland and submandibular gland. If clinics belong to the region that tends to consume large quantities of fish, fishbone should be regarded as one of the causes of throat pain even though foreign bodies are not detectable through laryngoscopy, gastroesophageal endoscopy, or simple X-ray. Extraluminal migration fishbones are rare in otolaryngology clinics, but we should pay much attention to avoid delayed diagnosis and misdiagnosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.