
Abstract
Sinonasal inverted papilloma (IP) is the most common benign tumor in sinonasal cavities. Treatment involves excising the whole tumor, so it is essential to evaluate the extent of the tumor by preoperative radiographic findings. Magnetic resonance imaging (MRI) is superior to computed tomography (CT) for determining a tumor’s location as MRI can discern the difference between mucus and IP. We herein report a 51-year-old man with sinonasal IP treated with endoscopic sinus surgery (ESS). Preoperative MRI showed findings resembling a convoluted cerebriform pattern on T2-weighted imaging, but this site was not enhanced by intravenous gadolinium at all. We preoperatively suspected that this site was not part of the tumor but rather the accumulation of mucus, and indeed, we found no tumor at this site when we performed the surgery. This patient is a valuable example of misleading findings of IP on T2-weighted imaging and underscores the importance of contrast-enhanced T1-weighted imaging to determine the extent of IP.
Introduction
Sinonasal inverted papilloma (IP) is a benign sinonasal epithelial tumor. The rates in sinonasal cavity tumor range between 0.4% and 7%. Distinguishing IP from nasal polyps and inflammatory mucosa is occasionally challenging. 1
A pathologic examination is essential for a diagnosis, and a precise diagnosis is difficult based on radiographic findings alone. However, computed tomography (CT) and magnetic resonance imaging (MRI) are valuable for determining the extent of the tumor. 2 These modalities can aid in choosing the most appropriate surgical approach for IP treatment. MRI is more helpful than CT because it can differentiate the mucus from the tumor. 3 Evaluating the accurate location of the tumor allows us to make an adequate preoperative plan, thus preventing unnecessary invasive operations attributed to overestimating the extent of IP.
We herein report a 51-year-old man diagnosed with sinonasal IP. On preoperative MRI, the mass in the left frontal sinus showed findings resembling a convoluted cerebriform pattern on T2-weighted imaging, but it was totally not enhanced by intravenous gadolinium. We would have misunderstood the extent of the tumor if we had not performed T1-weighted, gadolinium-enhanced imaging. This case suggests that MRI should be performed, including both T2- and T1-weighted, gadolinium-enhanced imaging, to determine the most reasonable surgical approach for IP treatment.
Case report
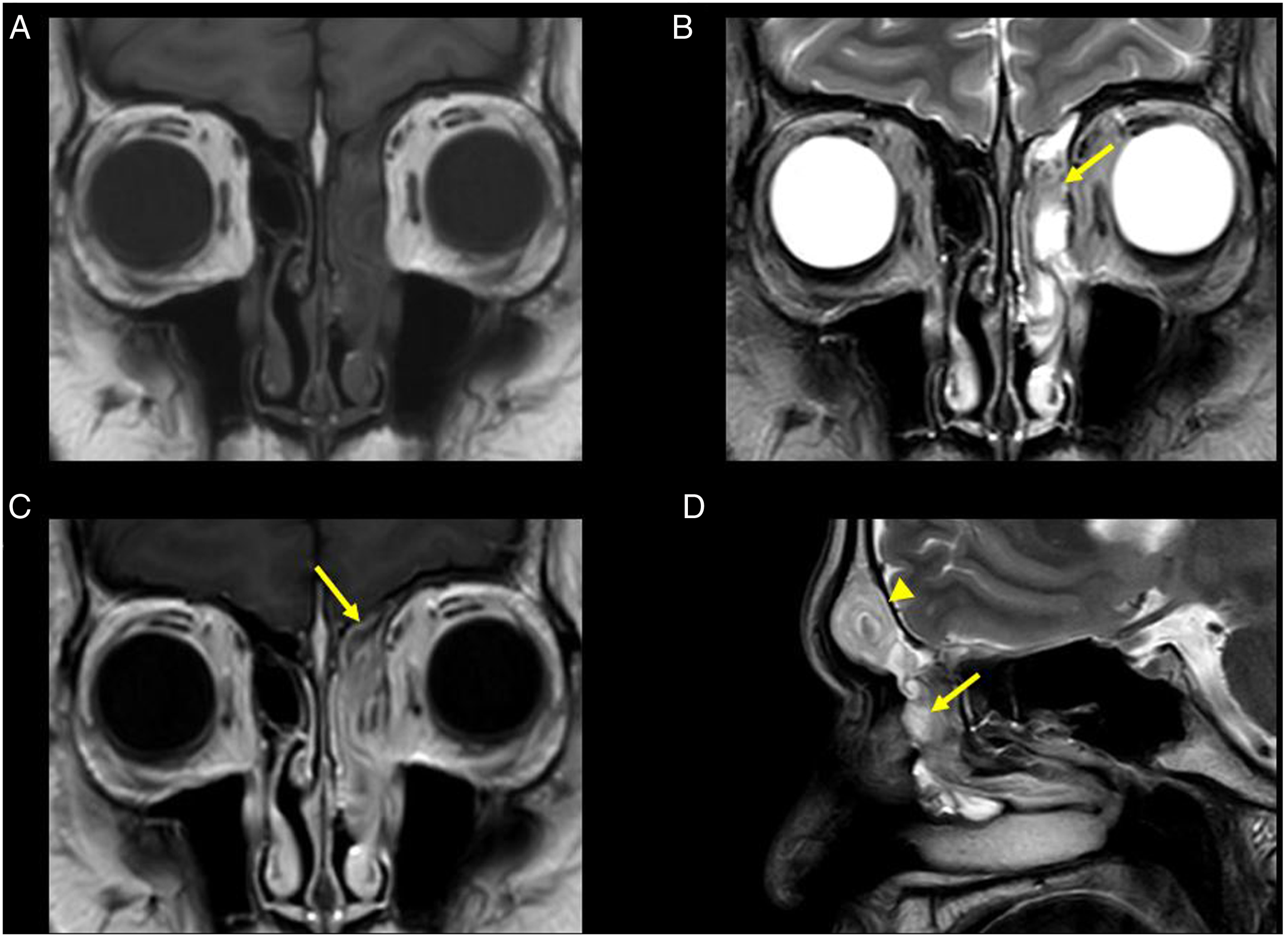
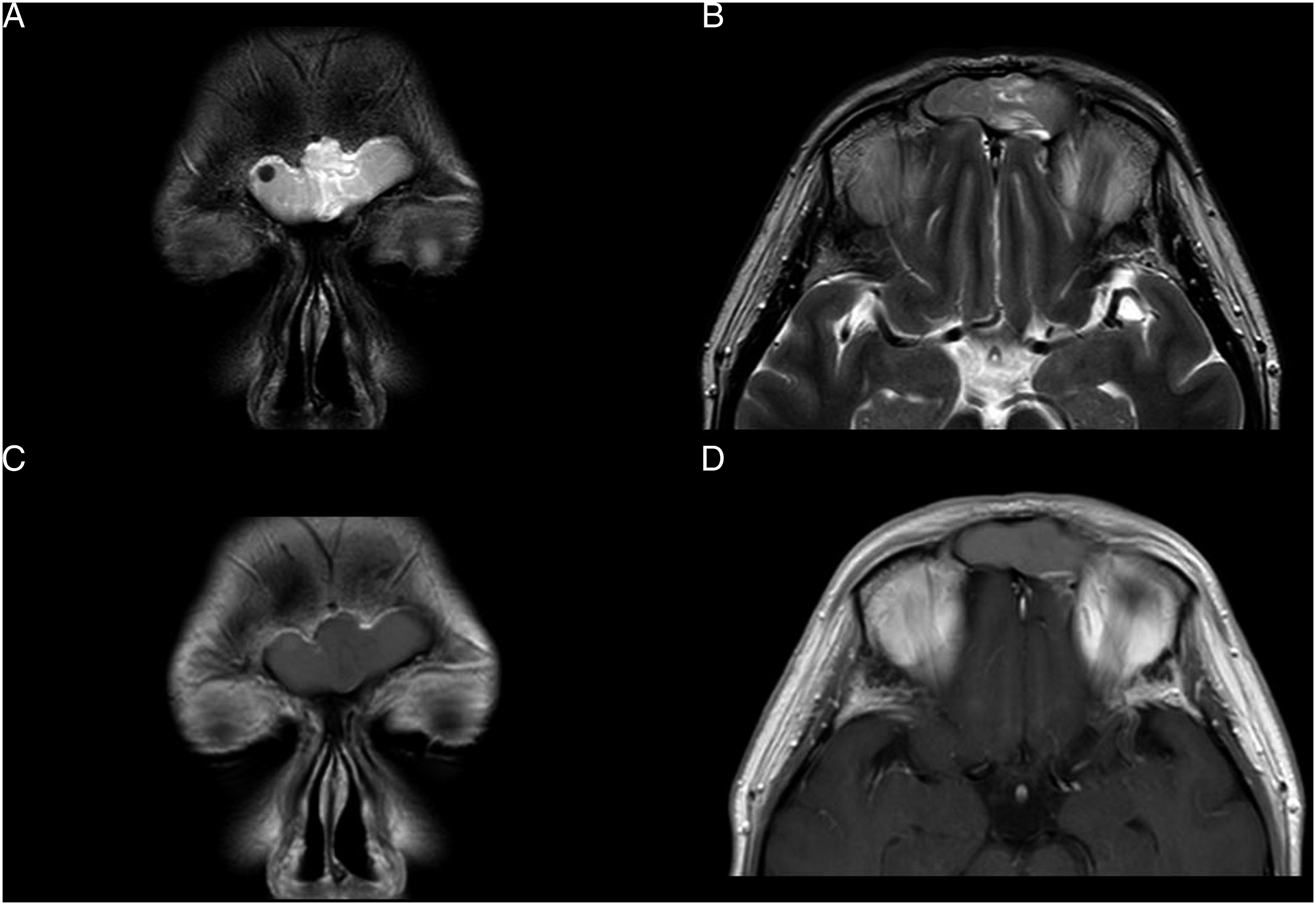
A 51-year-old man presented to our hospital because of a mass in the left nasal cavity found at a nearby otolaryngology clinic. He complained of left nasal congestion. Endoscopic exploration revealed a tumor occupying the left middle meatus and nasal cavity. CT showed a soft-tissue mass extending over the left frontal sinus, anterior ethmoid sinus, middle meatus, and nasal cavity (Figure 1). We also performed MRI. On T1-weighted sequences, the mass in the left anterior ethmoid sinus, middle meatus, and nasal cavity showed a hypointense signal (Figure 2A). On T2-weighted imaging, the mass demonstrated a high-intensity signal in the left middle meatus, nasal cavity, and most of the ethmoid sinus. It appeared to have a convoluted cerebriform pattern in part of the anterior ethmoid sinus (Figure 2B). Furthermore, the mass was diffusely enhanced with a convoluted cerebriform pattern, and part of the ethmoid mucosa demonstrated enhancement (Figure 2C). The mass in the left frontal sinus showed findings similar to a convoluted cerebriform pattern on T2-weighted imaging (Figures 2D, 3A, B) but did not show any enhancement (Figure 3C, D). A. Coronal CT shows a soft-tissue mass over the left anterior ethmoid sinus, middle meatus, and nasal cavity. B. Sagittal CT shows the soft-tissue mass occupying the left frontal sinus. Images of inverted papilloma on MRI. A. T1-weighted coronal imaging shows a hypointense mass occupying the left anterior ethmoid sinus, middle meatus, and nasal cavity. B. T2-weighted coronal imaging shows that the mass mainly has a high-intensity signal and appears to have a convoluted cerebriform pattern in part of the left ethmoid sinus (arrow). C. Coronal contrast-enhanced T1-weighted imaging shows that the mass is diffusely enhanced with a convoluted cerebriform pattern. At the same time, the ethmoid mucosa demonstrates partial peripheral enhancement (arrow). D. T2-weighted sagittal imaging confirms a convoluted cerebriform pattern of the mass in part of the left ethmoid sinus (arrow) and a finding resembling a convoluted cerebriform pattern in the left frontal sinus (arrowhead). Imaging of the frontal sinus on MRI. A, B. T2-weighted imaging shows a convoluted cerebriform pattern. C, D. Contrast-enhanced T1-weighted imaging shows unenhanced frontal sinus contents.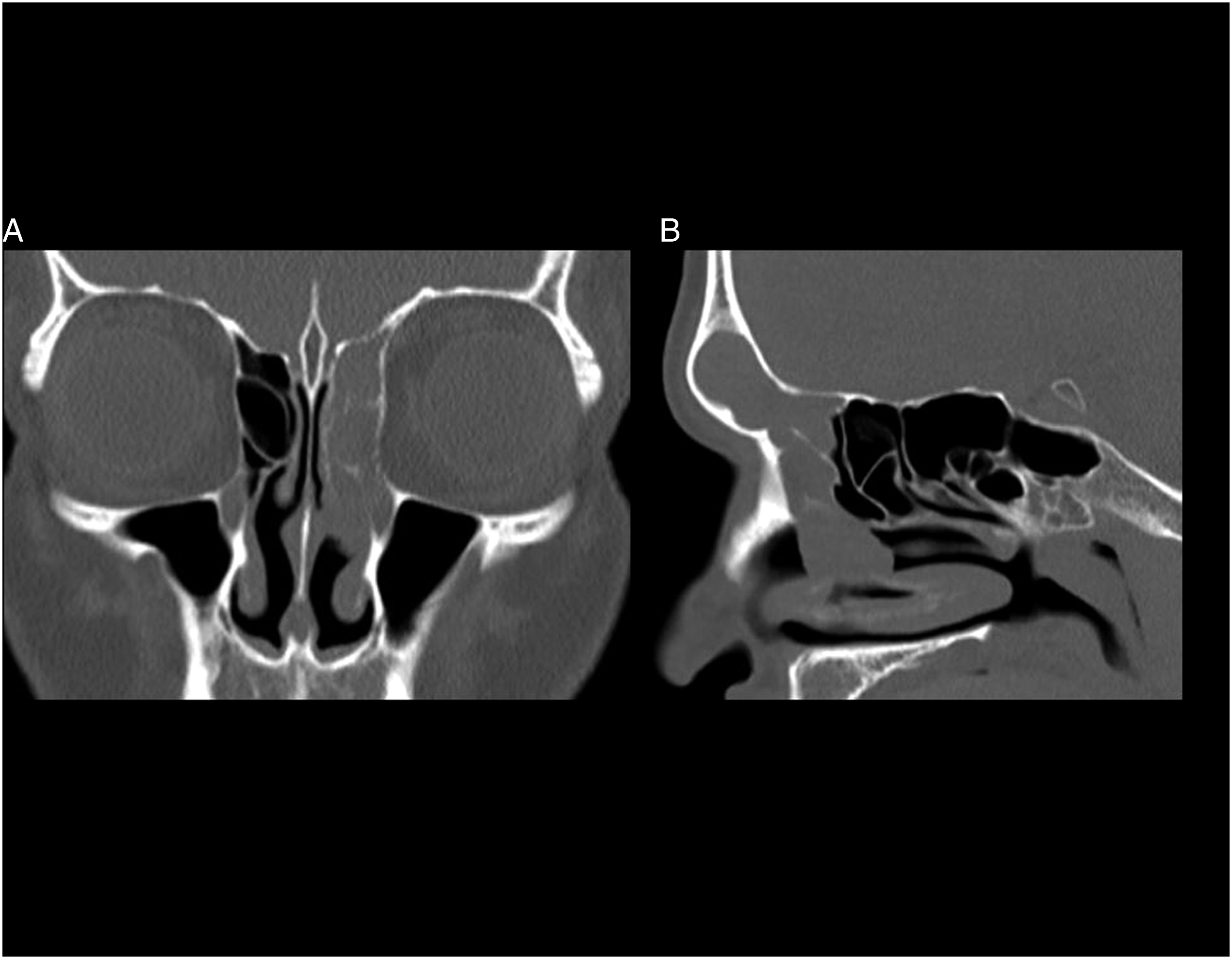
We performed endoscopic sinus surgery (ESS) and resected all of the tumors. The site of the primary lesion was the left frontal recess. There was no mass in the frontal sinus, and instead, it was filled with mucus. Pathological findings showed the invagination of the superficial epithelium into the underlying stroma, which is typical of IP. There was no sign of malignancy.
Discussion
We experienced a patient with sinonasal IP that showed a misleading signal on MRI. The preoperative MRI findings were confounding, but we were able to anticipate the extent of IP and choose a minimally invasive surgical approach because the lesion in the left frontal sinus was not enhanced by intravenous gadolinium. Our case indicates that both T2-weighted and contrast-enhanced T1-weighted imaging are indispensable for confirming the accurate extent of IP.
MRI is useful for determining the extent of sinonasal IP. 3 T2-weighted sequences and contrast-enhanced T1-weighted imaging show a convoluted cerebriform pattern, typical of IP, thereby enabling the differentiation of IP from inflammatory changes. 1 On T2-weighted imaging, IP usually shows intermediate signal intensity, while inflammatory processes show bright signal intensities, reflecting edema, serous fluid, and mucous secretion. 2 However, the findings in the left frontal sinus of our patient appeared to be a convoluted cerebriform pattern on T2-weighted imaging despite no tumor being identified there. We would have misunderstood the extent of IP if we had not checked the findings of contrast-enhanced T1-weighted imaging as the mass in the left frontal sinus was not completely enhanced, and this finding contradicts the general features of IP, which are usually enhanced homogeneously with intravenous gadolinium. 4
There have been several reports of sinus mucocele wherein a high-intensity signal on T2-weighted sequences consequently decreased and became more heterogeneous with time, reflecting the increased protein level or thick mucus of the lesion.5,6 We suspect that the different concentration of protein in the mucus in the left frontal sinus caused the findings to resemble a convoluted cerebriform pattern on T2-weighted imaging. We should be alert for such misleading findings to avoid overestimating the extent of IP and performing a more invasive operation than is necessary.
Enhanced MRI should be performed in all IP-suspected patients, except for those with a history of anaphylactic/anaphylactoid reaction to gadolinium-containing contrast agent, patients with a low estimated glomerular filtration rate, and those with an acutely deteriorating renal function. If only T2-weighted imaging is available, the potential for mucus with variable intensity should be kept in mind.
Conclusion
We encountered a 51-year-old man with sinonasal IP. Preoperative MRI of the left frontal sinus showed findings resembling a convoluted cerebriform pattern on T2-weighted imaging, but this site was not enhanced by intravenous gadolinium. These findings may have been due to variable protein content or mucus in the sinus. We should consider such misleading findings when determining the extent of IP.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the JSPS KAKENHI [grant number JP19K08948].
Ethical approval
The authors assert that all procedures contributing to this work comply with the ethical standards of the 1975 Declaration of Helsinki, as revised in 2008. I have obtained written informed consent but the written consent itself should be held by the authors themselves in a patient’s hospital record.