
Abstract
Keywords
Introduction
Allergic rhinitis (AR) is a common disorder that negatively affects a patient’s quality of life (QOL) and performance in work or academics. 1 Its prevalence is reportedly 27%–32% in Asia and 40% in children in Taiwan.2,3 This immunoglobulin E (IgE)–mediated inflammatory disorder is frequently related to other comorbidities such as asthma, rhinosinusitis, sleep disturbance, and psychiatric conditions. 4
Typical presentations of AR include pruritus, sneezing, nasal obstruction, and watery rhinorrhea. The most bothersome symptom, nasal obstruction, can result from nasal mucosal congestion due to allergic reactions5,6 or a combination with structural problems such as a deviated nasal septum and hypertrophic inferior turbinates caused by long-term allergen exposure. 4 The medical treatment of AR includes allergen avoidance and medications such as anti-histamines, intranasal corticosteroid sprays, and decongestants. 7 Previous studies described numerous surgical treatments for nasal obstruction. For example, septoplasty alone proved more effective than non-surgical management in patients with nasal obstruction and a deviated nasal septum, especially young patients.8,9 Moreover, AR patients could benefit from either septoplasty or inferior turbinoplasty to address other types of obstruction.10,11 A previous study revealed that AR patients reported greater nasal obstruction relief after septoplasty with turbinate surgery than after turbinate surgery alone. 11 Some AR patients with apparent structural problems that interfere with nasal airflow choose surgical rather than medical treatment due to medication side effects. For instance, antihistamines may cause sedation, which worsens academic or work performance. 1 In such situations, septoplasty with turbinoplasty is favorable and feasible, as it effectively corrects the nasal septum deformity and decreases the inferior turbinate volume, the major cause of nasal obstruction, decreasing nasal resistance, and increasing the nasal cavity space.
Nevertheless, no study to date has analyzed the factors related to the outcomes of septoplasty with turbinoplasty in patients with AR. Therefore, this prospective study aimed to determine the surgical effects in patients with AR and identify preoperative subjective or objective factors that may be linked to surgical outcomes.
Material and Methods
Patient Selection and Postoperative Management
Patients with one or more typical symptoms of AR that persisted for 4 consecutive weeks (categorized as persistent allergic rhinitis, PAR), 12 a positive serum allergy test (Phadiatop®, Pharmacia, Sweden), and a deviated nasal septum were prospectively recruited. The symptoms were refractory to medical therapy for at least three months. All medications were discontinued two weeks prior to surgery. We excluded patients with previous sinonasal surgeries, facial trauma, or those who did not complete a postoperative follow-up period of one year.
Surgery was performed under local anesthesia by a single surgeon. We performed submucosal correction of the deviated nasal septum and submucosal resection of the hypertrophic inferior turbinates. After surgery, nasal packs (Nasopore®, Polyganics, Groningen, The Netherlands) were used to prevent postoperative hemorrhage or septal hematoma. A postoperative oral regimen of amoxicillin (500 mg every 8 hours) was administered for three days, and nasal cavity debridement was initiated in the first week postoperatively for two weeks. All patients completed postoperative follow-up on a weekly basis for one month, on a two-month basis for six months, and then every three months.
Subjective and Objective Measurements
We administered the Taiwanese version of the Sinonasal Outcome Test-22 (SNOT-22) 13 one day before and one year after surgery as a subjective assessment. The SNOT-22 has been commonly applied in sinonasal symptom surveys, with each item score ranging from 0 (no symptoms) to 5 (most severe) and further divided into 5 subdomains, including rhinologic, extranasal, ear/facial, psychological, and sleep symptoms.14,15 Smoking status and major complaints, such as obstructive or non-obstructive symptoms, were recorded for further analysis. Preoperative laboratory data included serum eosinophil counts, eosinophil cationic protein (ECP) levels, and IgE levels. Absolute improvement in the SNOT-22 score was defined as the difference between the pre- and postoperative scores, whereas relative improvement was defined as the aforementioned difference divided by the preoperative score. If the improvement in SNOT-22 score was greater than the minimal clinically important difference (MCID), which has been defined as 8.9 for sinonasal diseases, it would suggest that the treatment significantly improved the patient’s QOL. 15 Factors potentially associated with achieving MCID in the SNOT-22 subdomains were also analyzed. Patients were under regular outpatient department follow-up for at least one year after surgery.
Statistical Analyses
SPSS version 22 statistical software program (IBM, Chicago, IL, USA) was used to perform all of the statistical analyses. Intergroup comparisons were made using Fisher’s exact test and Mann–Whitney U test for categorical and continuous variables, respectively. The Wilcoxon signed-rank test was used to compare pre- and postoperative differences in total SNOT-22 score, its 5 subdomains, and total SNOT-22 score according to patient characteristics. Logistic regression analysis was used to determine the association between the clinical factors and postoperative MCID achievement. A receiver operating characteristic (ROC) curve was constructed to determine the optimal preoperative SNOT-22 score for achieving MCID. Uni- and multivariate linear regression analyses were applied to determine the factors that impacted the absolute and relative postoperative improvements in symptom scores. All tests were two-tailed, and the significance level was set at p < .05.
Results
Study Groups
Characteristics of 128 Persistent Allergic Rhinitis Patients According to the Chief Complaint Of Nasal Obstruction And Other Symptoms.
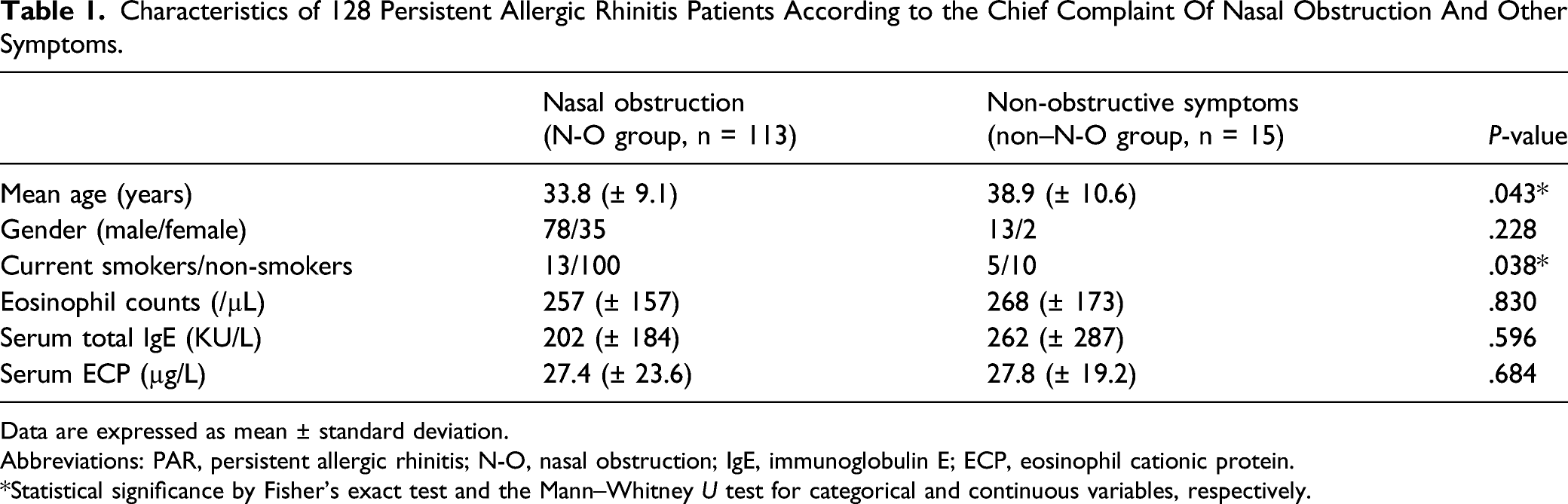
Data are expressed as mean ± standard deviation.
Abbreviations: PAR, persistent allergic rhinitis; N-O, nasal obstruction; IgE, immunoglobulin E; ECP, eosinophil cationic protein.
*Statistical significance by Fisher’s exact test and the Mann–Whitney U test for categorical and continuous variables, respectively.
Impact of Medical Factors on Postoperative SNOT-22 Score
Comparison of Pre- and Postoperative SNOT-22 Scores by Patient Characteristic.
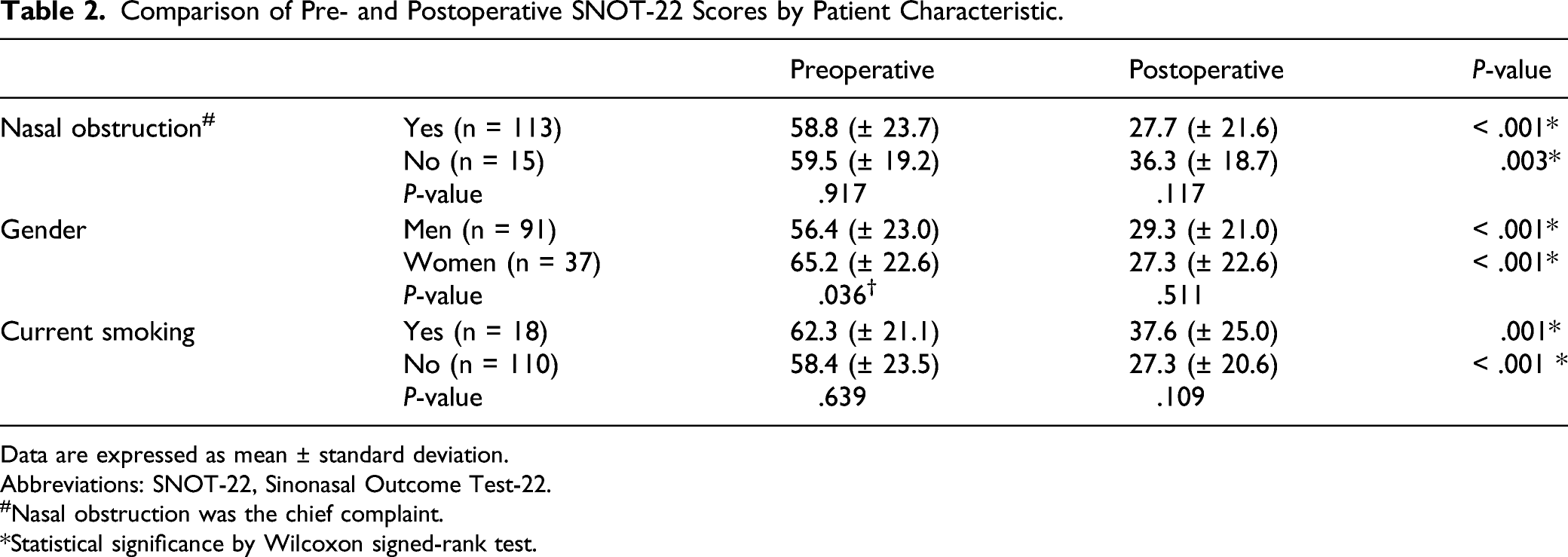
Data are expressed as mean ± standard deviation.
Abbreviations: SNOT-22, Sinonasal Outcome Test-22.
#Nasal obstruction was the chief complaint.
*Statistical significance by Wilcoxon signed-rank test.
Impact of Medical Factors on MCID Achievement
The MCID for the rhinologic, extranasal, ear/facial, psychological, and sleep subdomains of the SNOT-22 were identified as 3.8, 2.4, 3.2, 3.9, and 2.9, respectively. 15 We divided the patients according to MCID achievement versus non-achievement. As expected, the group whose postoperative improvement reached MCID demonstrated significantly more absolute and relative improvements in total and subdomain SNOT-22 scores (all P < .001).
Logistic regression was used to analyze the association between related medical factors and postoperative SNOT-22 MCID achievement. The preoperative SNOT-22 score had a marked impact on the achievement of MCID in the SNOT-22 total and subdomain scores (all p < .01). Next, we determined the optimal cut-off value for the preoperative SNOT-22 score using ROC curve analysis. According to Youden’s index, the cut-off value of 42.5 in the preoperative SNOT-22 score provided 82.2% sensitivity and 57.1% specificity for predicting MCID achievement (area under the ROC curve = .717; p = .002; Figure 1) and the odds ratio was 6.175 (95% confidence interval, 2.280–16.726; p < .001). Receiver operating characteristic curve for preoperative SNOT-22 score of persistent allergic rhinitis patients to predict postoperative minimal clinically important difference (MCID) achievement on SNOT-22. SNOT-22, Sinonasal Outcome Test-22.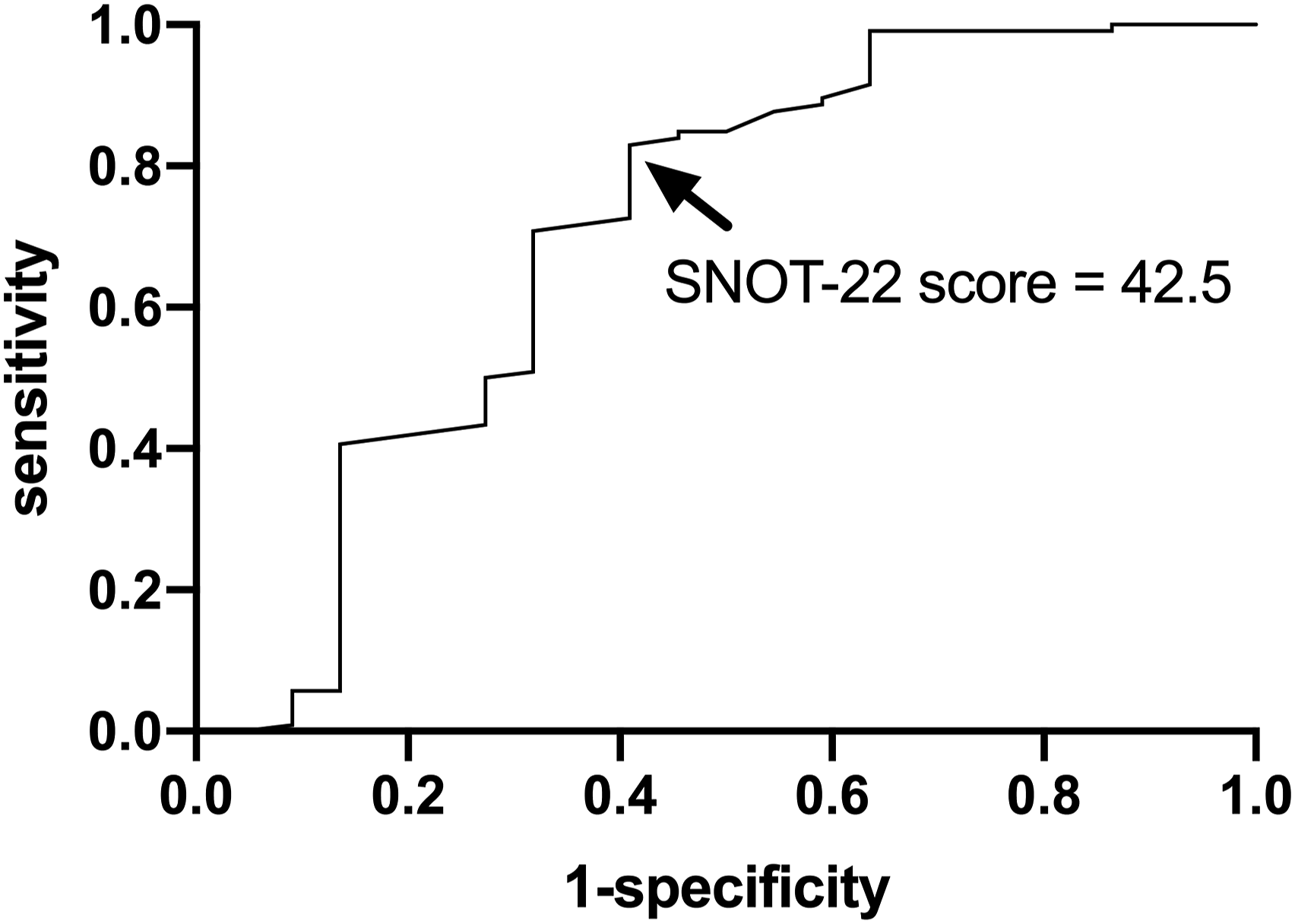
Regression Analysis of Factors Associated With Postoperative Absolute/Relative Improvements in SNOT-22 Scores
Regression Analysis Estimating Association Between Medical Factors and Absolute/Relative Postoperative Improvements of Patients’ SNOT-22 Scores.
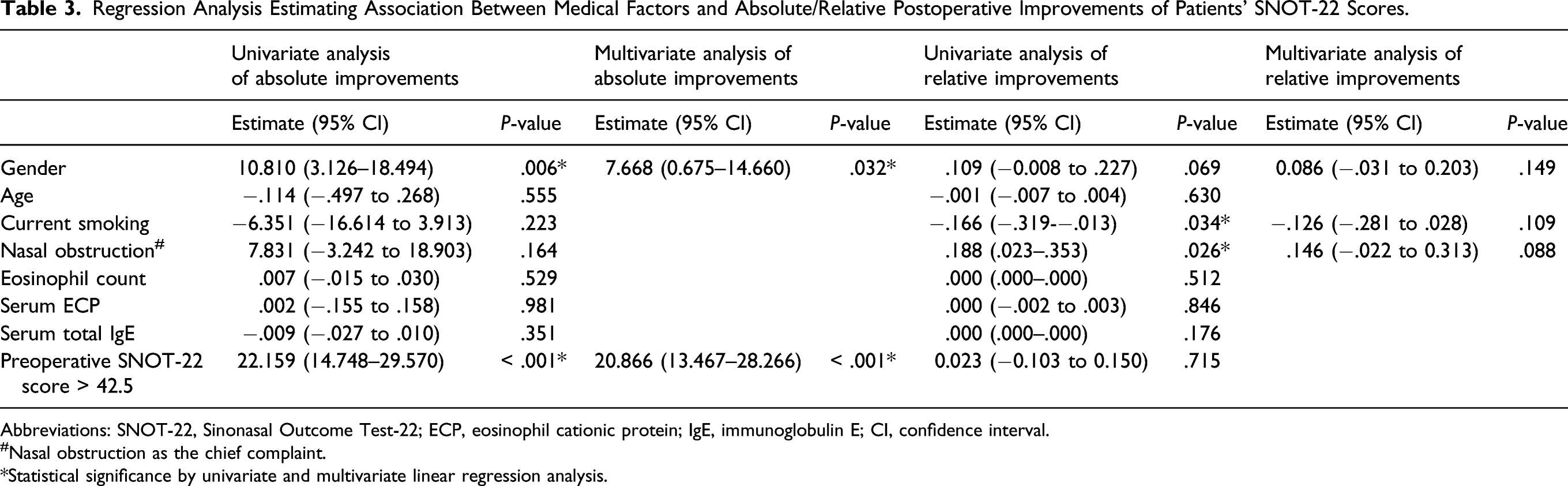
Abbreviations: SNOT-22, Sinonasal Outcome Test-22; ECP, eosinophil cationic protein; IgE, immunoglobulin E; CI, confidence interval.
#Nasal obstruction as the chief complaint.
*Statistical significance by univariate and multivariate linear regression analysis.
Factors Associated With Postoperative Absolute/Relative Improvements in Subdomain Scores
Similarly, medical and demographic factors were further analyzed in relation to postoperative improvements in the 5 subdomains of the SNOT-22. Women had significant absolute improvements in the ear/facial, psychological, and sleep subdomains (P = .015, .009, and .008, respectively). Nonsmokers had more relative ear/facial and sleep improvements (P = .048 and .003, respectively) as well as absolute improvements in sleep symptoms (P = .042). Patients in the N-O group benefited more from surgery in terms of absolute sleep improvements (P = .028) and marginal relative rhinologic improvements (P = .066). As expected, those with preoperative SNOT-22 scores above 42.5 achieved more absolute improvements in all 5 subdomains (all P < .001).
Discussion
Septoplasty with turbinoplasty is often performed in patients with nasal obstruction and prominent anatomic problems. Previous studies reported that AR patients would benefit less from septoplasty alone than those without AR and that turbinate hypertrophy may be another major cause of nasal obstruction.16-18 Patients who underwent septoplasty with turbinoplasty had a reduced revision rate versus those who underwent septoplasty alone, showing that the former was more effective at relieving obstructive symptoms. 18
The SNOT-22 scores in this study showed that surgical treatment improved the QOL of PAR patients at least one year after surgery. This indicates that surgery for a deviated nasal septum and hypertrophic inferior turbinates in PAR patients led to greater airflow patency and spatial symmetry inside the bilateral nasal cavity, bringing significant improvements not only in rhinologic symptoms but also in extranasal, ear/facial, sleep, and even emotional symptoms. This result was similar to that of a recent study showing that turbinate surgery improved QOL in the postoperative period; however, the benefits may decrease with long-term observation. 19
We found that preoperative SNOT-22 score could predict surgical outcomes. A higher preoperative SNOT-22 score would allow more postoperative improvements and a greater possibility of achieving an MCID on the SNOT-22. The present study was the first to obtain an optimal cut-off value of 42.5 for the preoperative SNOT-22 score, indicating that we could expect PAR patients with a preoperative score above 42.5 would have an approximately 6-fold higher possibility of achieving a postoperative MCID and a 21-fold higher chance of gaining postoperative improvements in SNOT-22 scores.
Theoretically, the main purpose of surgical treatment is to obtain adequate air space to enable greater nasal patency. Thus, PAR patients with nasal obstruction (i.e., the N-O group) experienced more postoperative rhinologic improvements and gained significant absolute postoperative improvements in sleep disturbance. A previous study indicated that septoplasty with or without concurrent inferior turbinoplasty during endoscopic endonasal trans-sphenoidal surgery provided notable sleep improvements on the SNOT-22. 20 Another recent study also revealed that septoplasty with or without inferior turbinate radiofrequency provided significant improvements on the Pittsburgh Sleep Quality Index. 21 These findings are consistent with those of our study in that significant improvements in sleep symptoms were noted after surgical treatment of the nasal cavities.
Smoking status was not associated with more severe symptoms in AR. 22 However, its effect on surgical outcomes is uncertain, as some consider smoking a poor prognostic factor owing to its alteration in nasal mucociliary clearance, while other studies have shown contradictory results.23-25 Compared to smokers in our study, nonsmokers demonstrated significantly greater improvements in the sleep and ear/facial domains. Hence, PAR patients in the N-O group and non-smokers showed greater improvements in the sleep subdomain in the present investigation. We propose that sleep problems among PAR patients may be attributed to anatomical obstruction and smoking-related impairments in mucociliary function. Thus, sleep symptoms can be alleviated by anatomical correction using surgical treatment.
A previous study showed that gender, age, and smoking status were not predictors of post-septoplasty functional improvements. 23 However, another study reported that gender did not influence outcome in patients receiving septoplasty or functional septorhinoplasty. 26 However, in our study, women with PAR had higher preoperative SNOT-22 scores and significantly more postoperative improvements in total SNOT-22 scores. After the adjustment for confounders, women had a 7.7-fold higher chance of absolute postoperative improvements in SNOT-22 scores at one year after surgery; this association deserves further investigation.
Some authors reported that young patients with the chief complaint of nasal obstruction experienced greater improvement from nasoseptal surgery, while others suggested otherwise.9,23 In our study, patients in the N-O group were younger; however, the correlation and regression analysis by age did not show a significant impact on postoperative improvement or MCID achievement. We hypothesized that young patients who undergo surgery might suffer more obstructive symptoms due to anatomical problems, while elderly patients have other more bothersome symptoms, such as psychological or sleep disturbances associated with dynamic problems. 9 Nevertheless, surgical treatment resulted in significant improvements in various age groups with different primary symptoms.
This study had several limitations. First, it was limited by its small sample size. Although we aimed to enroll a larger group of patients, a limited number completed the follow-up protocol. Rapid wound recovery and immediate symptom relief after surgery result in poor patient motivation to complete the postoperative follow-up. Second, a single intervention measurement using a self-assessment questionnaire is a point of concern. In the future, we will apply more subjective and objective measurements to form a hybrid intervention and reach a more definite conclusion. Third, we enrolled patients who underwent surgery that mainly targeted anatomical correction, resulting in an unavoidable imbalance in patient numbers with respect to their chief complaint. Finally, this study was conducted in a tertiary referral hospital, which may involve selection bias for disease severity. A multicenter study with a longer follow-up period and the enrollment of more patients with various non-obstructive symptoms must be conducted in the future.
In summary, septoplasty with turbinoplasty could improve the QOL and non-obstructive symptoms of PAR patients. Women with PAR and those with preoperative SNOT-22 scores > 42.5 would be candidates for surgical treatment to achieve more postoperative improvements. Non-smokers and patients with nasal obstruction as the chief complaint would gain more postoperative sleep improvement. Despite various patient characteristics, significant postoperative improvements were observed in all SNOT-22 subdomain scores. Studies with larger enrollment and a longer follow-up duration are crucial to achieving more definitive conclusions.
Footnotes
Acknowledgments
We thank research assistant Meng-Chieh Tsai, BS, for collecting the data and contacting the patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Ministry of Science and Technology (MOST 110-2314-B-182A-099).
Ethical Approval
This study has been approved by the Institutional Review Board of Chang Gung Memorial Hospital (no.104–6433A3).