
Abstract
Purpose
The relationship between ankyloglossia and speech is controversial. Our objective in the present study was to determine the most appropriate intervention and optimal timing for infants with speech articulation caused by ankyloglossia.
Patients and Methods
A total of 341 pediatric patients (aged 2 to 5 years) being referred for speech concerns due to ankyloglossia were enrolled in a randomized trial and assigned to either a surgical intervention (N = 166) or a no surgical intervention (N = 175) group. Subsequently, patients were further categorized into 3 groups according to age: 2 to < 3 years, 3 to < 4 years, and 4 to < 5 years. Measures of tongue appearance, tongue mobility, speech production, and parent and clinician intelligibility ratings were collected at preintervention (T0), 2-month postintervention (T1), 6-month postintervention (T2), and 12-month postintervention (T3).
Results
No statistically significant difference was found between surgical intervention and no surgical intervention groups for tongue appearance, tongue mobility, speech production, and intelligibility in the 2 to < 3 years age. However, there was significantly improved speech production and intelligibility in the surgical intervention group when compared to the no surgical intervention group in the 3 to < 4 and 4 to < 5 years old age.
Conclusion
Surgical intervention should not be performed too early for infants aged 2 to < 3 years with speech articulation caused by ankyloglossia, but rather watch and wait for the physiological growth of the lingual frenulum. The optimal timing range for surgical intervention is 4 to 5 years. This should provide certain significant guidance for infants with speech articulation caused by ankyloglossia.
Introduction
Ankyloglossia, or tongue-tie, refers to congenital anatomic variation which is characterized by a short or tight lingual frenulum and results in limited tongue movement. The incidence of this condition among infants varies from 2% to 10% with a male-to-female ratio of 3 to 1. 1 However, the exact etiology is unknown, with a few studies suggesting a genetic component. 2 Many studies have shown that ankyloglossia contributed to multiple dysfunctions, including newborn breast-feed difficulties, speech articulation disorder, poor oral hygiene, and various mechanical and social issues related to the inability of the tongue to protrude sufficiently. 3
Numerous studies have demonstrated that ankyloglossia has been associated with a variety of infant-feeding problems and frenotomy immediate improvement in nipple pain and breastfeeding scores.4,5 However, the correlation between ankyloglossia and speech articulation remains controversial, and defects in articulation have been one of the main reasons for infants. 6 Moreover, improvements from operative interventions have yet to be thoroughly explored with regard to ankyloglossia-related speech articulation. Srihari et al 7 conducted a retrospective chart review in 2019 and appeared that no significant improvement in speech quality following frenulectomy in children with ankyloglossia in comparison to speech quality without treatment. Conversely, many studies suggest that patients’ speech, intelligibility, and articulation were affected by restricted mobility and movement of the tongue and were improved following the procedure.8,9 Therefore, due to its insufficient and low-quality evidence with a high risk of bias prevented a definitive conclusion on the effect of surgical intervention on speech improvement in ankyloglossia patients.
More importantly, there is still huge controversy about the optimal timing of surgical intervention for patients with speech disorder caused by ankyloglossia. Some investigators have mandated withholding surgery until age 4 or more, and then offering surgery only to those with a manifest speech problem, 10 whereas others have advocated that children pronunciation is related to factors such as auditory function, language environment, intellectual development, and pronunciation. Thus, they advocate surgery should be completed at the age of 4–8. 11 It is well known that 2 to 5 years old is a critical period for the development of children’s voice system, and a short or tight lingual frenulum limits the motor tasks of the tongue, seriously affects the growth and development of the children’s language system, and inevitably causes permanent speech disorder in children. Therefore, accurate intervention measures and optimal timing of intervention are crucial for infants and young children with speech articulation caused by ankyloglossia.
Herein, the present study was to conduct a randomized trial that would adequately answer the question: What are the most appropriate intervention and optimal timing for ankyloglossia in infants with speech articulation?
Patients and Methods
Study Design and Setting
A randomized study composed of infants with ankyloglossia was designed and implemented in the Gansu Maternal and Child Health Hospital. The study was approved by the Gansu Maternal and Child Health Hospital Institutional Review Board, and informed consent was obtained from family members before the initiation of intervention. All pediatric patients (aged 2 to 5 years) being referred for speech concerns due to ankyloglossia between January 2016 and January 2019 were consecutively enrolled. Exclusion criteria included craniofacial anomalies, cleft lip, or palate; neurologically, compromised infants and all other diseases that may cause language disorders diagnosed by a speech pathologist.
Procedure
Once the presence of ankyloglossia was confirmed by a fellowship trained pediatric otolaryngologist, parents were informed of the current study and asked whether they would like to participate. After consent and enrollment, all subjects with ankyloglossia were randomly assigned to the surgical and no surgical group using a computerized random-number generator of blocks of 4 created by a statistician and implemented by a research assistant. Following this, the groups were further categorized into 3 groups according to age: 2 to < 3 years, 3 to < 4 years, and 4 to < 5 ears. All subjects underwent a further detailed examination by the surgeon to better characterize the degree of ankyloglossia. Notably, criteria of surgical intervention were Kotlow’s Classification (KC) class III and IV (free tongue movement less than 7 mm) and Bristol Tongue Assessment Tool (BTAT) scores less than 3. The method of surgical treatment was frenotomy, which was performed by the same oral and maxillofacial surgeon. However, some infants with ankyloglossia were enrolled to the no surgical intervention group. They were only observed and monitored without any treatment measures. In addition, patients were then cross-referenced to blind the interviewer and the statistician. Measures of tongue appearance, tongue mobility, speech production, and parent and clinician intelligibility ratings were collected at preintervention (T0), 2-month postintervention (T1), 6-month postintervention (T2), and 12-month postintervention (T3). All follow-up sessions were also audio-recorded.
Measures
Tongue Appearance and Tongue Mobility Assessments
Examiners graded ankyloglossia using the KC and BTAT, 12 which measure tongue mobility and tongue appearance, respectively. This study suggested KC has excellent reliability for determining the recommendation for a frenotomy, defined as appearance score lower than 7 mm with function score higher than class III. Infants with these score thresholds were defined as having significant ankyloglossia. Unfortunately, there is no documented association between this classification scheme and the clinical symptoms of ankyloglossia. Therefore, we also have added a measurement item on the appearance of the tongue, which is performed using BTAT measurements that have excellent interrater reliability. The scores for the 4 items are summed and can range from 0 to 8. Scores of 0–3 indicate more severe reduction of tongue function. And less than 3 was defined having significant ankyloglossia in the present study. All assessments are photographed and recorded.
Speech Sound Assessment
Depending on the age of the participant, either the Goldman-Fristoe Test of Articulation-2 (GFTA-2) 13 or the phonology subtest of the Diagnostic Evaluation of Articulation and Phonology (DEAP) 14 was administered to assess each participant’s speech sound production. These tools are standardized assessments for speech sound production. The DEAP provides differential diagnoses of speech disorders in children aged 3 years to 8 years 11 months. The GFTA-2 provides more accurate assessments of speech errors in patients aged 2-21 years. These have been previously validated for children and young adult with normative scores being established for males and females. All words produced for the test were transcribed using the International Phonetic Alphabet.
Intelligibility Assessment
Parent and clinician intelligibility ratings were used to measure the child’s overall ability to be understood on a 5-point Likert scale. 15 All sessions were video-recorded with an iPhone and audio-recorded with an Olympus VN741PC recorder. Assessment data were transcribed after each session. Two student speech pathologists, the chief investigator, and an assistant completed all assessments. To ensure inter-rater reliability between scorers, 20% of recordings (audio and video) were randomly selected and scored in their entirety. A high rate of consistency (>95%) was achieved between the 2 raters, with any differences being discussed and agreement reached.
Statistical Analysis
All data are analyzed by using SPSS software. Outliers were not excluded as they captured the spread of participants. The descriptive statistical method was used to evaluate the difference of therapeutic effect between the sham and frenotomy group in different age groups by analyzing the average value. Categorical data were analyzed by using X 2 analysis. The scores were analyzed by using repeated-measures analysis of variance. Computed t tests were performed for analysis of baseline demographic data. For all tests, *P < .05 was considered statistically significant.
Results
Participant characteristics for the surgical intervention and the no surgical intervention groups.
Note. N = number of participants; M = mean, SD = standard deviation.
As Figure 1 demonstrates, compared with before the intervention, both the surgical and no surgical groups demonstrated statistically significant increases in KC, BTAT, and GFTA-2 after the intervention for infants with ankyloglossia in the 2 to < 3 years age group. However, no statistically significant differences were found between surgical intervention and no surgical intervention groups after 1 year of follow-up in KC, BTAT, GFTA-2, and Likert scores (P > .05). The KC and BTAT scores in the surgical group were significantly higher than the no surgical group 2 months after the intervention (P < .05) (Figure 1A and B), but no such difference was detected in GFTA-2 and Likert scores (P > .05) (Figure 1C and D). KC, BTAT, GFTA-2, and Likert scores of children with ankyloglossia before and after the surgical vs no surgical intervention in the 2 to < 3 years age group.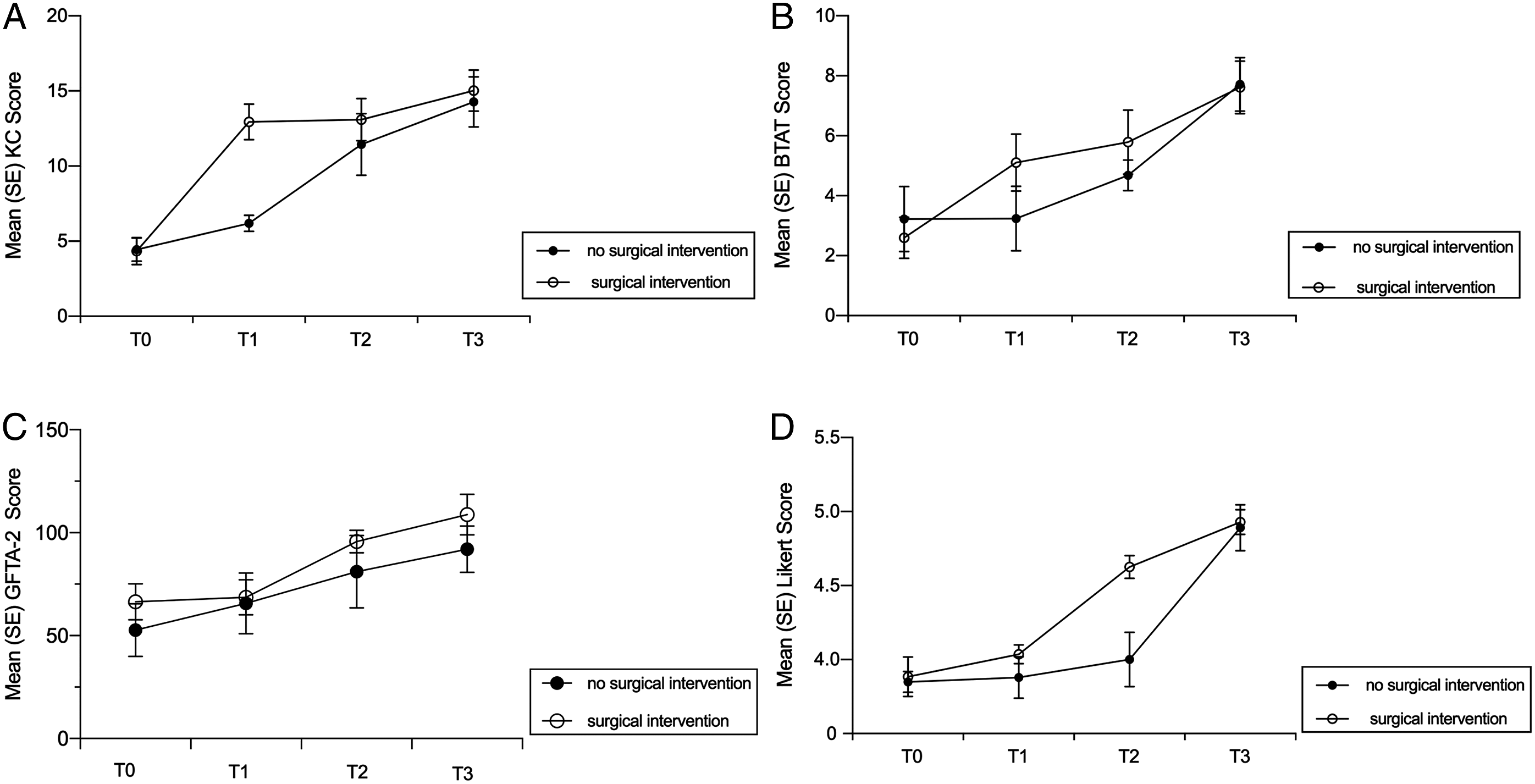
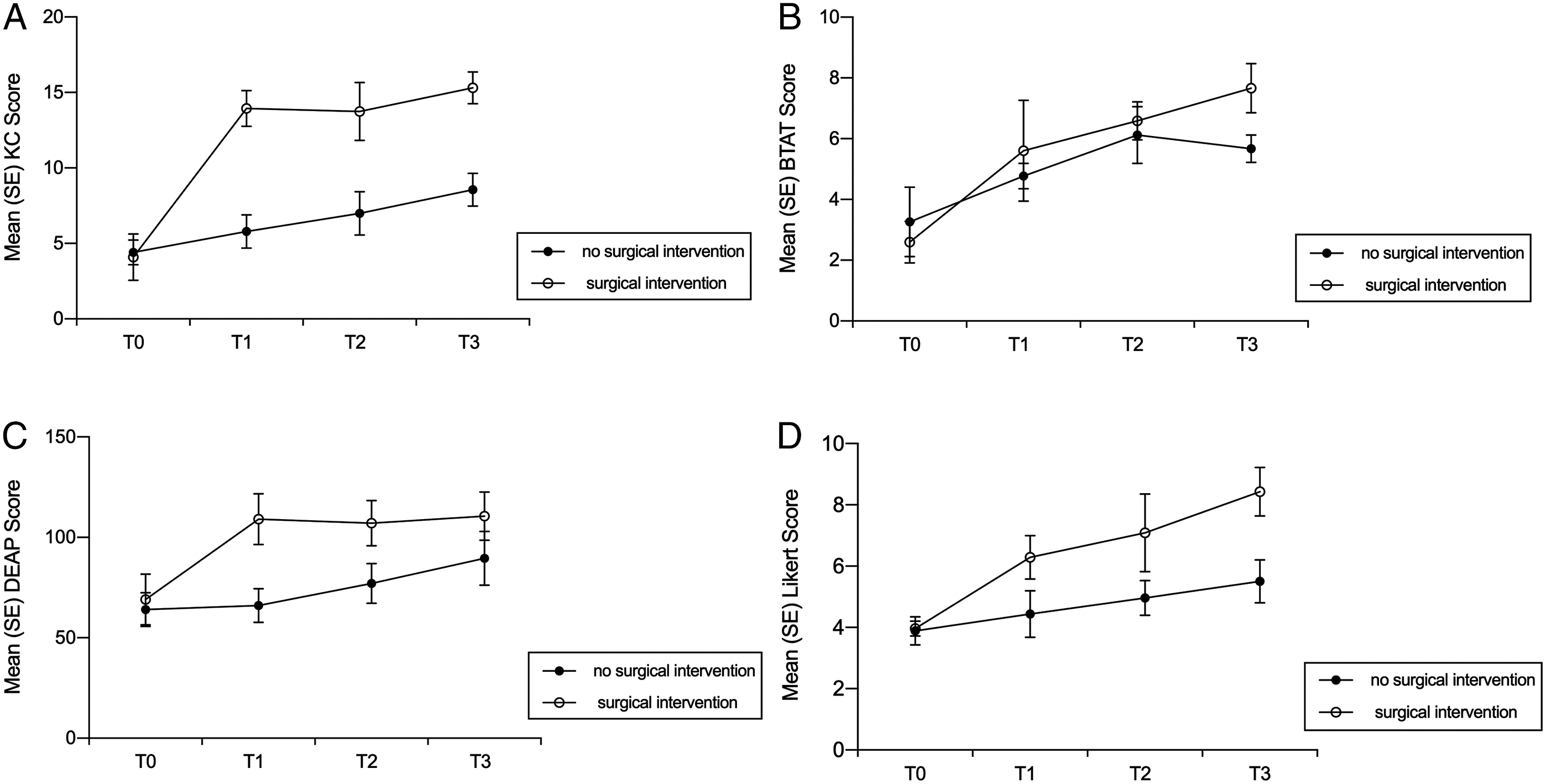
For infants with ankyloglossia in the 3 to < 4 years age groups, both 2 groups improved significantly in KC and BTAT scores after the intervention compared with before the intervention. Moreover, there was no significant difference in income between the surgical group and the no surgical group after 1 year of follow-up (P < .05) (Figure 2A and B). However, the surgical group improved significantly than the no surgical group in DEAP and Likert scores (P < .01) (Figure 2C and D). In addition, compared with the pre-intervention, only the surgical group significantly increased all scores for infants with ankyloglossia in the 4 to < 5 years age (P < .01) (Figure 3). No such changes were found in the no surgical group. The surgical group improved significantly more than the no surgical group in all scores after 1 year of follow-up (Figure 3). KC, BTAT, DEAP, and Likert scores of children with ankyloglossia before and after the surgical vs no surgical intervention in the 3 to < 4 years age group. KC, BTAT, DEAP, and Likert scores of children with ankyloglossia before and after the surgical vs no surgical intervention in the 4 to < 5 years age group.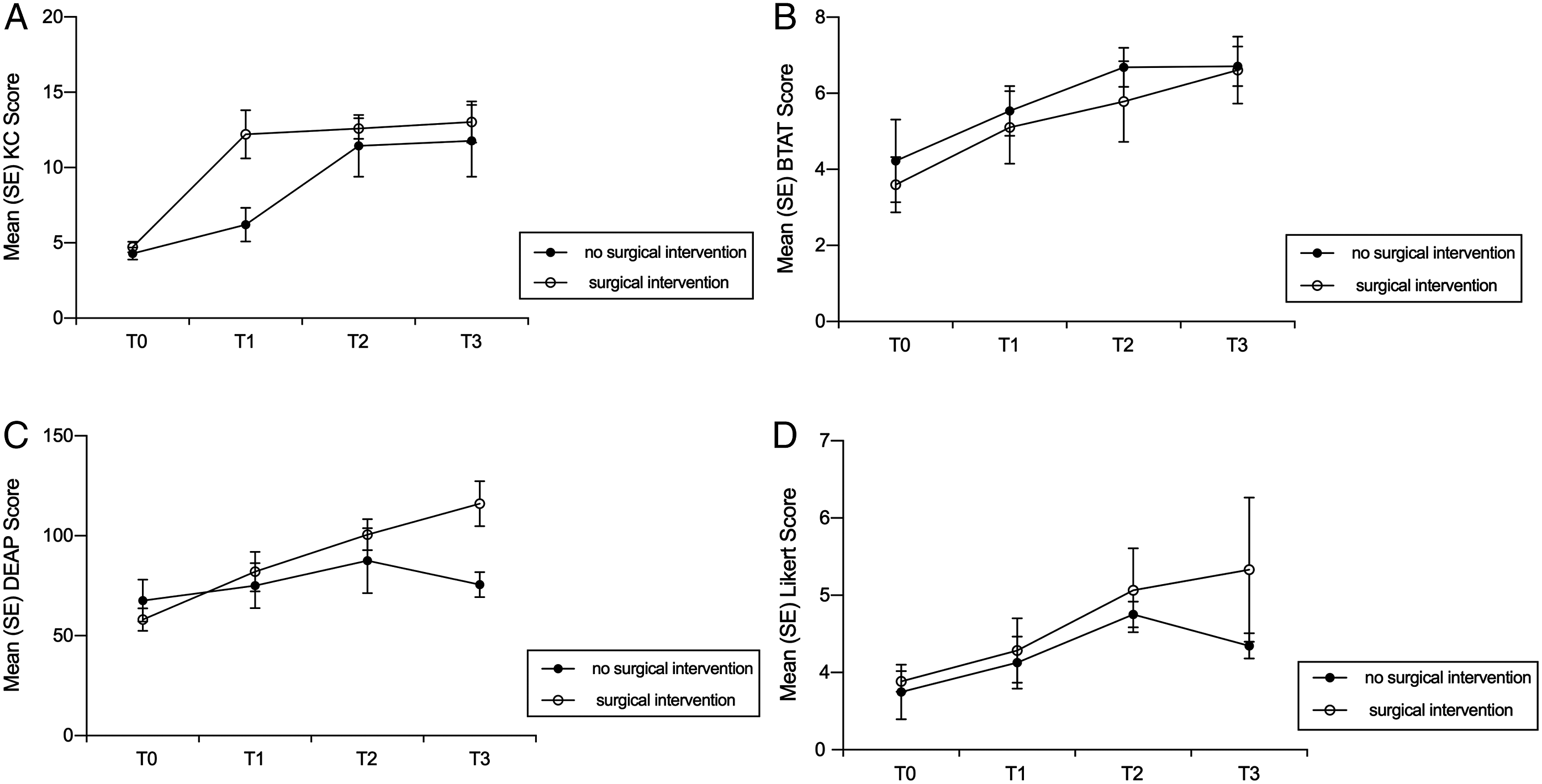
Discussion
Although the relationship between ankyloglossia and speech is controversial, speech articulation is the main complaint and therapeutic indication for children with tongue-tie. A systematic review of the relationship between ankyloglossia and speech articulation and the therapeutic efficacy of surgical interventions has demonstrated that there was no clear connection between ankyloglossia and speech problems due to lacking high-quality clinical evidence. 16 Notably, there have been opinions and differences in the treatment of ankyloglossia, especially for the intervention method and optimal timing of treatment for infants whose parents and referring healthcare providers expressed concerns about speech development. Therefore, more widely accepted uniform grading systems and well-designed clinical studies are needed.
In the current study, a total of 341 pediatric patients (aged 2 to 5 years) being referred for speech concerns due to ankyloglossia were enrolled in this study. Firstly, although no statistically significant differences were found between surgical intervention and no surgical intervention groups for tongue appearance, tongue mobility, speech production, and intelligibility in the 2 to < 3 years age, both groups significantly improved after the intervention compared with before the intervention. This is in contrast to several previous studies that the surgical group improved significantly more than the no surgical group in improved speech outcomes.7,17 A systematic review published in Pediatrics Journal 2015 mentioned some data points to the fact that there is no need for surgical treatment, since the short frenulum will likely elongate spontaneously with use and stretching with the development of jaws and the eruption of teeth. 18 Therefore, this study recommended that surgical intervention should not be performed prematurely for 2 to 3 years old infants with ankyloglossia due to the physiologic regression of the tongue-tie. Consistently, numerous reports suggested that avoiding performing resection on patients of a very young age due to the possibility of improvement with growth and the fact that the procedure can cause scarring. 19 However, there are no accurate clinical studies on the physiological growth period of the tongue frenulum so far. Although there was a study shown that the physiological growth of the lingual frenulum has completed as early as 1 year after birth, 20 in this study, infants with ankyloglossia aged 2 to 3 years developed physiological growth of the lingual frenulum during the 1-year follow-up, which may explain why there was no significant difference between the surgical and non-surgical groups in tongue appearance, tongue mobility, speech production, and intelligibility.
In addition, the results showed the surgical group was significantly higher than the non-surgical group after 1 year of follow-up in terms of improvement in speech articulation for infants with ankyloglossia in the 3 to < 4 years old. However, there was no significant difference between them in tongue appearance and tongue mobility. Notably, this result demonstrated that surgical intervention significantly improves speech articulation for 3 to 4 years old children with ankyloglossia. The results are consistent with those of Walls 21 that there were significantly improved speech outcomes designated by parents in the surgical intervention group when compared to the no surgical intervention group. Interestingly, this could be related to a slight gain in speech production training in kindergarten, because entering kindergarten after reaching the age of 3 as required by Chinese law. 22
Subsequently, in this study, compared with the pre-intervention, only the surgical group significantly increased tongue appearance, tongue mobility, speech production, and parent and clinician intelligibility ratings for infants with ankyloglossia in the 4 to < 5 years age. Importantly, the surgical group improved significantly more than the no surgical group after 1 year of follow-up. Consistently, previous studies showed that children with preoperative moderate speech and language impairment attained better speech and language outcomes after frenulectomy when compared to children without surgery. 23 However, many studies have demonstrated that surgical intervention did not have a significant positive effect on speech improvement in children with ankyloglossia.7,13,17 Notably, there were several inconsistencies in the conclusions of the included studies, which may be due to differences in study design, study subjects, the follow-up period, and the assessment methods. Moreover, the physical improvement of speech as the children aged and the lack of unified and standardized articulation evaluation methods and subjective assessment results contributed to the main source of divergence.
Notably, the primary concern in the present study was to determine the most appropriate intervention and optimal timing for infants with speech articulation caused by ankyloglossia. It follows that 4 to < 5 years old is the best time for surgical intervention, which can improve the speech articulation caused by ankyloglossia. Nevertheless, Veyssiere 24 recommended the lingual frenulum should be removed as soon as possible for infants 6 months ago, and another author affirmed that the majority of the children manage it between 12 and 15 months. 25 Because at that time the lingual frenulum is still a layer of sophisticated cell membrane in infants and newborns, frenotomy is rapid and relatively easy to accomplish in the office with local or no anesthesia and sedation. 26 Some authors advised that the process can be completed around 4 or 5 years old, because it is considered that when the first molars appear, the real chewing movements begin and the learning of a mature swallowing starts. 27 Considering the restlessness, crying, and other adverse reactions, sedation may be required in frenectomy for older children, induce sleep and general anesthesia in certain doses, and contribute to an amelioration in depression and anxiety. However, the possible side effects of sedatives on children, especially newborns, cannot be ignored in frenectomy. Recent several in vivo studies have shown that early use of sedatives can lead to permanent structural and functional changes of central nervous system. There may be intellectual disabilities, lethargy, nausea, vomiting, loss of appetite, and other symptoms, which will seriously affect the development of the brain. 28
There were several limitations to this review. It mainly included the following 3 aspects: (1) the diagnosis of ankyloglossia was limited by the lack of validated criteria or a standard test, (2) the indications for surgical treatment remain unclear, and (3) speech outcome measures lack a unified standard method, which currently remains subjective and distinct in most included studies. In addition, this study was small observational studies, which are more likely to selectively report positive results, leading to a higher risk of publication bias.
In summary, this study suggests that surgical intervention should not be performed too early for infants who aged 2 to < 3 years with speech articulation caused by ankyloglossia owing to the spontaneous growth of frenulum, and concludes that the optimal timing range for surgical intervention is 4 to 5 years old. However, convincing evidence for those seeking a surgical intervention for infants with speech articulation caused by ankyloglossia still needs to be further studied.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Nature Science Foundation of China (Grant No.51501042), Lanzhou Science and Technology Project (Grant No.2016-3-122), and Gansu Province Science and Technology Innovation Development Special Fund Project (Grant No.2018ZX-03).