
Abstract
Objective
The relationship between ankyloglossia and speech is controversial. The objective of this study was to determine the effect of tongue-tie release on speech articulation and intelligibility.
Methods
A prospective cohort study was conducted. Pediatric patients (>2 years of age) being referred for speech concerns due to ankyloglossia were assessed by a pediatric otolaryngologist, and speech articulation was formally assessed by a speech language pathologist using the Goldman-Fristoe Test of Articulation 2 (GFTA-2). Patients then underwent a tongue-tie release procedure in clinic. After 1 month, speech articulation was reassessed with GFTA-2. Audio-recordings of sessions were evaluated by independent reviewers to assess speech intelligibility before and after tongue-tie release.
Results
Twenty-five participants were included (mean age 3.7 years; 20 boys). The most common speech errors identified were phonological substitutions (80%) and gliding errors (56%). Seven children (28%) had abnormal lingual-alveolar and interdental sounds. Most speech sound errors (87.9%) were age/developmentally appropriate. GFTA-2 standard scores before and after tongue-tie release were 85.61 (SD 9.75) and 87.54 (SD 10.21), respectively, (P=.5). Mean intelligibility scores before and after tongue-tie release were 3.15 (SD .22) and 3.21 (SD .31), respectively, (P=.43).
Conclusion
The majority of children being referred for speech concerns thought to be due to ankyloglossia had age-appropriate speech errors at presentation. Ankyloglossia was not associated with isolated tongue mobility related speech articulation errors in a consistent manner, and there was no benefit of tongue-tie release in improving speech articulation or intelligibility.
Introduction
Ankyloglossia is a common congenital anomaly characterized by a short lingual frenulum that may restrict tongue mobility.1-3 Ankyloglossia has been associated with a number of functional limitations including difficulties with breastfeeding, speech articulation, oral hygiene, and psychosocial concerns.4-6 Although studies have demonstrated an association between ankyloglossia and breastfeeding issues, relations with other functional difficulties are less clear.4-7
Speech problems associated with ankyloglossia are believed to be related to articulation errors caused by limited movement of the tongue tip.8-10 Although this intuitively makes sense, all speech sounds in the English language can often be produced with minimal tongue tip mobility through compensatory mechanisms. 11 Furthermore, the lingual frenulum may physically adapt and lengthen/stretch overtime, thereby overcoming any significant functional limitations related to speech. 12 Subsequently, it is still challenging to discern whether ankyloglossia solely contributes to speech errors.
Treatment for ankyloglossia is tongue-tie release. If speech errors are caused by limited tongue mobility, the expectation is that these errors should improve following tongue-tie release. However, current evidence has been conflicting.13-16 Moreover, high-quality research is lacking as studies have been limited by retrospective design and use of subjective, non-validated measures of speech articulation (eg, parental perception).13-16 Despite the lack of evidence, many providers report that ankyloglossia is a common cause of speech problems and often recommend tongue-tie release.17-19
The purpose of this study was to assess whether ankyloglossia causes speech problems in children and to assess the effect of tongue-tie release on speech outcomes including speech articulation and intelligibility.
Methods
A prospective cohort study was conducted at a tertiary-level pediatric otolaryngology clinic in Eastern Canada. New pediatric patients (>2 years of age) being referred for speech concerns due to ankyloglossia between July 2015 and June 2017 were consecutively enrolled. Exclusion criteria included any history of other developmental delays, hearing loss, neuromuscular disorders, craniofacial disorders, learning to speak multiple languages, absence of ankyloglossia, children in active speech therapy, or lack of decision-making authority of the accompanying caregiver. Institutional review board approval was obtained prior to enrollment.
Procedure
A standard consultation was first performed by a fellowship-trained pediatric otolaryngologist. Once the presence of ankyloglossia was confirmed, parents were informed of the current study and asked whether they would like to participate. Those who agreed underwent a further detailed examination by the surgeon to better characterize the degree of ankyloglossia according to the modified lingual frenulum function assessment form (Supplementary Appendix A).20,21 This was done to ensure that the degree of ankyloglossia was assessed to be moderate to severe in a consistent manner (ie, mild cases of ankyloglossia were excluded). After clinical assessment, participants were assessed by a speech language pathologist using the Goldman-Fristoe Test of Articulation-2 (GFTA-2). All sessions were audio-recorded. Following the GFTA-2 assessment, parents were offered the choice of a tongue-tie release procedure in clinic. After applying topical local anesthetic, a primary release procedure was performed with the aid of a grooved director and sterile iris scissors in clinic.
All participants were then seen back in the pediatric otolaryngology clinic at 1 month for follow-up. The same surgeon assessed the oral cavity to ensure that there was good healing with no significant scarring or re-fusion of the lingual frenulum. The GFTA-2 test was then repeated by the speech language pathologist to assess post-procedure speech articulation. All follow-up sessions were also audio-recorded.
Power analysis was performed with the GFTA-2 (primary outcome measure). A moderate expected effect size with 80% power showed that 20 participants were required to detect a clinically meaningful change on speech assessment.
Measures
Goldman-Fristoe Test of Articulation-2 (GFTA-2)
The primary speech outcome of the study was the GFTA-2 Words-in-Sounds test. The GFTA-2 is one of the most well established and commonly used speech articulation tests in North America. It has been previously validated for children and young adults, between ages 2-21 years, with normative scores being established for males and females. 22 The GFTA-2 provides information about a child’s articulation ability by sampling both spontaneous and imitative sound production. During the test, participants respond to picture plates and verbal cues from the speech language pathologist with single-word answers that demonstrate common speech sounds in the English language. All words produced for the test were transcribed using the International Phonetic Alphabet (Supplementary Appendix B).
Speech Intelligibility Assessment
Speech intelligibility was assessed using the scaling method previously described by Kent and colleagues. 23 Naïve listeners (n = 5) were asked to rate children’s speech intelligibility using the audio samples that were previously recorded during the speech assessment on a numeric scale ranging from 1 to 10 (1 being totally unintelligible and 10 being completely intelligible). All raters listened to speech samples at random order multiple times to assess for intra-rater reliability.
Data Analysis
Data was analyzed using the SPSS Statistics for Windows Version 17.0 (Chicago, Illinois). Parametric tests were used as the data was normally distributed. Descriptive data included mean, standard deviation (SD), and range. Inter-rater reliability was assessed using Kappa statistics. Due to the exploratory nature of this study, a convenience sample size was used.
Results
Participants
Twenty-eight consecutive patients met inclusion criteria and were enrolled into the study. Two children did not show up for their follow-up appointment, and one participant’s audio-recording was not useable due to technical reasons. Therefore, a total of 25 participants were included in the final analysis.
The mean participant age was 44.4 months (SD = .4; range 24–87 months), and the majority of participants were male (n = 20; 80%). All presenting parents and referring health care providers had concerns about the child’s speech development, which they believed were related to the child’s tongue-tie. Three parents also expressed specific concerns about limited vocabulary and one parent voiced concerns with respect to difficulties with eating.
All children underwent an uneventful tongue-tie release procedure in clinic. No post-procedure complications were noted. Subjectively, 12 parents (48%) reported some improvement in their child’s speech at the follow-up 1-month visit. The remaining parents were unsure or reported no noticeable changes in speech development.
Goldman-Fristoe Test of Articulation-2
Goldman-Fristoe Test of Articulation-2 Results.
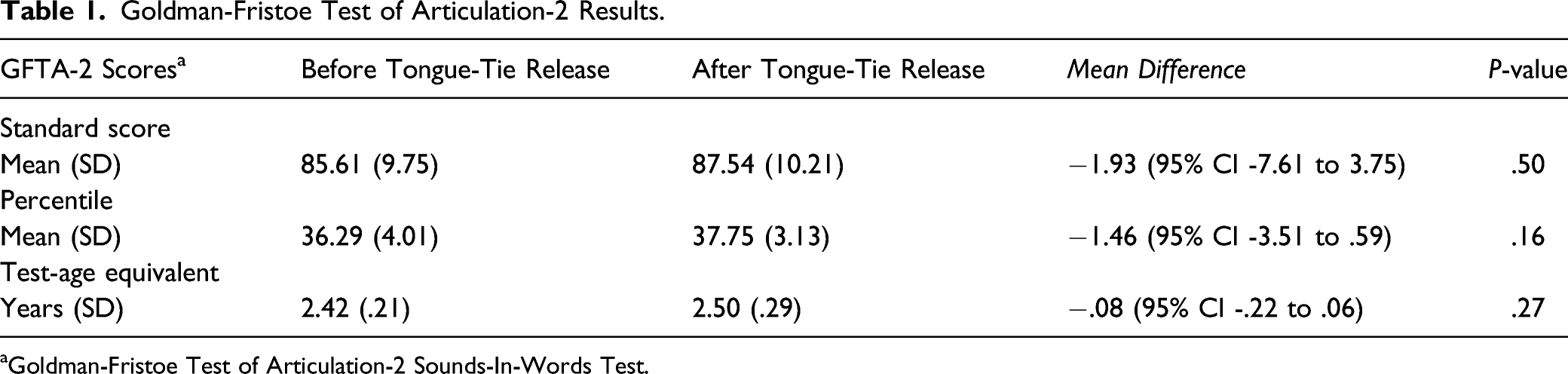
aGoldman-Fristoe Test of Articulation-2 Sounds-In-Words Test.
Five (20%) participants scored at or above the 50th percentile for their age and gender group before tongue-tie release while six children (24%) scored at or above the 50th percentile for their age and gender group after tongue-tie release. The overall test-age equivalent score was considered to be slightly lower than expected both before and after tongue-tie release.
With respect to specific speech sound errors, no consistent pattern was observed before or after tongue-tie release. Multiple speech sound error types (eg, substitutions, deletions, additions, omissions, distortions), error distribution (eg, altering position of sound in word), and error patterns (eg, phonological errors) were noted on initial presentation and several children presented with more than one form of speech sound error. The most common speech sound errors were phonological substitutions (n = 20; eg, dus for bus), gliding errors (n = 14; eg,/f/for/θ/), and initial/k/,/s/, and/h/substitutions (n = 8). Seven (28%) children had abnormal lingual-alveolar (t, d) and interdental sounds (voiced and voiceless/th/), along with other tongue mobility related sound errors (/s/,/z/,/l/and/r/). However, they were considered age appropriate in terms of development for all children (eg,/l/sound may not develop till 5–7 years of age). Moreover, five of these children also had other identified speech sound errors. Some younger children (n = 4) were not stimulable for certain sounds and intelligibility in connected speech was reduced (n = 9). Overall, most speech sound errors (87.9%) were considered to be developmentally appropriate.
Speech Intelligibility Assessment
The mean intelligibility score across all children was 3.15 (SD = .22; range 1.8–6.9) before tongue-tie release and 3.21 (SD = .31; range 1.9–7.3) after tongue-tie release. No significant difference in speech intelligibility was noted (t = .79, P = .43; mean difference −.06, 95% CI -.21 to .09). Intra-rater assessment showed high agreeability (>85%) and inter-rater reliability was found to be substantial (Kappa coefficient = .82). 24
Discussion
The belief that tongue-tie can cause speech problems is long-standing. Yet, high-quality empirical evidence is lacking.5,6 In the current study, we enrolled children with ankyloglossia whose parents and referring healthcare providers expressed concerns about speech development, which was specifically attributed to the child’s tongue-tie. Overall, no significant improvements were noted in speech articulation or intelligibility after tongue-tie release. This is in contrast to several previous studies that concluded that tongue-tie release procedures were associated with improved speech outcomes in some patients.14,15 However, to our knowledge, none of the previous studies assessed specific speech sounds as an outcome measure. Most studies reported improvements in terms of subjective outcomes, such as parental and caregiver perceptions.5,15 Even in studies that employed speech language pathologists, the measured outcomes did not ascertain specific types of misarticulations that can be attributed to sounds related to tongue-tip immobility. For instance, Messner and Lalakea reported that 9 of 15 patients demonstrated “improvement” in speech after tongue-tie release. 14 Yet, their assessment did not involve standardized speech samples and specific articulation errors were not reported.
In our study, all children were assessed by a licensed speech language pathologist with a standardized speech sample before and after tongue-tie release to objectively assess speech articulation. To our knowledge, this is the first study to report specific speech sound errors in children presenting with ankyloglossia using a validated speech sound articulation test to assess the effects of tongue-tie release. The results showed that many children had speech sound errors that were considered age-appropriate on presentation. Furthermore, many speech sound and articulation errors were sounds not typically caused by tongue tip immobility. Theoretically, speech errors secondary to ankyloglossia are caused by limited anterior tongue (or tongue tip) movement. If this association were true, one would expect lingual-alveolar, interdental, and other anterior tongue mobility related sounds to be predominantly altered, which should improve after tongue-tie release. However, our findings were not consistent with this supposition. The results from this study demonstrated that the majority of children being referred for tongue-tie release had age-appropriate speech. In fact, most speech sound errors (87.9%) were found to be age-appropriate phonological substitutions that parents and referring providers thought were being caused by ankyloglossia. Given these findings, it is not surprising that there was no significant change demonstrated in speech articulation or intelligibility following tongue-tie release. Therefore, it is important for healthcare providers to understand that many different types of speech errors (eg, articulation disorders, dysfluency, phonological disorders, voice disorders) can exist, and some sounds that necessitate maximal tongue tip extension (eg,/l/sounds) are not expected to develop until later in childhood.
The results in this study showed that many children with ankyloglossia did not have the specific misarticulations that would result from limited tongue movement. This is in keeping with the notion that lingual restriction should not significantly affect speech when considering the type of sounds that require tongue tip movement. Specifically, lingual-alveolar sounds (d, t, n) can be produced with very minute tongue elevation, while/s/and/z/sounds can also be produced with little distortion even when the tongue tip is unable to fully elevate. 11 That is, as long as the tongue tip can reach the back of the central incisors, all of these sounds can easily be produced. The/l/sound requires the most amount of tongue movement towards the back of the maxillary alveolar ridge; yet, even this sound can be produced with the tongue tip down and the dorsum of the tongue up against the alveolar ridge. 11 The/r/sound can also be produced with the tongue tip down, as long as the posterior tongue is elevated on both sides. Taken together, all of these sounds can essentially be produced without much difficulty, even when significant tongue tip restriction is present. Therefore, it does not make sense that ankyloglossia would physiologically cause speech misarticulations.
Almost half of parents reported that they noticed an improvement in their child’s speech following tongue-tie release, despite no objective improvement being demonstrated. Similar results have been reported in previous studies assessing speech outcomes with parental perceptions post-tongue-tie release. 15 However, when speech intelligibility was assessed with blinded naïve listeners, no significant differences were noted. This emphasizes the importance of using validated outcome measures with standard speech samples when assessing speech outcomes to reduce placebo effect or treatment bias.
As mentioned above, some studies have reported improvements in speech after tongue-tie release.13-15 However, in many studies the timing of the post-ankyloglossia release speech assessment was not consistent and/or too long. In one study, several months passed between the pre- and post-frenotomy speech assessments. 14 Although many participants were noted to show speech improvement, normal development may have been the reason for this finding. In our study, the second speech assessment was performed at 1-month post-treatment. The rationale for this timeline was to allow for adequate healing and recovery from the frenotomy procedure and also to allow the child to get accustomed to speaking at home with family and peers. At the same time, follow-up testing at a later date may have confounded the results as children may have demonstrated normal development in speech, especially at a young age.
There are limitations in this study. First limitation is the relatively small sample size. However, it should be noted that our sample size analysis showed that the number of participants was adequate. Another limitation is that the GFTA-2 was designed to test single-words in series as opposed to connected speech. It is important to keep in mind however, that some younger children being referred for speech concerns secondary to ankyloglossia have not yet developed fully connected speech. Furthermore, we had blinded listeners assess speech intelligibility of participants to partially account for this limitation. Another limitation is that certain institutions do not routinely perform tongue-tie release without general anesthesia in older children. However, our experience has been that most older children do tolerate this procedure in our clinic with topical/local anesthetic. Hence, our routine practice is reflected in this study which may not be generalizable. Finally, although this study did not demonstrate an overall benefit of tongue-tie release for speech outcomes, it is still unclear whether there may be a benefit of tongue-tie release in a subset of children with alveolar-dental or lingual speech issues that persist past developmentally appropriate age. As well, it is unclear whether earlier frenotomy would have made the participants’ speech and language development different than what was noted on presentation. Therefore, future studies should assess children who had earlier vs later tongue-tie release procedure.
Supplemental Material
sj-pdf-1-ear-10.1177_01455613211064045 – Supplemental Material for The Effect of Tongue-Tie Release on Speech Articulation and Intelligibility
Supplemental Material, sj-pdf-1-ear-10.1177_01455613211064045 for The Effect of Tongue-Tie Release on Speech Articulation and Intelligibility by Jonathan Melong, Michael Bezuhly and Paul Hong in Ear, Nose & Throat Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.