
Abstract
A thyroglossal duct cyst (TGDC) is the most common congenital anterior neck mass. It can develop from residual tissue not degenerated during development and is mainly diagnosed in pediatric patients. However, a TGDC is sometimes diagnosed for the first time in adult patients. A TGDC is mainly caused by repeated infections of the duct and there might be no specific symptoms. A TGDC can occur anywhere from the floor of the mouth to the thyroid but is most often found at the infrahyoid level. Over the past 10 years, there has been no report of a TGDC in the suprasternal region among TGDCs in unusual locations. This paper describes one case of a suprasternal TGDC with a review of the literature on this topic.
Introduction
A thyroglossal duct cyst (TGDC) refers to the formation of a cyst-type tumor when residual thyroid tissue remains from the root of the tongue to the anterior subhyoid bone of the upper neck during the process of thyroid gland descent before birth.1-3 The thyroid gland descends from the foramen cecum into the pretracheal space during the six weeks after fertilization. The descending and formed thyroglossal duct degenerates during the second month of pregnancy. At this time, a TGDC can occur in various locations such as the intralingual, the floor of the mouth, suprahyoid, intralaryngeal, intrathyroidal, and suprasternal areas. Over the past 10 years, there has been no report of a TGDC in the suprasternal region among TGDCs in unusual locations. This paper describes one case of a suprasternal TGDC and presents a review of the literature on this topic.
Case Report
A 23-year-old female presented with the sudden onset of a left neck palpable mass that had started three days previously. She did not complain of any other symptoms. She was diagnosed with a cystic mass between the left thyroid lobe and the common carotid artery by neck ultrasonography and computed tomography (CT) (Figure 1). After aspirating about 24 cc using a syringe, the swelling disappeared. Considering the radiologic examination results and the location of the tumor, it was thought to be a thymic cyst or bronchogenic cyst. The left recurrent laryngeal nerve was close, and the cyst size was reduced by aspiration. Thus, observation was recommended at first. Neck ultrasonography (A) and computed tomography (B) showing a huge cystic mass between the left thyroid lobe and the common carotid artery.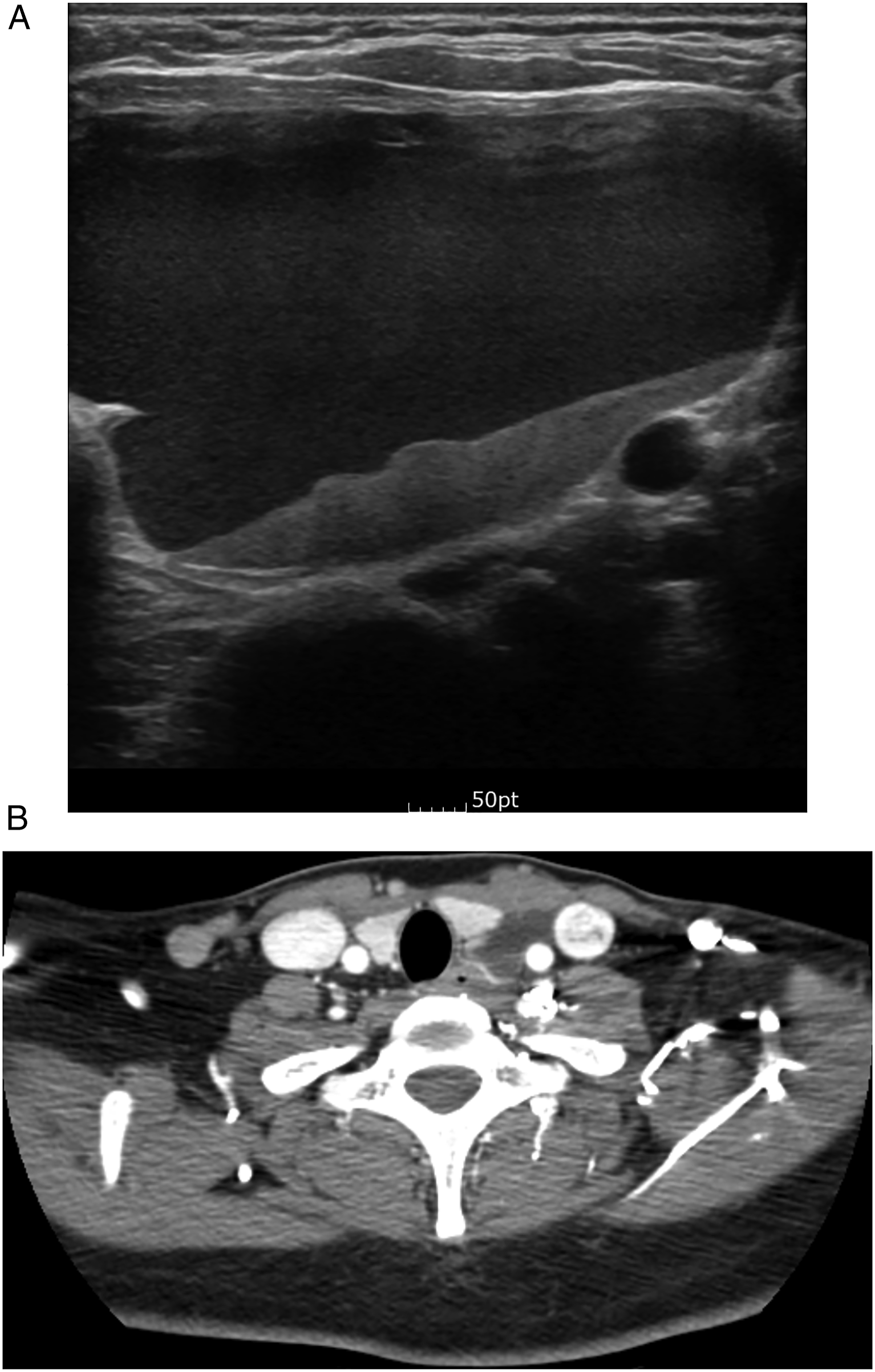
However, the swelling continued for six months and the patient revisited for surgery due to chest tightness when lying down. Neck cyst resection was performed under general anesthesia. In the operating field, there was a large cystic mass ranging from the upper thyroid pole to the sternum level. The cystic mass was completely removed while preserving the left recurrent laryngeal nerve (Figure 2). Intraoperative photos. (A) The cyst (asterisk) is closely attached to the recurrent laryngeal nerve (arrow). It was removed without nerve damage (B).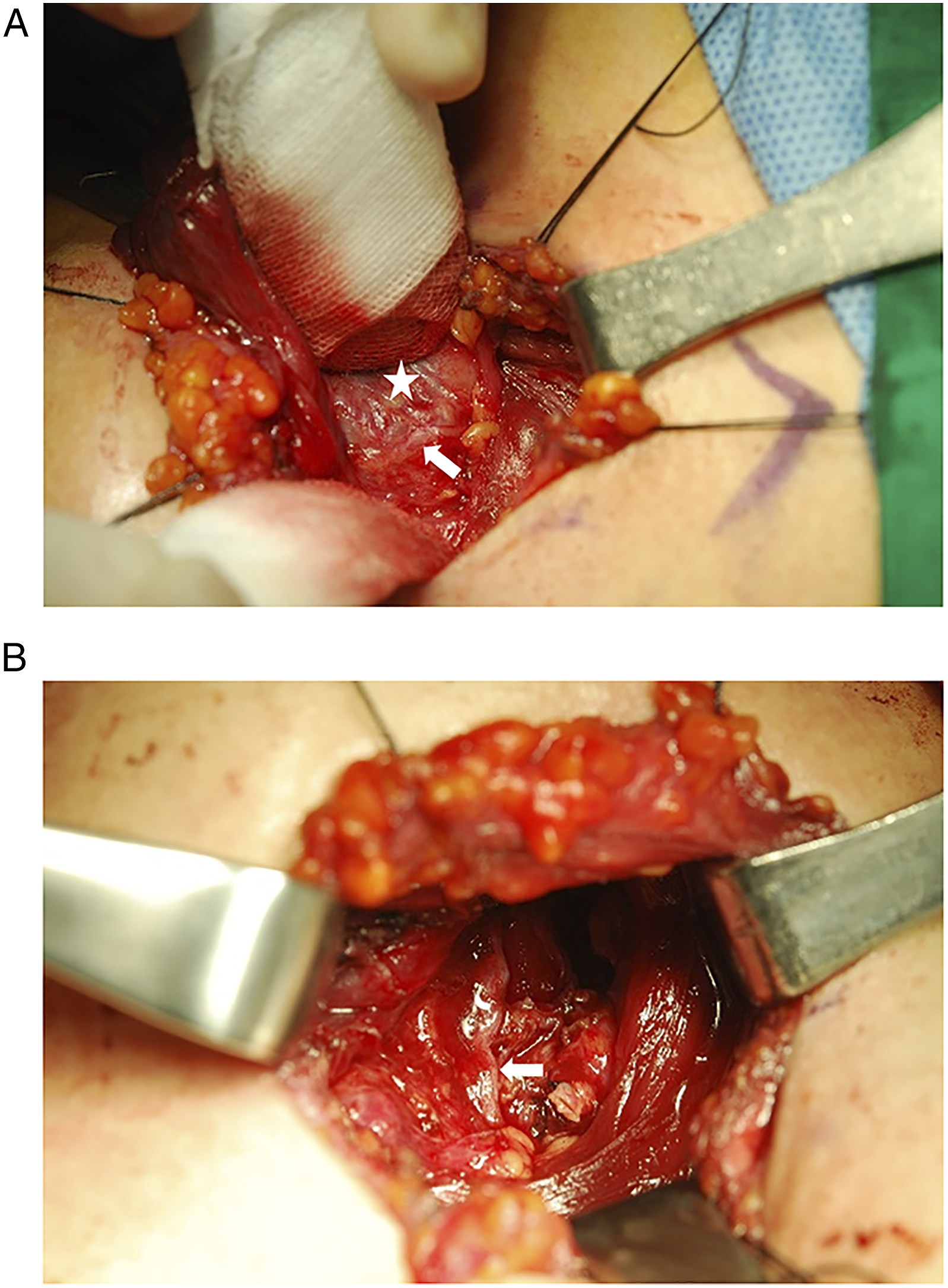
The histological examination confirmed a TGDC. Observation was decided without additional treatment such as a Sistrunk operation. She remains without problems or recurrences 17 months after surgery.
Discussion
A TGDC is the most common congenital mass occurring on the central portion of the neck in adults. 4 At the end of the third week of gestation, the thyroid develops from the second bronchial arch. The early thyroid gland travels for four weeks from the origin of the foramen cecum to the anterior to the pharynx. From the eighth week to the tenth week after gestation, the tract usually collapses and degenerates. Thus, remnants of the epithelial tract wall eventually disappear. However, if this duct persists after birth and forms a cyst due to repeated local infections or inflammation, secretions from the epithelial lining may be deposited.5-7
Thyroglossal duct cysts commonly occur below the level of the hyoid bone (85%). They can also be detected from the region of migration of the primitive thyroid during embryogenesis, the foramen cecum at the base of the tongue to the level of the suprasternal notch. 7 Thyroglossal duct cysts develop in four general locations, the intralingual (2.1%), suprahyoid (24.1%), thyrohyoid (60.9%), and suprasternal areas (12.9%).8,9 However, there has been no report of a TGDC in the suprasternal region, as occurred in our patient.
Thyroglossal duct cysts are generally found adjacent to the midline, near the hyoid, presenting as a painless mass. In some cases, they can present as swelling and tenderness due to an infection.9,10 However, symptoms vary depending upon where the TGDC is, and include dysphagia, airway obstruction, and obstructive sleep apnea. 11 In the present case, the patient manifested chest tightness when lying down.
Computed tomography generally shows a TGDC as a smooth, thin-walled hypoattenuating mass. On magnetic resonance imaging, the lesion has a high signal on T2-weighted images and a low-to-intermediate signal on T1-weighted images depending upon its protein content. 12 Ultrasonography can be a good diagnostic modality in pediatric patients. Thyroglossal duct cyst shows a well-defined anechoic to hypoechoic structure with posterior through transmission.
When performing the differential diagnosis of head and neck tumors, the first thing to consider is the location of the tumor. There are some mimics, including branchial cleft cysts, dermoid and epidermoid cysts, laryngocele, thymic cysts, lymphatic malformation, and necrotic lymph nodes. 12 The histological findings are the most accurate clues for diagnosing TGDCs, which are known to have walls composed of alternating non-keratinizing stratified squamous epithelium and respiratory epithelium. 5
The treatment choices for a TGDC include the Sistrunk procedure because the recurrence rates of TGDCs vary from 8% to 40% and about 1% of TGDCs become malignant.13,14 However, there are some reports about TGDCs occurring in unusual locations.5,6,10,15 If there is no duct, only excision of the cystic mass is performed. Previous studies suggested that only periodic follow-ups are sufficient.5,6,10,15 When considering the location of the tumor and imaging characteristics of the tumor before surgery, some cystic tumors including a TGDC can be considered. No thyroglossal duct tract was found during surgery. Thus, solitary mass excision was performed. Although the histological findings indicated a TGDC, they did not suggest possible primary carcinoma. Thus, we decided not to perform any additional treatment. We performed regular follow-ups to detect recurrence or any other symptoms. In the present case, there was no evidence to suggest that the suprasternal mass could be TGDC in the future.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.