
Abstract
Lipoma is the most common soft tissue benign tumor in the body. It can occur in the head and neck area as well. Fibrolipoma is a variant of lipoma that contains fibrous tissue. Fibrolipomas of the head and neck are relatively rare, and their presentation depends largely on their size and location; some slowly growing tumors might go unnoticed until they reach significant size and become symptomatic. Here, we report a case of 64-year-old male who presented with large pedunculated oropharyngeal fibrolipoma that originated from the posterior oropharyngeal wall and extended downward into the postcricoid area and cervical esophagus. It was excised transorally using rigid endoscope, and ACE Harmonic scalpel was utilized to excise this 16.7 cm long mass. The postoperative pain was minimal, the surgical site showed complete healing, and oral diet was resumed easily in 5 days.
Introduction
Lipoma and its variants are the most common benign soft tissue tumors in the body, and about 17% of the lipomas occur in the head and neck area. 1 A lipoma is composed of lobules of mature adipocytes. Lipoma variants are designated according to their mesenchymal elements, being fibrous tissue in the case of fibrolipoma. 2 Fibrolipomas of the head and neck are relatively rare, and they can occur in different sites, such as the aerodigestive tract, nose, eyelids, and postauricular region, among others.3-5
We report a case of a large pedunculated oropharyngeal fibrolipoma that was excised through a transoral endoscopic approach.
Case Report
A 64-year-old gentleman was admitted to the Internal Medicine Department at Prince Hamza Teaching Hospital complaining of recurrent strokes during the previous 2 months. His past medical history was unremarkable except for hypertension. Upon admission, he complained of decreased oral intake, dysphagia, and episodic dyspnea attacks, especially at supine position. His son reported the protrusion of “tongue-like” fleshy mass outside his mouth after episodes of vomiting or bouts of coughing. When this occurred, it caused labored breathing that was relieved by reswallowing the mass in a special position.
After consulting the Otorhinolaryngology, Head, and Neck Surgery department in the hospital, the patient’s general activity appeared normal with no respiratory distress. Examination of the oral cavity and oropharynx did not show any abnormal mass. No palpable lymph nodes or masses were detected after neck examination. However, flexible naso-pharyngo-laryngoscopy showed a seemingly pedunculated, mucosally covered mass that originated from the posterior oropharyngeal wall and extended downward into the postcricoid area and cervical esophagus. The distal end of the mass could not be visualized (Figure 1A). A flexible esophagoscopy was then performed, which showed that the mass was long and pedunculated; its only attachment was to the lower oropharynx. Computed Tomography (CT) scan showed a large heterogenous lesion in the upper esophagus that extended down to the lower esophagus and caused asymmetrical irregular narrowing of the esophageal lumen. The mass showed some heterogenous enhancement with intravenous contrast (Figure 1B and 1C). A) Preoperative flexible naso-pharyngo-laryngoscopy with obvious origin of the mass. B) The distal end of the fibrolipoma in the esophagus is shown. C) Computed Tomography (CT) scan showing the origin of the mass from the posterior oropharyngeal wall. D) Postoperative examination with completely healed site of surgery. Nasogastric (NG) tube is in place.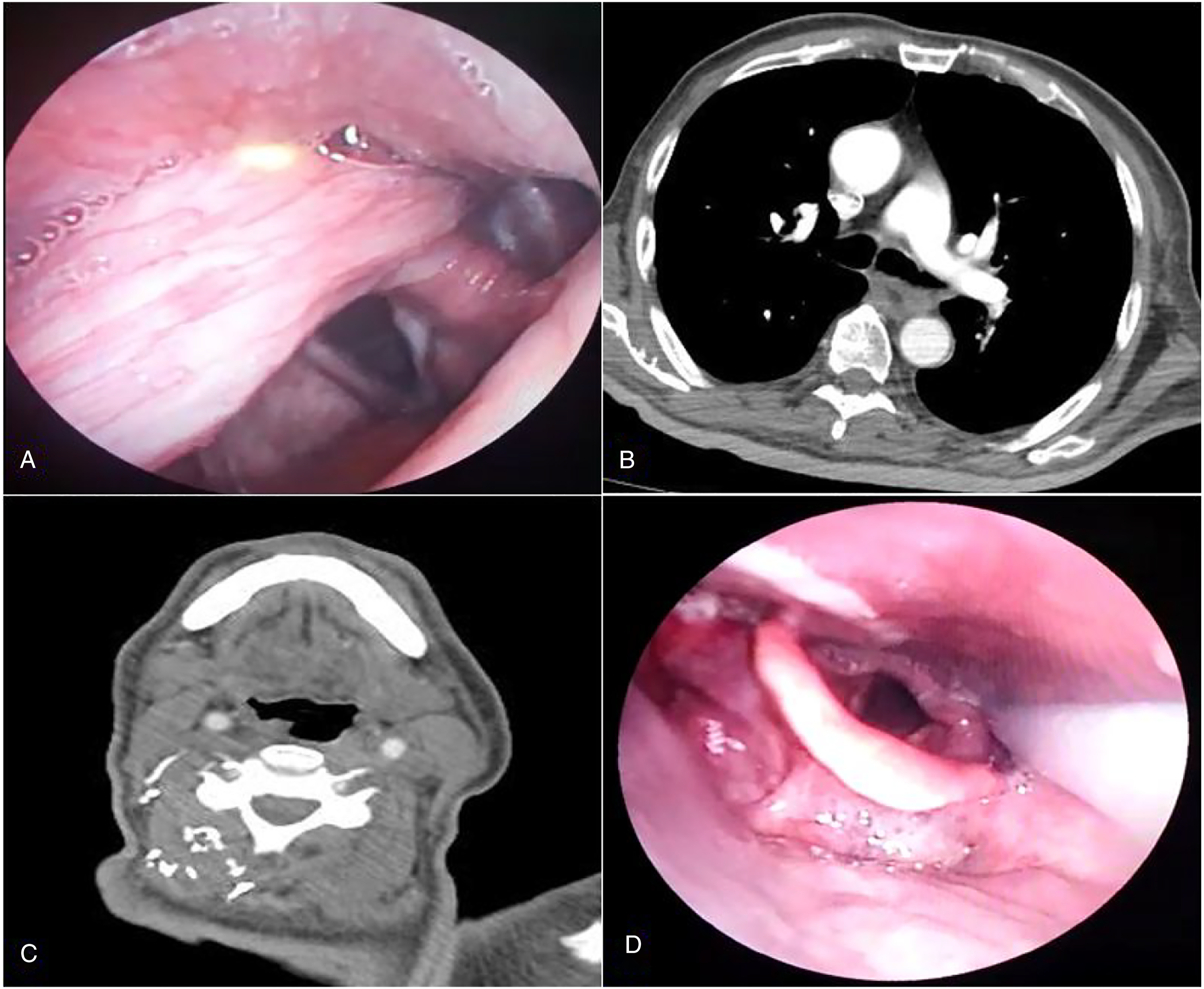
After an informed consent was obtained from the patient for transoral excision, he underwent endotracheal intubation under general anesthesia. Boyle-Davis mouth gag was inserted into the mouth, and it was fixed in neck extension position using a Drafin's bipod metallic stand. Hopkins rod endoscopes 0 and 30 degrees were used to visualize the aforementioned mass. The origin of the mass was identified in the posterior oropharyngeal wall (Figure 2A and 2B), and the distal intra-esophageal portion of the mass was pulled up easily and the entire mass was brought into the oral cavity and pharynx. ACE Harmonic scalpel was then used to excise this attachment site under direct endoscopic visualization (Figure 2C). Careful examination was done after each bite until the whole mass was excised, and no bleeding nor residual tumor could be identified at the bed site. A nasogastric (NG) tube was inserted and fixed in place and was kept for 5 days. A flexible naso-pharyngo-laryngoscopy was performed on day 5 after the surgery, and it showed a nicely healing surgical site (Figure 1D). Postoperative pain was minimal and was managed by occasional intravenous paracetamol. A) The distal end of the mass was pulled out the oral cavity before resection. B) Intraoperative endoscopic view of the stalk of the mass (arrowhead) attaching to the posterior pharyngeal wall. C) Intraoperative endoscopic view of the stalk while being resected by the Harmonic scalpel, arrow refers to the scalpel blade. D) Postoperative resected mass.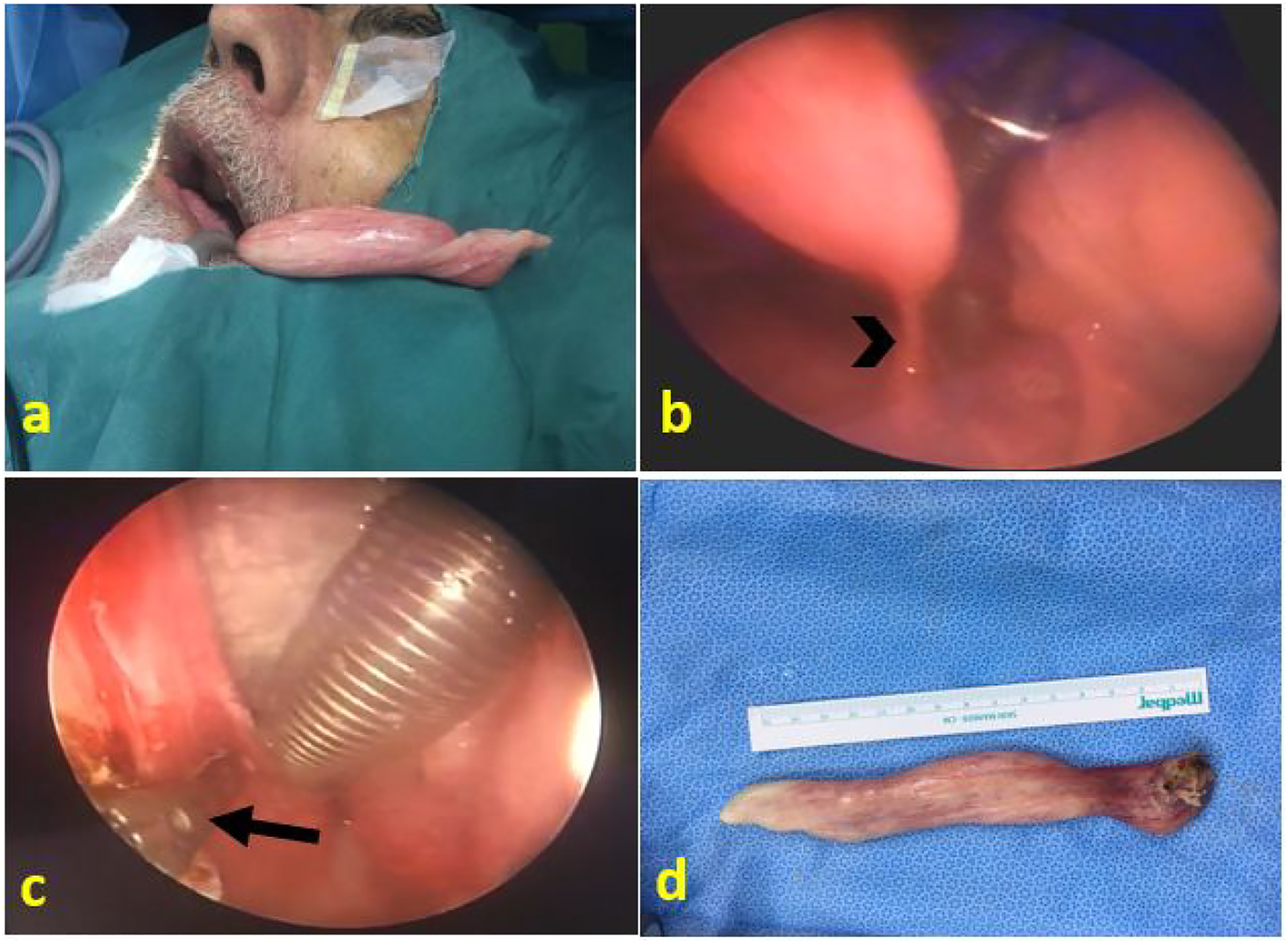
The excised mass was soft to rubbery in consistency, about 16.7 cm in length, and between 2 and 2.5 cm in cross section (Figure 2D). The microscopic histopathologic sections showed unremarkable thin stratified squamous epithelial lining with focal parakeratosis. The underlying stroma contained mature adipose tissue, fibrous tissue, and dilated blood vessels. There was no evidence of malignancy. The above findings were consistent with a fibrolipoma.
The patient was examined 2 weeks postoperatively, and he had no dysphagia, dyspnea, nor residual mass. Unfortunately, the patient had another stroke about 6 weeks later, developed urosepsis and died.
Ethical approval to report this case was obtained from the IRB committee at Hashemite University (Approval code: 11/12/2019/2020).
Discussion
The etiology of lipoma is uncertain. It varies from the differentiation of multipotent mesenchymal cells, fat tissue, or metaplasia of a pre-existing lipoma. 6 Lipoma has been associated with endocrine imbalances, such as multiple endocrine neoplasia type 1 (MEN1) and adrenal lipomas with endocrine abnormalities, and its malignant degeneration is extremely infrequent.7-9 Fibrolipoma is a benign lesion classified by the World Health Organization as a histologic variant of lipoma. In the past, it was considered as hamartoma. 10 Fibrolipomas do not exhibit specific age or sex predilection and they can even occur in children. 11 Oropharyngeal fibrolipoma usually occurs in elderly adults. However, they can present in children.11,12
Thorough clinical and imaging evaluation of any pharyngeal tumor is crucial to determine its extent and to plan appropriate treatment. Upper aerodigestive endoscopy as well as imaging studies is of extreme importance. 9 In our case, the CT scan showed upper esophageal mass that was followed by upper endoscopy, both of which showed the features and the length of the mass. Furthermore, upper endoscopy identified its only attachment at the pharyngeal level, which was helpful in management planning.
Because of the potential prolapse into the esophagus or the trachea, patients with oropharyngeal lipomas may be either asymptomatic or experience dysphagia, foreign body sensation, changes in quality of voice, or sudden transient episodes of dyspnea. Although the more severe symptoms might be mistaken for cardiopulmonary disorders, pharyngeal examination is indicated to exclude local pathology. 13 Previous cases reported the presence of fibrolipomas as a mass protruding from the mouth.14,15 In our case, mixed symptoms were present; such as dysphagia, transient dyspnea, and most notably a tongue-like fleshy mass that protruded outside his mouth after episodes of vomiting or bouts of coughing. Such an unusual and rather dramatic occurrence should alert the clinician to a potential pedunculated upper aerodigestive tract lesion. Malignant fatty tumors, liposarcomas, are thought to arise de novo, but malignant degeneration of lipomas has been reported rarely. This is particularly uncommon in some head and neck areas like the pharynx, cheek, and parapharyngeal space. 16
Aerodigestive masses have special risk to general anesthesia and intubation in some cases. Although most cases are straightforward, some cases are challenging and might need tracheostomy to secure the airway, and the patient can help the anesthetist in some other cases.17,18 Despite the recurrent transient episodes of positional dyspnea in our case, flexible laryngoscopy and upper endoscopy assessment of the aerodigestive tract precluded the need for tracheostomy. Furthermore, the anesthesia team felt comfortable to intubate the patient in routine way, but with caution.
Although external cervical approach (e.g., lateral pharyngotomy) was once the treatment of choice of pharyngeal tumors, recent technological advances have opened the door to other approaches. 19 Although pharyngeal location can be challenging in many cases, transoral access is a natural tract and has been utilized recently to remove pharyngeal tumors with much less complications, similar to the case presented here. 20 Using endoscopes has simplified the resection of many tumors that needed external approaches in the past with their potential morbidity. 21
Multiple resection techniques have been used to remove pharyngeal masses transorally. These include cold dissection and resection, monopolar resection, mechanical stapler Endo Gia Universal, and laser excision. 22 The Harmonic scalpel has been used rarely for such lesions. 23
Many recent advanced tools are being implemented nowadays in different surgical procedures. These are progressively used in head and neck operations. Ultrasonic scalpel instruments transfer the vibrating mechanical energy to tissues, leading to hydrogen bond breakage and protein denaturation at relatively low pressure, resulting in coagulation and cutting properties. 24 Their use in common pharyngeal procedures (e.g., tonsillectomy, base of tongue reduction sleep surgery) has been promising, and has resulted in less postoperative pain compared to electrocautery.25,26 Compared to monopolar cautery, ultrasonic scalpels cause less tissue distortion at surgical margin, less cautery artifact, and less margin fragmentation. 27 In addition, they are safe to be used with safety limit of 3–5 mm from the important structures (e.g., nerves). 28 Combined with endoscopes, more complicated procedures like total laryngectomy could be performed transorally, and the term “TransOral Endoscopic UltraSonic Surgery (TOUSS)” was first coined by Mario M Fernández-Fernández et al in 2015. This approach was proposed as a potential alternative to robotic surgery, yet less expensive.29,30 Our patient underwent resection of the rare pharyngeal fibrolipoma using the harmonic scalpel, and the procedure was easily done with minimal blood loss, little need for analgesia in the postoperative days, and relatively early postoperative oral feeding. Furthermore, the long tumor with limited stalk could be manipulated easily through the common oral access.
With adequate surgical excision, the prognosis of fibrolipoma is usually good.11,15 Unfortunately, our patient died 2 months after his operation due to urosepsis that was unrelated to the fibrolipoma; thus, longer follow-up period was not possible.
Conclusion
The advancements in endoscopic technology have resulted in easier diagnosis and surgical resection of fibrolipomas in the head and neck region with less morbidity compared to conventional methods. Furthermore, energy-based devices like harmonic scalpel are effective in many endoscopic procedures, and can have a bigger role in the future of head and neck surgery.
Footnotes
Acknowledgments
The authors thank everyone who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.