
Abstract
This report illustrates the successful removal of a proper intra-orbital oculosporidiosis (extralacrimal, extraconjunctival) exclusively by the endonasal endoscopic approach. It also introduces the naso-orbital pseudofontanelle as an important surgical landmark and describes a hitherto undefined intra-orbital extramucosal three-dimensional potential wedge that harbored the Rhinosporidium seeberi infestation as a nodular conglomerate. The patient, a 50-year-old woman, was operated on three years ago for rhinosporidiosis of the nasal cavity and the distal lacrimal drainage system (lacrimal sac and nasolacrimal duct). The resulting alterations in regional anatomy were evident on imaging. They could explain the present recurrence and formation of the pseudofontanelle that allowed the conglomerate to bulge through the lateral nasal wall on digital pressure, making endoscopic intervention feasible. The primary principle for adopting this approach was to protect the facial skin from possible seeding. With an angled endoscope, the pseudofontanelle was breached and the intra-orbital extramucosal wedge between the bony orbital wall and the peri-orbita entered. The nodules that formed the conglomerate were densely adherent with the peri-orbita and skin. They were carefully and meticulously removed to avoid inadvertent injury to vital intra-orbital structures. Endonasal endoscopic intervention for a true intra-orbital oculosporidiosis has never been documented before. The surgical approach, the newly defined anatomical domain for the intra-orbital extramucosal oculosporidiosis, and the concept of pseudofontanelle characterize this report as a novel clinical experience worth presenting.
Introduction
Oculosporidiosis is a chronic granulomatous disease caused by Rhinosporidium seeberi, an aquatic protistan parasite of the class Mesomycetozoea, that affects the eye.1,2 R. seeberi belongs to a group of fish parasites (the DRIPclade: dermocystidium, rosette agent, ichthyophonus, and psorospermium), and is abundant in freshwater bodies of southern India, Sri Lanka, and some Latin American countries.1-3 They mostly affect the nasal cavities (rhinosporidiosis) in people having the habit of pond bathing but may also affect the larynx, trachea, and bronchi, in addition to the skin and mucocutaneous areas such as the genitalia when disseminated. Oculosporidiosis is a relatively less common form that constitutes about 11-15% of the overall incidence, affecting mainly the lacrimal sac and nasolacrimal duct (the distal lacrimal drainage system), conjunctiva (predominantly palpebral), sclera, eyelids, and skin adjacent to the canthi.2,4 The treatment of choice for all forms of rhinosporidiosis is surgical removal, although even meticulous intervention might not prevent dissemination and recurrence due to intra-operative hemorrhage, poor vision, and residual spores. The endonasal endoscopic approach is preferred to address oculosporidiosis restricted to the distal lacrimal drainage system with/without involvement of the nasal cavity.4,5 However, this approach has never been reported before for a strictly intra-orbital oculosporidiosis that extends beyond the confines of the distal lacrimal drainage system and conjunctival sac. This report presents a unique clinical situation in which the altered anatomy of the rhino-orbital region secondary to a previous surgery helped us successfully adopt the endonasal endoscopic approach for oculosporidiosis that was extramucosal (extralacrimal, extraconjunctival) and intra-orbital.
Case report
A 50-year-old woman presented with a gradually progressive swelling under the left medial canthus for four months [Figure 1]. The swelling was firm, mildly tender, with a defined outline, and had restricted sideways mobility. The overlying skin was intact but edematous, with the lesion apparently adhered to it. The patient was otherwise asymptomatic and did not have co-morbidities. She was a farmer and had a history of pond bathing in her childhood. This 50-year-old woman presented with a gradually progressive, firm swelling under her left medial canthus for four months. The swelling had restricted sideways mobility and perilesional edema.
The patient was regularly followed up in our department after treatment for rhinosporidiosis three years back; the disease involved her left nasal cavity, the lateral nasal wall (inferior turbinate, uncinate process), and the distal lacrimal drainage system. Based on contrast-enhanced computed tomography and naso-endoscopy findings, she underwent extensive endonasal endoscopic surgery that included inferior turbinectomy, middle meatal antrostomy, dacryocystectomy and removal of the nasolacrimal duct, and powered drilling of the adjacent frontonasal process of maxilla, up to the orbital process of the frontal bone. The subsequent three years, prior to the development of her recent complaints, went uneventful.
Currently, gadolinium-enhanced magnetic resonance imaging (Gd-MRI) of the nose, paranasal sinuses, and orbits revealed a conglomerated mass of nodules with perilesional edema, intimately associated with peri-orbita and the medial aspect of the left bony orbit, encroaching posteriorly along the globe, pushing it behind [Figure 2]. The imaging sequence suggested that the conglomerate occupied an imaginary three-dimensional potential wedge within the orbit (which was further delineated later in surgery). The wedge was bounded anteriorly by skin, inferiorly by the orbital floor, posterolaterally by the anterior peri-orbita, and posteromedially by the medial orbital wall/lateral nasal wall, with the apex progressing posterosuperior within the bony orbit along the globe. Gd-MRI of the nose, paranasal sinuses and orbits [T2-weighted; A-C: coronal; D,E: axial] revealed a conglomerated mass of nodules with perilesional edema. The mass was intimately associated with the peri-orbita (yellow arrows) and the medial aspect of the left bony orbit. It encroached posteriorly along with the globe, pushing it behind and laterally [D,E]. The red line along the lateral nasal wall [A] indicates the pseudo-fontanelle, lateral to which the mass could be seen. The boundaries of the three-dimensional intra-orbital potential wedge harboring the mass could be appreciated in this imaging sequence. Also note the stigmata of the previous endoscopic surgery [B,C]. [Please refer to the text for the definition of “pseudo-fontanelle” (Discussion) and the “three-dimensional potential wedge” (Case Report).]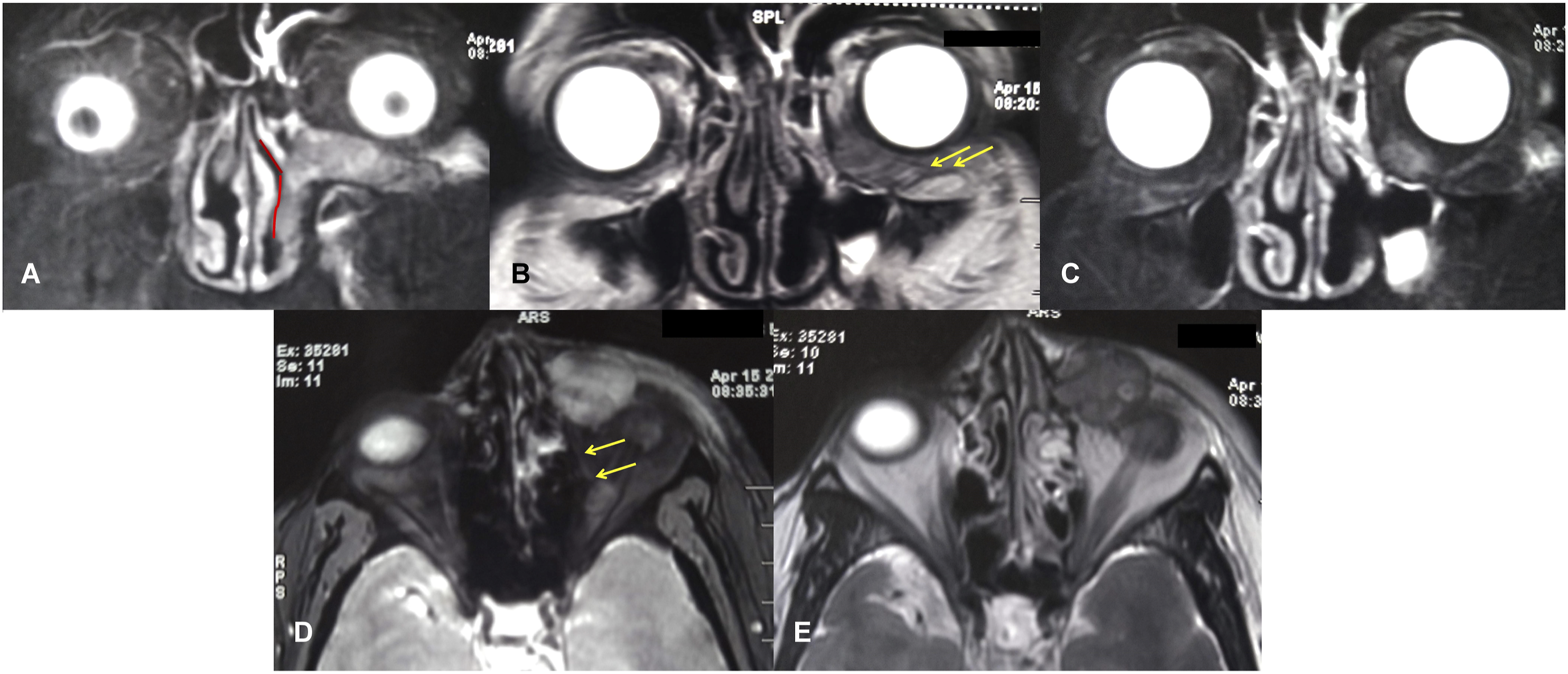
Naso-endoscopy at this stage was unremarkable with well-mucosalized lateral nasal wall and patent maxillary sinus neo-ostium. Given the previous history of rhinosporidiosis and due to its notoriety for recurrence, a provisional diagnosis of oculosporidiosis was made and the patient was planned for surgery.
Following consultation with our ophthalmology team, an entirely endonasal endoscopic approach was decided to prevent injury and subsequent seeding of the facial skin below the medial canthus. The surgical steps are depicted in Figure 3. The steps of surgery are shown in sequence. Naso-endoscopy showed well-mucosalized lateral nasal wall; the area in gray indicated the pseudo-fontanelle [A; please also refer to the Supplemental video]. A curvilinear incision was made with endo-cautery anterior to pseudo-fontanelle [B,C]. After the posterior-based flap was elevated with Freer elevator, the fibrous coat of the nodular conglomerate was visible [D]. With a 45º endoscope, under sustained digital pressure from outside, a plane was created between the nodules and the surrounding tissues (peri-orbita, skin). With a Freer elevator, the nodules could be carefully teased off from the adhesion and gently extracted through the nasal cavity [E-I]. After all the nodules were removed, the three-dimensional potential wedge within the orbit that harbored the conglomerate could be demonstrated [J,K; K is the magnified view of J; P=peri-orbita, M=nasal mucosa, S=septum].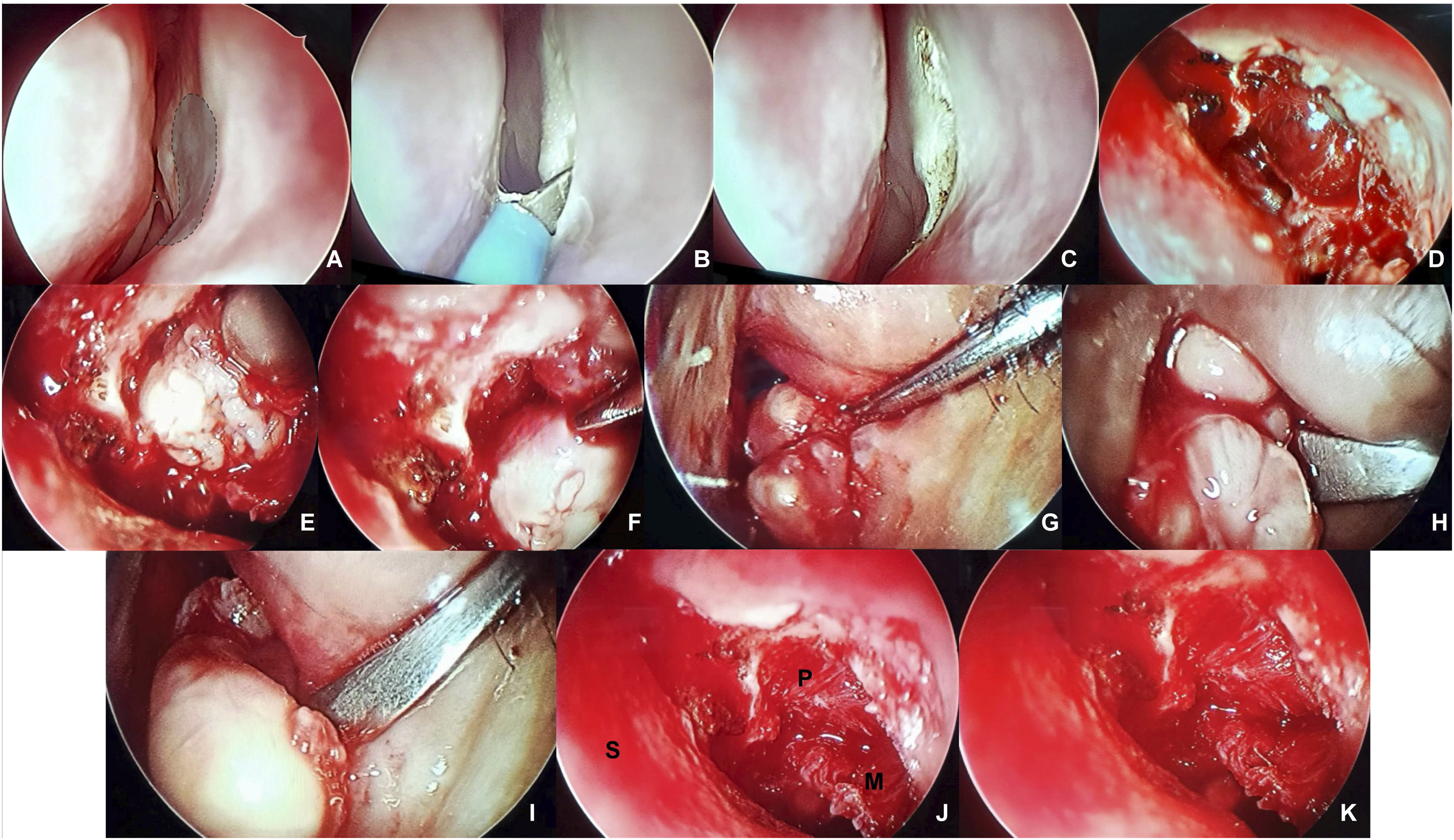
Under general anesthesia, a curvilinear incision was made with endo-cautery anterior to the area on the lateral nasal wall that produced a bulge when the mass was pushed medially. This mobile area in the lateral nasal wall would henceforth be termed “pseudo-fontanelle” (please refer to the Discussion below and to the Supplemental video). A posterior-based flap was elevated with Freer elevator and the fibrous coat of the conglomerate was visible. With a 45º endoscope, under sustained digital pressure from outside, attempts were made to create a plane between the nodules and the surrounding tissues (peri-orbita, skin). However, the nodules were densely adherent, and there were possibilities of inadvertent injuries during the process of dissecting them out. However, using blunt probing instruments, such as the Freer elevator and ball-point probe, the nodules could be gently teased off from the adhesion. The conglomerate occupied a three-dimensional potential wedge within the orbit, as described previously. After removal of the nodules that included even the most lateral and posterior ones, the intra-orbital wedge space was inspected for any residual lesion and irrigated with 5% povidone-iodine solution.
Following surgery, the patient was put on systemic steroids and antibiotics. The edema in the left naso-orbital region subsided in a few days. She recovered without complications. Histopathology of the nodules revealed large, thick-walled sporangia with endospores accompanied by a dense inflammatory infiltrate suggesting R. seeberi infestation [Figure 4]. The oculosporidiosis nodules were removed in their entirety [A]. Histopathology revealed large, thick-walled sporangia (arrowhead) with endospores (arrows), accompanied by a dense inflammatory infiltrate, suggestive of R. seeberi infestation [B,C; Haematoxylin-Eosin; x400]. The sporangia could be seen in various stages of degranulation.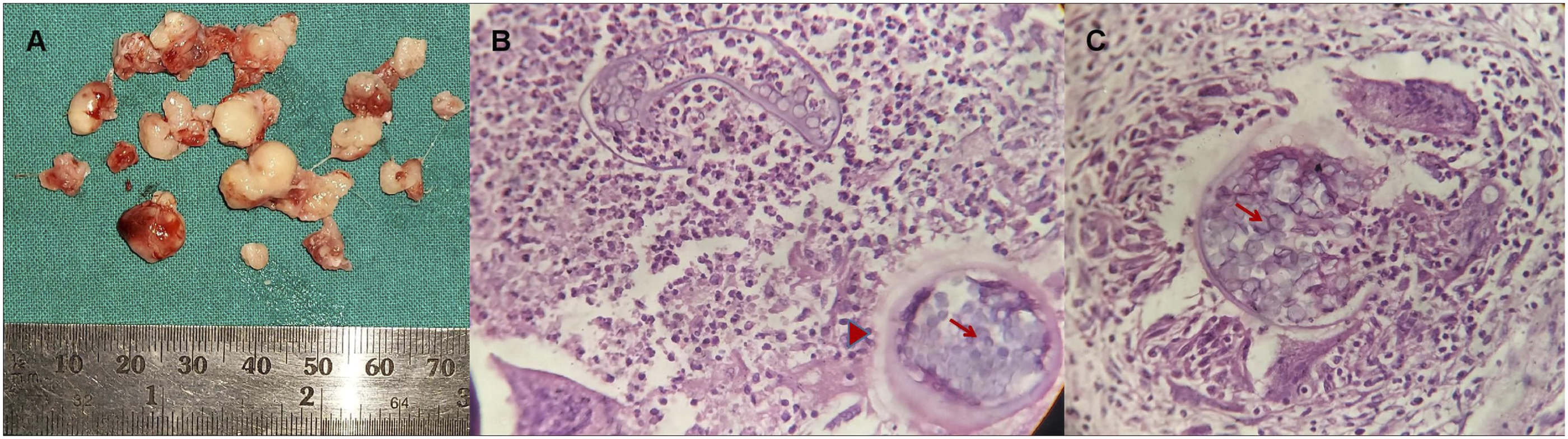
The patient had been under follow-up since eight months and was prescribed dapsone (tablet; 100 mg twice a day for six months). To date, there has been no recurrence, and a follow-up MRI after a month [Figure 5] showed the potential intra-orbital space collapsed and healed without any residual nodule. Gd-MRI at one month follow-up [A,B] showed the potential space within the left orbit collapsed and healed, without any residual nodule.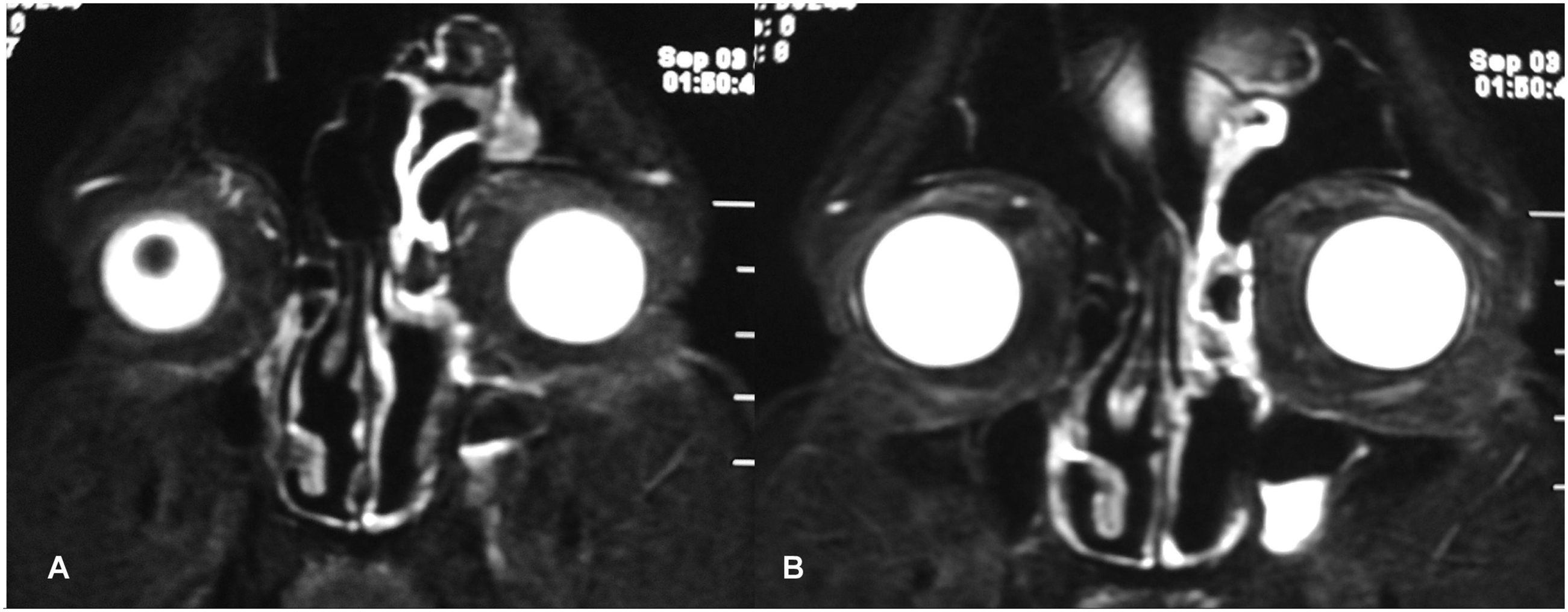
Written informed consent has been obtained from the patient for the publication of this clinical record. The clinical and surgical principles adopted for her management complied with the ethical standards of the relevant national and institutional guidelines on human experimentation, as laid down in the Declaration of Helsinki, 1975, as revised in 2008.
Discussion
This report describes an interesting clinical situation where the R. seeberi infestation, predominantly within the confines of the orbit (intra-orbital, extramucosal), was successfully addressed entirely through the endoscopic endonasal route. Due to the sacrifice of the distal lacrimal drainage system during surgery three years ago, the R. seeberi re-infestation was essentially extralacrimal. Additionally, the lesion did not involve the palpebral/bulbar conjunctiva; therefore, it was also extraconjunctival. In this sense, the lesion was truly intra-orbital and extramucosal, an unusual site for oculosporidiosis infestation. The intervention of choice for rhinosporidiosis involving the distal lacrimal drainage system is surgery through the endonasal endoscopic route, either dacryocystorhinostomy or dacryocystectomy with/without extirpation of the nasolacrimal duct, depending upon the lesion's extent.4,5 However, the approach presented here has never been described before for a proper intra-orbital lesion of this nature.
There were two factors that helped us adopt the endonasal endoscopic approach in this patient. The decision was based on a careful study of the MRI and after consultation with our ophthalmology colleagues. First, the R. seeberi conglomerate was closely associated with the skin below the medial canthus. The lesion could have been removed by external approach in a technically easier and less time-consuming manner. However, that would essentially violate the skin and would result in fistula and seeding.
Second, earlier surgery altered regional anatomy in a way that made the endonasal endoscopic approach feasible and practical. Removal of the bony bed of the lacrimal fossa along with generous drilling of the adjacent facial bone and skull base effectively created a "pseudo-fontanelle" [Figure 6; Supplemental video]. The term “fontanelle” here suggests apposition of the nasal mucosa and orbital tissue/peri-orbita; and we refer to it as “pseudo” as it was iatrogenic. It was this naso-orbital pseudofontanelle that allowed the conglomerate to bulge within when pushed medially. It also demarcated the endonasal endoscopic port of entry into the three-dimensional intra-orbital potential wedge that harbored the conglomerate. The boundaries of this newly defined wedge have been stated earlier (vide supra; Case Report). The concept of pseudo-fontanelle is demonstrated here as the endonasal conduit to the three-dimensional intra-orbital potential wedge space. The area in gray in the endoscopic endonasal view represents the pseudo-fontanelle [A]. Please also refer to the Supplemental video that demonstrates the mobility of this region on digital pressure. The pseudo-fontanelle signifies apposition of the nasal mucosa with peri-orbita without any intervening bone that was lost due to the previous surgery. The corresponding areas are shown in a skull to denote the extent of bone that was lost in the formation of the pseudo-fontanelle, and its location relative to the known anatomical landmarks [B, angled endoscopic view; C, external view through the orbit]. CP = cribriform plate; MT = middle turbinate; MS = maxillary sinus; S = septum; ALC = anterior lacrimal crest; PLC = posterior lacrimal crest.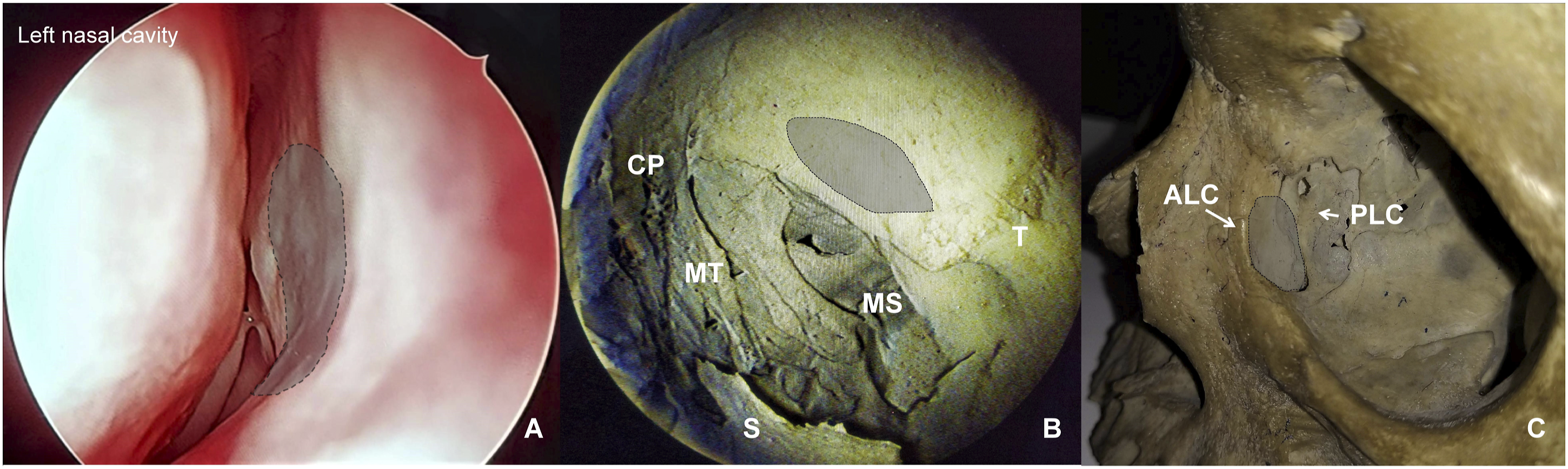
This unique anatomical modification in this patient explains how the previous nasolacrimal infestation of R. seeberi reached the intra-orbital space. With the absence of the distal lacrimal drainage apparatus, the recurrence was facilitated by the lack of resistance provided by the bony lacrimal bed and the adjacent lateral nasal wall. Fortunately, the recurrence was limited compared to the initial lesion by volume, but it created and expanded an extramucosal wedge space within the orbit, pushing the globe posterolaterally.
The morphology of the lesion at recurrence was different from that of the initial infestation, and this influenced our pre-operative experience. Unlike rhinosporidiosis, which is highly vascular, friable, and fleshy, oculosporidiosis in its most common locations is less vascular and presents as pale, discrete nodules.2,4 In our patient, these nodules coalesced to form a conglomerate with significant adhesion to the adjacent structures. Endonasal endoscopic removal of these adherent nodules posed a challenge that tested our technique, patience, and temperament. Working in an undefined anatomical space with sustained use of an angled endoscope amid dense adhesion invited chances of inadvertent injury to the peri-orbita and skin. The anterior peri-orbita was in closer relation to the sclera and the extra-ocular muscle tendons, with minimal peri-orbital fat. Injury to the anterior peri-orbita could lead to diplopia and visual compromise. Again, trauma to the skin would have defeated our reason for adopting the endoscopic approach in this patient. This was also why the wedge space adherent to the conglomerate was not purposefully cauterized following its removal. Here, it should be noted that before entering the wedge, the incision in the lateral nasal wall adjacent to the pseudofontanelle was made with endo-cautery so that the mucosal rim is burned, preventing seeding.
Therefore, although the dangers of the endonasal endoscopic approach were realized, its merits were more evident, and the intra-orbital nodular conglomerate representing the R. seeberi infestation could be meticulously and successfully removed even from the most lateral and posterior corners of the three-dimensional wedge space.
Conclusions
This report describes oculosporidiosis in a hitherto undefined intra-orbital, extramucosal compartment. This is also the first documentation of the removal of a truly intra-orbital R. seeberi infestation entirely through the endonasal endoscopic approach. The driving principle for opting for this route was to protect the facial skin from seeding, and the approach was facilitated by alterations in the regional anatomy caused by previous surgery. Identification and understanding the significance of the pseudofontanelle and the adjacent intra-orbital potential wedge space harboring the disease demanded improvisations in our surgical technique, and the resultant experience was rewarding and worth presenting.
Supplemental Material
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.