
Abstract
Rhinosporidiosis, an infectious granulomatous disease, is seldom encountered in the United States. We present a case of rhinosporidiosis in a 26-year-old man, who presented with an unusual mass in his nasal cavity. Suspicion for rhinosporidiosis was high due to the patient’s travel and activity history. After imaging and proper diagnosis, surgery was performed to excise the lesion. As international travel resumes during the COVID-19 pandemic, the potential for encountering this rare organism is heightened.
Keywords
Introduction
Rhinosporidiosis is an infective granulomatous disease rarely encountered in the United States. Caused by an organism called Rhinosporidium seeberi, there is controversy as to whether this pathogen is a water-borne fungus, a protozoan, or cyanobacterium. When acquired, it attacks the mucosal lining of the conjunctiva, nose, nasopharynx, palate, and urethra. It can affect other parts of the body (skin, trachea and brain), but these are rare.
Rhinosporidiosis is endemic to the Indian subcontinent, and cases have been reported in South America and Africa. It is rare in the United States, but when found, it is usually in the southeastern United States and Texas.
The typical presentation of rhinosporidiosis is nasal obstruction accompanied by epistaxis stemming from friable polypoid masses in the nasal cavity or sinuses. We present a case of rhinosporidiosis in a 26-year-old man. The University of Kansas IRB has granted an exemption for this case report.
Case Presentation
A 26-year-old man presented to ENT of New Orleans in the summer of 2020 for potential COVID-19 exposure. The patient was negative for symptoms and signs of COVID, but a granulomatous mass in the left nasal cavity was noted (Figure 1). CT scan of patient performed prior to excision; note polypoid lesion at anterior left septum.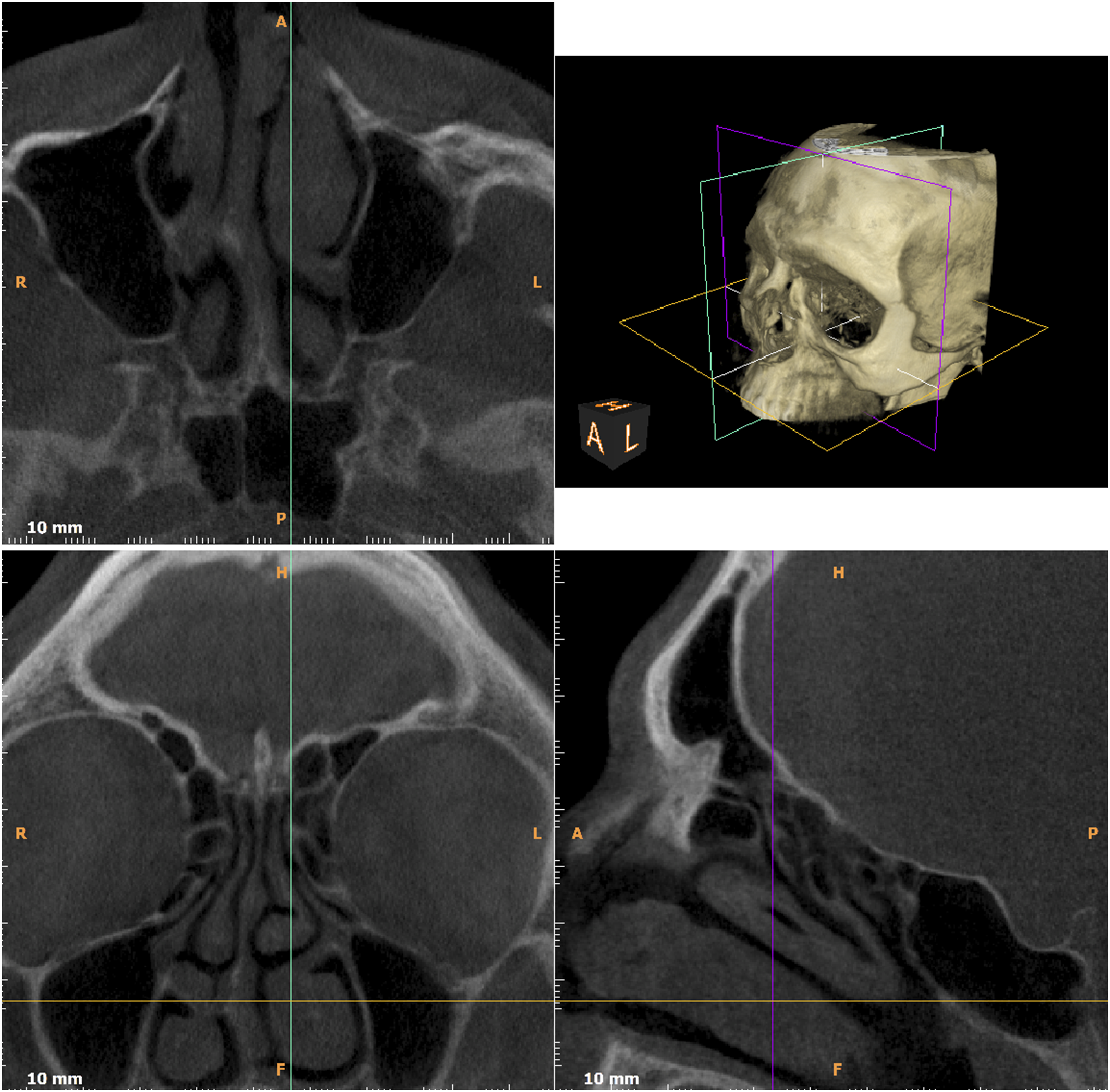
Upon examination, the patient had a badly deviated septum and engorged turbinates and was unable to breathe comfortably through his nose. This was attributed to a history of severe nasal trauma, and his nasal symptoms had been present for years. A lesion in the left nasal cavity was observed. The patient acknowledged that the lesion had been present for “a while” and was enlarging. CT imaging was obtained in order to evaluate the extent of disease. The patient was started on medications. There was no improvement, and the patient proceeded to surgery. Septoplasty was performed, and the left nasal mass was resected, ablated, and cauterized.
Surgical pathology revealed granulomatous inflammation. Parasitic structures were present within the granulomatous inflammation. The pathology report noted no evidence of fungus, indicating instead the existence of rounded bodies with brightly eosinophilic walls (consistent with the cuticle of a parasite). Pathology recommended that the travel history of the patient be examined in the interest of a possible diagnosis of rhinosporidiosis (Figure 2). Microscopy from pathology. Note the cuticle of the parasite highlighted by PAS stain, as well as surrounding inflammation.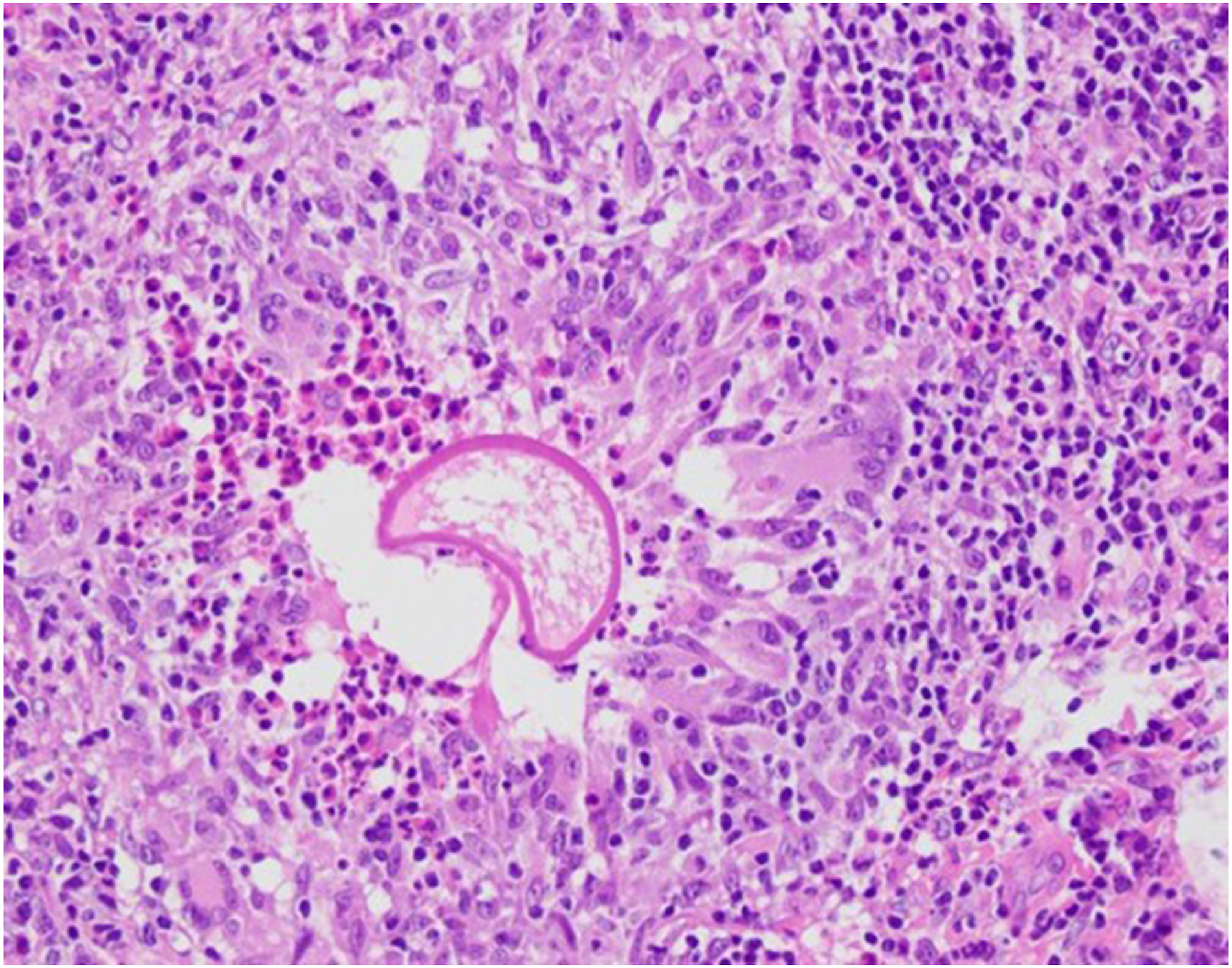
The patient acknowledged travel to many overseas locations, including India. In addition, the patient had been a participant in “Tough Mudder” races.
Discussion
Rhinosporidiosis has been documented for over a century 1 (first in Argentina in 1896), but its causative organism, Rhinosporidium seeberi, has proven difficult to culture. This resistance to culture has led in turn to difficulties in identifying its taxonomy as it lies at a divergent point between animals and fish. It was originally classified as a fungus but is now regarded as an aquatic parasite. It is believed to be transmitted in stagnant pools shared by animals as it has also been encountered in dogs, cats, horses, and other mammals.
Rhinosporidiosis usually affects the mucosa of the nose, nasopharynx, conjunctiva, palate, and urethra. It can involve other body parts (oropharynx, trachea, ear, and rectum) and typically presents with unilateral nasal obstruction, rhinorrhea, coryza with sneezing, localized pruritus, and postnasal drip. Patients often report a foreign body sensation in the nose.
Physical exam will show soft polyps with a pink to red coloration and have been described as strawberry-esque in appearance. These polyps are friable and vascular and can be pedunculated or sessile. They bleed easily upon manipulation. 2 It is worth noting that these polyps originate from locations such as the mucosa of the nasopharynx, inferior turbinate, nasal floor, septum, or anterior nares. Thus, if polyps arise in locations other than the middle turbinate, it is worth including rhinosporidiosis in the differential diagnosis. 3
Definitive diagnosis comes from histopathology as well as a thorough travel history. Stains include mucicarmine, Gomori methenamine silver, periodic acid-Schiff, and H&E stains. The mainstay of treatment is surgical excision as medical intervention has historically not proven successful. Some literature indicates that long courses of dapsone may be effective. 4
Conclusion
We have presented a case of rhinosporidiosis in a 26-year-old man with travel and activity history putting him at high risk for this disease. While rare in the United States (the last case report on rhinosporidiosis in the literature was in 1984 in Arkansas 5 ), the resumption of international travel plus known risk factors (exposure to stagnant pools shared by animals) renders this disease a significant consideration (however rare) for chronic granulomatous disease of the nasal cavity. As such, it is worth following up index cases to determine prevalence and source of infection.
Footnotes
Acknowledgments
ENT of New Orleans would like to acknowledge the generous assistance of the University of Kansas Department of Otolaryngology and Head and Neck Surgery and Delta Pathology Group in this case report.
Author’s Note
ENT of New Orleans:
Gregory W. Pippin, MD
Thomas M. Irwin Jr, MD, Adil A. Fatakia, MD/MBA
Delta Pathology Group:
James E. Brown Jr, MD, William H. Luer, MD
LSU Pathology Residents
Fernanda Da Silva Lameira, MD, Walter Beversdorf, MD.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.