
Abstract
Objectives
The incidence of odontogenic sinusitis has been gradually increasing due to the recent increases in invasive dental procedures. This study aimed to describe the clinical features of present patients with odontogenic sinusitis compared to the past, confirm the importance of endoscopic sinus surgery (ESS), and analyze the predictive factors for ESS.
Methods
This retrospective review included all patients diagnosed with odontogenic sinusitis between January 2010 and December 2011 and between January 2019 and December 2020. The patients were classified into 2 groups (past and present) depending on the time of the first visit. The clinical characteristics and treatment modalities were compared between the two groups. In addition, among patients in the present group, we analyzed variables to identify factors contributing to the risk of undergoing ESS.
Results
This study included 56 patients (23 in the past group and 33 in the present group). Compared to the past group, the present group had an older mean age (P = .001) and significantly increased iatrogenic etiologies (52.1% vs 90.9%; P = .002). The proportion of patients treated with ESS also increased in the present group compared to that in the past group (39.1% vs 66.7%; P = .041). In the present group, 11 patients (33.3%) were cured with conservative treatment, while 22 patients (66.7%) underwent additional ESS. Multivariate analysis revealed that the Lund–Mackay score was the only significant predictor of ESS (odds ratio [OR]: 14.901, P = .035).
Conclusion
The incidence of odontogenic sinusitis with iatrogenic etiologies has increased compared to the past. In addition, two-thirds of the patients in the present study underwent ESS, a significantly higher proportion than in the past. Therefore, ESS is one of the most important treatment modalities for odontogenic sinusitis, especially iatrogenic, in recent years. A severe Lund–Mackay score was associated with a significantly increased risk of ESS.
Introduction
Sinusitis is a multifactorial inflammatory disease caused by environmental allergens, viral infections, bacterial infections, fungi, and/or odontogenic problems. 1 Approximately 10% of all sinusitis cases are attributed to odontogenic problems, and odontogenic sinusitis should be treated with special care because of its different microbiology, diagnostics, and treatment compared to sinusitis with other etiologies. 2 The overall incidence of odontogenic sinusitis is still known to be relatively low, but several studies have reported its increasing incidence in recent years.3-5
Odontogenic sinusitis occurs when the Schneidarian membrane of the maxillary sinus is inflamed or injured; the resultant inflammation or injury causes mucosal inflammation and worsens mucociliary function within the maxillary sinuses. 6 The most common etiology of odontogenic sinusitis is iatrogenic injuries, including dental extraction, dental implant, and maxillary sinus augmentation (or sinus lift), which have gradually become more common. 4 Recent studies have demonstrated the contribution of the increasing rates of these dental procedures in recent years to an increased incidence of iatrogenic etiologies of odontogenic sinusitis.6-8
Endoscopic sinus surgery (ESS) may be necessary for patients with odontogenic sinusitis in whom initial medication and dental treatment have failed. The risk of undergoing surgery varies depending on the etiology of odontogenic sinusitis.9-11 Sinusitis caused by periodontal diseases, such as infections of the structures around the teeth, often improve with conservative management alone; however, odontogenic sinusitis with iatrogenic causes underwent surgery in approximately 80% of cases. 12 As the proportion of iatrogenic cases of odontogenic sinusitis increases, the risk of surgery is also increasing. Therefore, otolaryngologists play an increasing role in the treatment of odontogenic sinusitis.
This study aimed to describe the changes in the clinical characteristics and treatment modalities of patients with odontogenic sinusitis compared to the past, confirm the importance of ESS, and analyze factors predicting the risk of undergoing surgery through a retrospective chart analysis.
Materials and Methods
Patients
This study was approved in advance by the Institutional Review Board of Korea University Guro Hospital. We performed a retrospective chart review of all patients diagnosed with sinusitis who visited the Department of Otorhinolaryngology-Head and Neck Surgery at our hospital between January 2010 and December 2011 and between January 2019 and December 2020. Sinusitis was diagnosed according to European Position Paper on Rhinosinusitis and Nasal Polyps guidelines. 13 Among patients with sinusitis, this study included those diagnosed with odontogenic sinusitis. The diagnosis of odontogenic sinusitis was based on a thorough chart analysis and imaging review, including computed tomography (CT) scans of the paranasal sinuses (PNS) and nasal endoscopic images. All the included patients had a clear temporal and causal connection between dental problems and the appearance of the rhinologic symptoms. Patients with any of the following were excluded from the study: incomplete data, bilateral rhinosinusitis or nasal polyposis, previous ESS, and/or lack of follow-up until the disease was completely cured.
Measures
Demographic factors, comorbidities, duration of symptoms, and etiologic factors (periodontal disease, extraction, dental implant, or maxillary sinus augmentation) were analyzed by reviewing the medical records of the enrolled patients.
Initial PNS CT scans and nasal endoscopic images were also reviewed to evaluate the severity of sinusitis, obstruction of the osteomeatal unit (OMU), and haziness of the maxillary sinus. The severity of sinusitis was evaluated using the Lund–Mackay score. We checked the haziness at 6 sites (anterior ethmoid sinus, posterior ethmoid sinus, frontal sinus, sphenoid sinus, maxillary sinus, and OMU) and ranked each from 0 to 2 (normal state: 0, partial haziness: 1, total haziness: 2). Using nasal endoscopic images and PNS CT scans, we graded the obstruction of the OMU from 0 to 2 (0, no obstruction; 1, partial obstruction; 2, complete obstruction). The haziness of the maxillary sinus was ranked into 4 stages by PNS CT scans (1: 0–25%, 2: 25%–50%; 3: 50%–75%: 4: 75%–100%).
We also checked the treatment modalities through a chart review of all patients. We analyzed whether the patients were treated with conservative management (antibiotics, dental treatment, and/or sinus irrigation) or underwent additional surgical treatment.
Group Classification
We classified all enrolled patients into two groups according to the time of their first visit. Patients who visited our hospital between January 2010 and December 2011 were classified into the past group, while those who visited between January 2019 and December 2020 were classified into the present group. By comparing these two groups, we investigated the changes in demographics, clinical characteristics, and treatment modalities between past and present patients with odontogenic sinusitis.
Additionally, we divided the patients in the present group into two groups based on treatment modalities (conservative and surgical groups). By comparing the measurements between these two groups, we investigated which factors contributed to changes in the treatment modalities and analyzed the risk factors for undergoing surgery.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics for Windows, version 22.0 (IBM, Corp., Armonk, NY, USA). The results are shown as means ± SE. Pearson’s chi-square, Fisher’s exact, and Mann–Whitney U tests were used to compare factors between groups. In addition, univariate and multivariate logistic regression analyses were performed to describe the factors contributing to the risk of surgical treatment. Statistical significance was set at P < .05.
Results
Past Versus Present Groups
Demographics and clinical characteristics of the past and present groups.
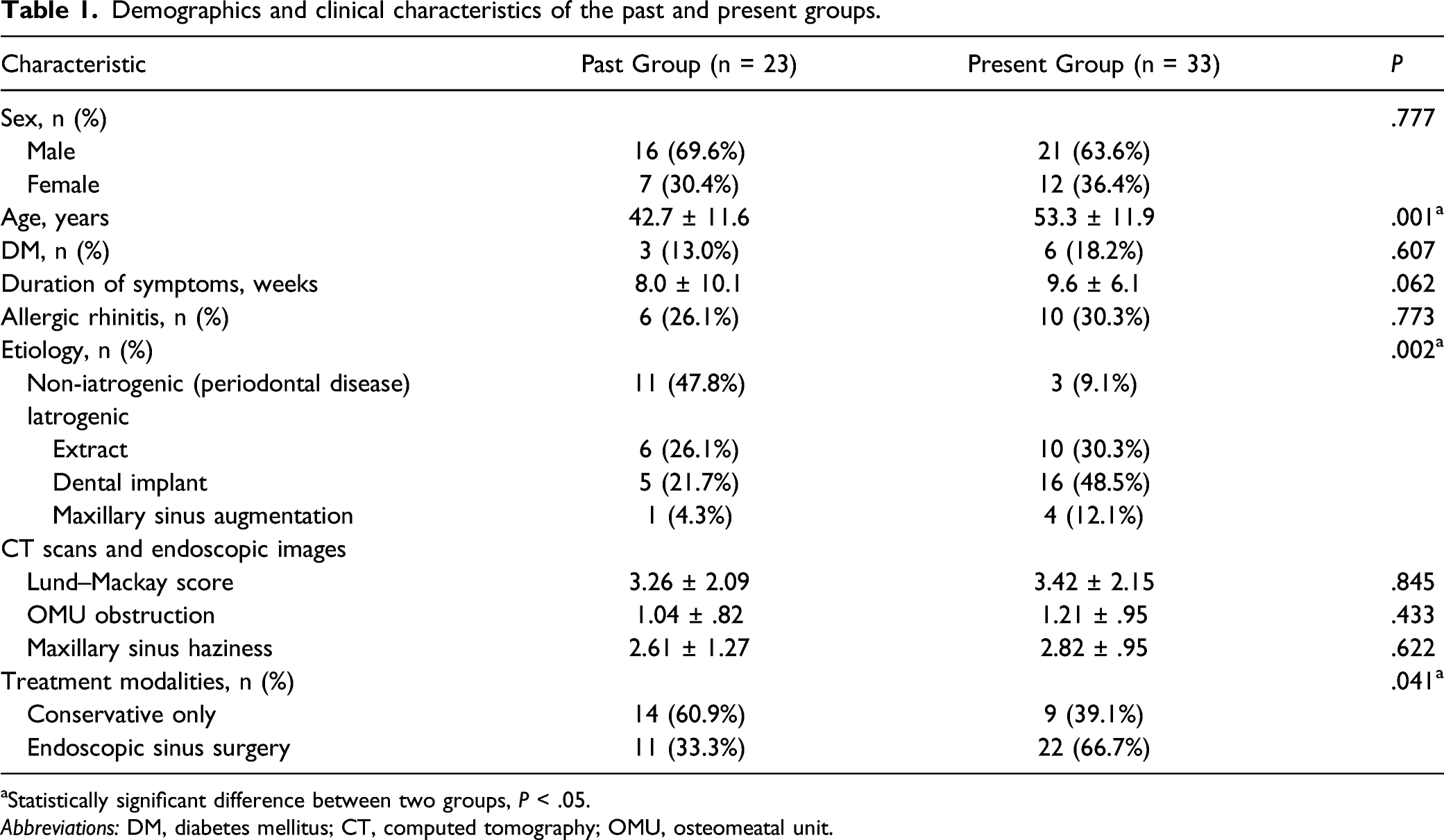
aStatistically significant difference between two groups, P < .05.
Abbreviations: DM, diabetes mellitus; CT, computed tomography; OMU, osteomeatal unit.
Conservative Versus Surgical Groups
Comparisons of demographics and clinical characteristics between conservative and surgical groups.
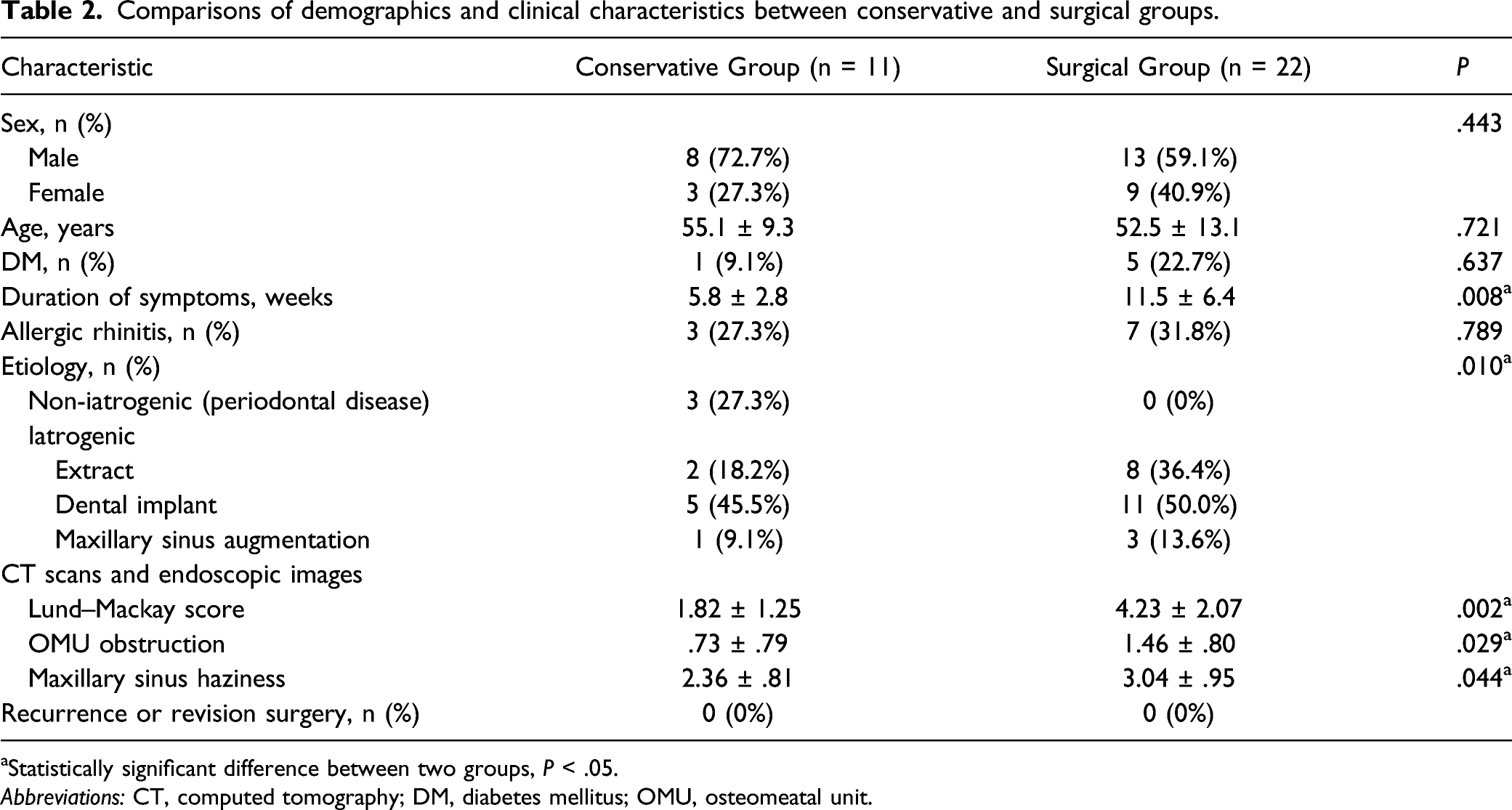
aStatistically significant difference between two groups, P < .05.
Abbreviations: CT, computed tomography; DM, diabetes mellitus; OMU, osteomeatal unit.
Results of univariate and multivariate logistic regression analyses.
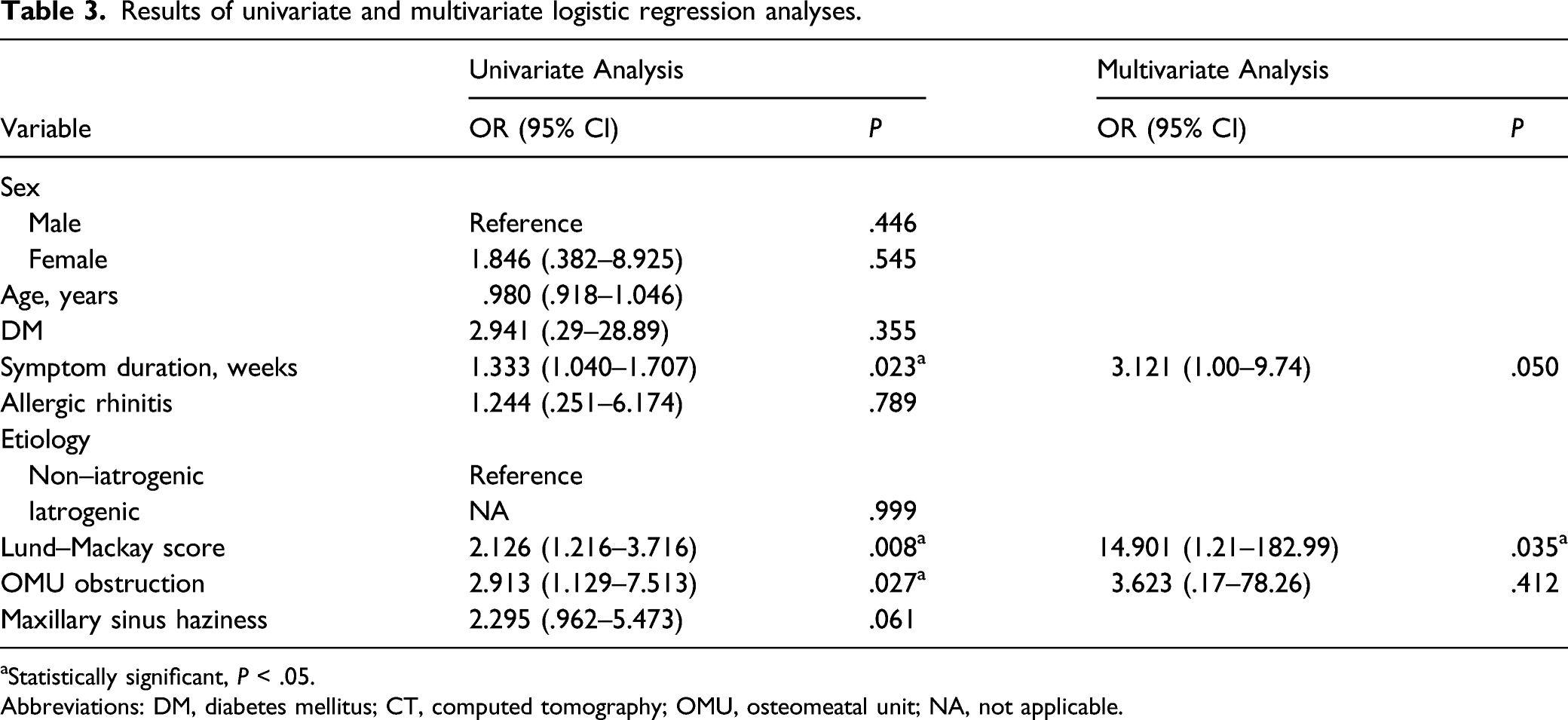
aStatistically significant, P < .05.
Abbreviations: DM, diabetes mellitus; CT, computed tomography; OMU, osteomeatal unit; NA, not applicable.
Discussion
The incidence of odontogenic sinusitis has gradually increased in recent years and odontogenic pathology, particularly in unilateral maxillary sinusitis, is an important cause of rhinosinusitis.4,5 Odontogenic maxillary sinusitis is one of the most common odontogenic infections in the head and neck area, and has been known to account for the largest number of patients with odontogenic infections requiring hospital admission. 14 The etiologies of odontogenic sinusitis include periodontal disease, trauma to the maxillary sinuses or teeth, and iatrogenic causes such as implant-related procedures or tooth extraction. A meta-analysis conducted in 2010 reported the following order of odontogenic sinusitis etiologies: iatrogenic (55.97%), periodontitis (40.38%), and odontogenic cyst (6.66%). 7 Another systematic review in 2014 investigating the etiology of odontogenic sinusitis among 674 patients reported that approximately 65% of cases were attributed to iatrogenic etiologies; 25.1% had periodontal disease, and 8.3% had marginal periodontitis. 15 Iatrogenic etiologies account for the largest proportion of the causes of odontogenic sinusitis and recent increases in invasive dental procedures, including dental implant and maxillary sinus augmentation, have gradually increased the proportion of iatrogenic etiologies for odontogenic sinusitis.5,16
In our study, iatrogenic etiologies, which accounted for approximately 52.1% of all causes 10°years ago, have increased significantly, recently accounting for 90.9% of all causes. The most likely explanation for this trend may be coverage of dental implants for older people by the Korean National Health Insurance Service starting in 2014. Subsequently, older adults have increased access to dental care, and therefore, iatrogenic factors, including tooth extraction and dental implant-related procedures, have been increasing rapidly. 17 This point is also consistent with our finding that the mean age of the present group was significantly higher than that of the past group.
Among the available methods for the treatment of odontogenic sinusitis include medication, dental treatment, ESS, and concomitant management of dental problems and related sinusitis are very important. Antibiotic therapy along with dental treatment is usually the initial treatment for patients with odontogenic sinusitis; however, patients who do not respond to conservative treatment undergo surgical treatment such as ESS. 8 Many studies have analyzed treatment strategies, and treatment methods may vary depending on the etiologies of the odontogenic sinusitis or the clinical characteristics of the patients.18,19 Therefore, the management of odontogenic sinusitis must be tailored to individual patients and requires various combinations of medication, dental treatment, and ESS.
Many studies have also investigated the role of ESS in the management of patients with odontogenic sinusitis. Studies on patients with iatrogenic etiologies reported relatively high rates required surgery.9,19-21 Kim et al. analyzed 19 patients treated for odontogenic sinusitis resulting from dental implants; only 21% of patients were successfully treated with conservative management, while 79% required ESS.
12
In addition, Chen et al. reported that 15 of 18 patients with odontogenic sinusitis due to dental implants required surgical treatment.
21
Two representative causes of iatrogenic odontogenic sinusitis are extraction and dental implant; the reasons for the high rate of undergoing surgery are as follows. First, when odontogenic sinusitis occurs due to tooth extraction, additional dental treatment is not necessary and ESS should be primarily considered if medical treatment is ineffective (Figure 1A).21,22 Second, in the case of dental implants or maxillary sinus augmentation, the implant materials or augmentation protrude into the maxillary sinus and sinusitis occurs. Early-stage ESS is more advantageous for improving maxillary sinusitis by removing foreign materials and improving sinus ventilation (Figure 1B and C).21,22 Therefore, in this study, the incidence of iatrogenic etiologies increased significantly compared to 10°years ago, which increased the risk of undergoing surgery. Computed tomography scans of the paranasal sinuses showing 3 representative types of iatrogenic etiologies included in this study. All 3 cases were cured by endoscopic sinus surgery. (A) Temporary oroantral fistula after dental extraction (yellow arrow). (B and C) Cases with protrusion of implant material (arrowhead) and sinus augmentation (asterisk) into the maxillary sinus were treated by removing the foreign materials and improving ventilation during endoscopic sinus surgeries.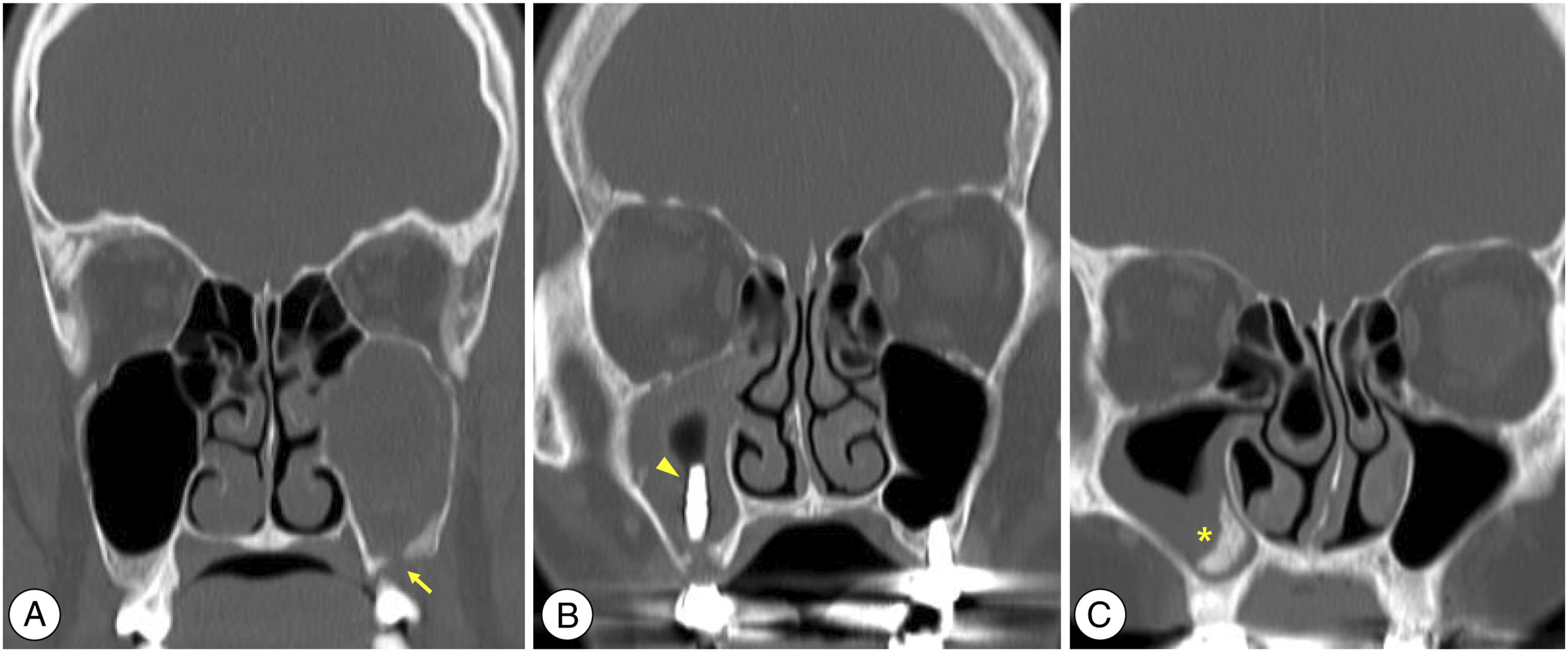
Alternatively, periodontal disease can occur in cases of chronic infection in tooth structures; this results in mucosal inflammation and worsening of mucociliary function in the maxillary sinuses. 23 Odontogenic sinusitis due to non-iatrogenic etiologies is initially treated with medication along with management of the underlying dental pathology, including apicoectomy, or dental extraction.9-11 Endoscopic sinus surgery may be performed for patients who fail initial medication and dental management; however, the proportion of patients undergoing surgery is lower than that of sinusitis due to iatrogenic etiologies. Yoo et al. explored the treatment strategy for odontogenic sinusitis in 33 patients who developed sinusitis due to periodontitis resulting from dental caries or periapical abscess. Among a total of 33 patients, 22 (67%) were cured with medical and dental treatment, and only one-third of the patients required additional ESS. 18 Therefore, otolaryngologists may not encounter many non-iatrogenic patients; in our study, only 3 patients in the present group had conditions that were non-iatrogenic-related and all 3 were cured with conservative treatment alone.
Another concern in our study was the identification of factors predicting for undergoing ESS in odontogenic sinusitis, as early surgery can reduce the treatment period. In addition, the patient–physician relationship can also be improved by appropriately counseling patients who are most likely to undergo surgery. A recent study of patients with dental implant-associated sinusitis showed that patients who underwent ESS had a significantly higher rate of OMU obstruction, along with more severe Lund–Mackay scores. 12 In another study, OMU obstruction and previous dental procedures were significant predictors of ESS in patients with odontogenic sinusitis. 9 In studies on patients with non-iatrogenic etiologies, Lund–Mackay scores and smoking were predictive factors for surgery. 18
We analyzed the treatment modalities of the present group, excluding the past group, to examine recent treatment strategies. Approximately 67% of patients in the present group (22 of 33) were not cured with initial conservative treatment; therefore, ESS was performed. Multivariate analysis identified only Lund–Mackay score as a predictor of patients undergoing ESS (odds ratio [OR]: 14.901, P = .035). Consistent with the results of previous studies, we confirmed that the Lund–Mackay score is a powerful factor in predicting surgery. A high Lund–Mackay score indicated that the disease involved many more sinuses beyond the maxillary sinus, the diseases were worse in degree and extent, and the diseases were more likely to require surgery. Craig et al. also reported that the ESS group showed a tendency for a longer symptom duration compared to the conservative treatment group, although the difference was not statistically significant. 20 Similar results were also found in our study. Thus, surgeons should be aware that ESS may be necessary when counseling patients with long symptom duration.
This study had several limitations. Owing to the retrospective design, some patients may have been missed due to missing data or problems in the search process, which could have resulted in a selection bias. Data on the exact dental procedures of the treatments were also not available for concurrent dental treatment at other institutions. Lastly, there was a limitation in deriving statistically significant results due to the small number of patients. Further investigation of patient outcomes in a prospective study may compensate for these limitations.
Conclusion
The incidence of odontogenic sinusitis attributed to iatrogenic etiologies has been increasing rapidly and accounts for most odontogenic sinusitis patients in recent years. This recent trend is very important for otolaryngologists because many patients with iatrogenic etiologies underwent surgery. In addition, the clinical characteristics of patients can help determine treatment strategies; among these, the Lund–Mackay score was a significant factor in predicting for undergoing ESS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Korea University Guro Hospital (KOREA RESEARCH-DRIVEN HOSPITAL) and grant funded by Korea University Medicine (K2110261).
Authors Note
Jae-Min Shin and Su-Jong Kim contributed equally to this work.