
Abstract
By summarizing and analyzing the diagnostic and treatment process of a case with atypical Stevens–Johnson syndrome (SJS) characterized by mucosal ulcerations of the pharynx and larynx, and reviewing related literature, we would like to remind that in the presence of unexplained mucosal lesions, atypical SJS should not be ignored.
Keywords
A 38-year-old man with a painful expression and listless spirit was admitted to the hospital. He complained of a sore throat, dysphagia, and tearing after acquiring a cold 3 days earlier, and sought treatment in a local hospital. Medication with cefazolin, dexamethasone, fluconazole, aescin, aerosol inhalation, and sodium bicarbonate gargle did not result in significant improvement in symptoms. On admission, his vital signs were steady. Ulcerations in lips, gums (Figure 1A), uvula, soft palate, base of the tongue, and tonsils were observed, as well as conjunctival congestion in both eyes (Figure 1D). He had been treated for reactive arthritis for a year with intermittent oral sulfasalazine and Voltaren. He had no family history of illness or drug allergies. Mucosal ulcer-bleeding-scab of lip and gums and conjunctival congestion (A: mucosal ulcer-before treatment, B: mucosal bleeding-during treatment, C: mucosal scab-after treatment, D: conjunctival congestion in both eyes).
Fungal infection of the throat was initially suspected based on the patient’s symptoms and signs, but tuberculosis and rheumatic immune diseases such as Behcet’s disease could not be ruled out. Fiber laryngoscopy was performed right after admission, and the results revealed that the oropharynx, hypopharynx, and laryngeal mucosa were all red and swollen, with white ulcers scattered throughout (Figure 2). Medications including methylprednisolone, clindamycin, dafukang, pulmicort aerosol inhalation, sodium bicarbonate gargle, and growth factor spray as well as other symptomatic and rehydration support treatments were given right after admission. Blood routine, C-reactive protein, erythrocyte sedimentation rate, mycobacterium tuberculosis, throat swab bacterial culture and drug sensitivity, bacterial smear, fungal smear, and sputum inspection were performed but revealed no significant abnormal results. Mucosal ulcerations of the pharynx and larynx (A: uvula and posterior pharyngeal wall; B: larynx cavity; C: right pyriform fossa; D: left pyriform fossa).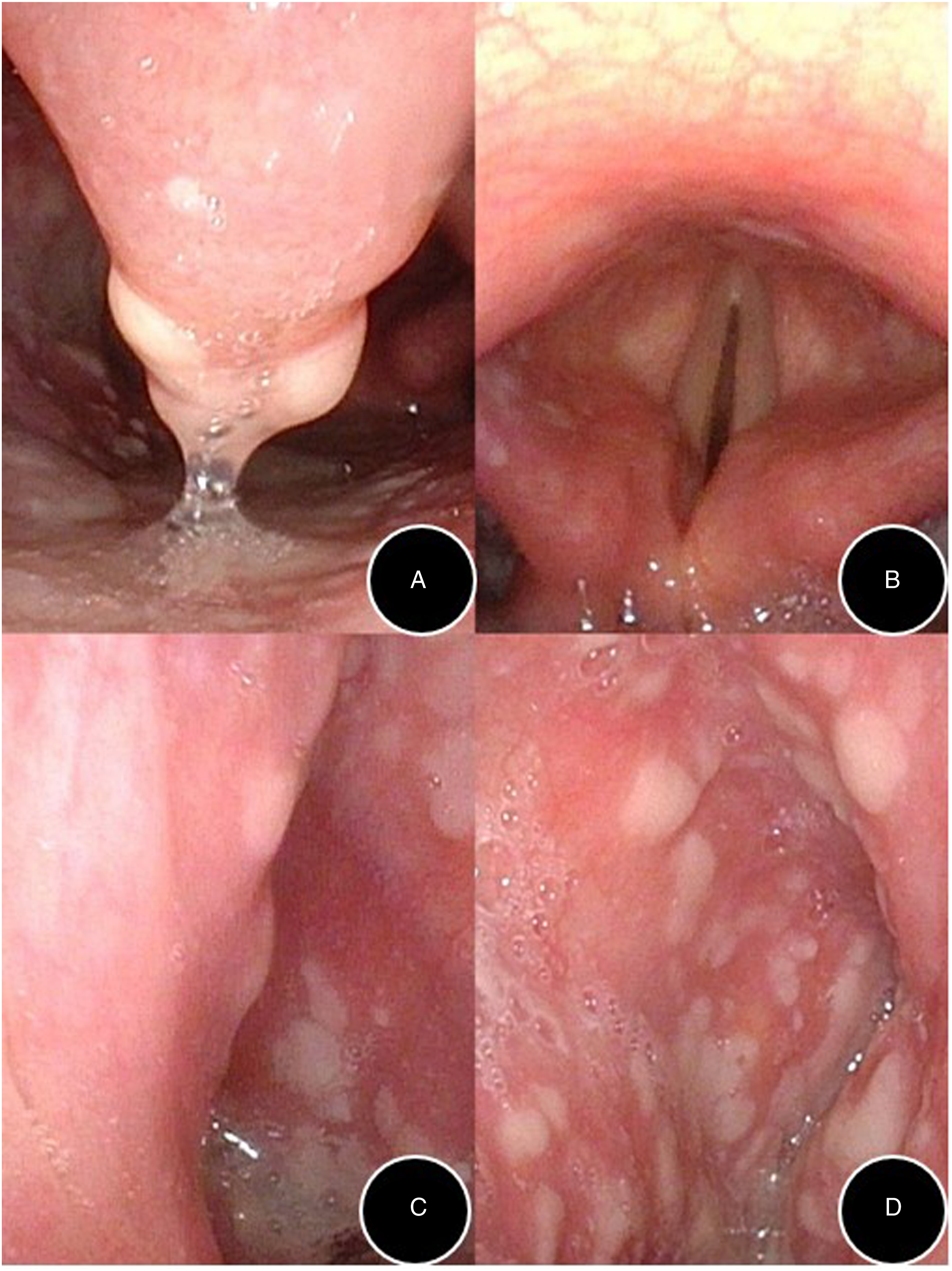
After consulting with doctors from the Departments of Infectious Diseases and Rheumatology and Immunology, the medication plan was changed the next day to include an intravenous drip of ceftriaxone, metronidazole, fluconazole, and oral Lianhua Qingwen granules with continued atomization, mouthwash, spray, and nutrition support treatment. The presence of antibodies against viruses including respiratory pathogens, TORTH, and Epstein-Barr virus antibody, as well as autoantibodies, humoral immune function, immunoglobulin G4, and antineutrophil antibodies and subtypes was detected and no abnormal results were found.
Based on the suggestions of doctors from the Department of Rheumatology, sulfasalazine and Voltaren were discontinued. The patient was diagnosed with atypical Stevens–Johnson syndrome (SJS) after further consultation with a doctor from the Department of Dermatology. Glucocorticoids, antibiotics, and nutritional support were recommended to be continued, as well as subcutaneous injection of Etanercept at 50 mg was initiated after tumor was ruled out. Clapton eye drops, pranoprofen eye drops, and erythromycin eye ointment were applied following recommendations from an ophthalmologist.
According to the consultations, the therapy plan was changed and the patient completed the relevant examinations. The patient received Etanercept treatment after ruling out tumors, and the sore throat and dysphagia gradually alleviated, and the pharyngeal mucosal ulcers slowly healed. One week later, he was discharged from the hospital. On the day of his discharge, the pharyngeal mucosa partially fell off and the lips began to bleeding and crust (Figure 1B). After discharge, the blood crust of the patient’s lips regularly fell off and a film-like substance developed on the floor of the pharyngeal and conjunctival ulcers after healing, and then gradually fell off till the mucosal floor became normal (Figure 1C). About 1 month postdischarge, his throat symptoms essentially disappeared, and only slight dryness of the nasal cavity and dry eyes remained, and which eventually disappeared in about 6 months. During the one-year follow-up, no throat and eye discomforts, such as sore throat, dysphagia, and tearing, occurred again.
Discussion
Stevens–Johnson syndrome
Stevens–Johnson syndrome is a serious skin and mucosal reaction and may also be accompanied by multiple organ involvement. 1 It is characterized by blisters and generalized epidermolysis and in most cases is triggered by drugs. The lesions exhibit as atypical erythema, purpura-like spots, blisters, and bullae, which rapidly fuse into a piece and unfold throughout the body. The mucous membranes of the eyes, mouth, nose, and genitalia are regularly affected and present as erosive hemorrhagic mucositis. 2 Stevens–Johnson syndrome normally appears 4–28 days after taking the suspicious drug, and the cure time depends on the length of exposure time to the sensitizing drug. 3
The incidence rate of SJS is low and approximately 1–7/1 000 000 4 are reported annually. However, the mortality rate is as high as 4.8%. 5 Its pathogenesis is generally associated with drugs and the genetic background of the body. Common exogenous drugs that can induce SJS include anticonvulsants, antidepressants, sulfonamides, NSAIDs, anti-infective drugs, and targeted drugs. 6 Genetic background is commonly associated with the polymorphism of human leukocyte antigen (HLA). Domestic and foreign scholars have discovered that HLA-B*1502, HLA-B*5701, HLA-B*5801, HLA-B*5901, HLA-B*1301, and other genes are associated with SJS, 1 among which HLA-B*1301 is associated with SJS induced by sulfasalazine. 7 Histopathologically, SJS lesions are accompanied with extensive apoptosis and necrosis of epidermal keratinocytes, which are primarily mediated by drug-specific cytotoxic T cells. FasL, perforin, granzyme, TNF-α, INF-γ, and carbon monoxide synthase are believed to be significantly associated with the occurrence and development of SJS. 8
Analysis of sensitizing drugs
The drugs suspected in this case were Voltalin and sulfasalazine. Voltalin (diclofenac sodium enteric coated tablets) is a type of NSAIDs. In the drug instructions, skin rash is a rare adverse event and SJS is not mentioned. However, it cannot be definitely ruled out as SJS induced by diclofenac sodium sustained-release capsules has been reported. 9
Sulfasalazine is an azo compound of salicylic acid and sulfapyridine. It has antibacterial, antirheumatic, and immunosuppressive effects. Among its adverse drug reactions, erythema multiforme or SJS is the most common. The contraindications include hypersensitivity to sulfasalazine and its metabolites, sulfanilamide, and salicylic acid. The patient’s history of drug sensitivities was investigated in detail. He did not have a clear history of drug sensitivity; however, his mother had a history of sulfonamide allergy. We reasoned that sulfasalazine is more likely to have triggered SJS in this patient.
If a single drug is used, the sensitizing drug can be identified directly. However, it is difficult to decide the sensitization drugs when taking multiple drugs at the same time. The Alden algorithm can be used for the retrospective assessment of sensitizing agents for SJS. 2
Treatment plan
(1) General treatment: All suspected sensitizing drugs should be stopped, and airway patency should be ensured. Antibiotics, rehydration, desensitization, analgesic, and nutritional support should be used for treatment and water, electrolyte, and acid–base balance should be maintained. Regular rinsing of the mucous membrane of the eyes, mouth, nose, and vulva with normal saline is necessary to reduce infection and prevent adhesion. When oral mucositis is present, nasogastric feeding is recommended. (2) Glucocorticoid: Early high-dose systemic application of glucocorticoid can efficiently inhibit the inflammatory response. Multiple research studies have proven that glucocorticoid therapy can appreciably reduce the expected mortality of SJS sufferers, which makes it one of the systemic treatment options for SJS.
10
(3) Immunoglobulin: Immunoglobulin can block receptors and inhibit apoptosis. Studies have shown that intravenous administration of immunoglobulin combined with glucocorticoid can significantly decrease the risk of death in SJS sufferers, and the utility of immunoglobulin can reduce the dosage of glucocorticoid as well.
11
(4) Immunotherapy: Studies have shown that immunosuppressants such as cyclosporine A, cyclophosphamide, thalidomide, and TNF-α antagonist can be used to treat SJS.
12
This patient was treated with Etanercept, which is a TNF-α antagonist. It can shorten the time of epidermal restoration and contribute to the rapid management of the disease.
13
TNF-α antagonist can be used alone or in combination with glucocorticoid, and should be used as early as possible.
1
(5) Blood purification: Plasma exchange and hemoperfusion are generally used to treat SJS. Studies have shown that blood purification can relieve symptoms, prevent disease progression, and shorten disease course; they can be used as an alternative to traditional ineffective treatments.14,15
(6) Gene therapy: It is a new way to deal with SJS, and it can alternate the mechanism of action of drugs. Susceptible alleles screening can improve the prevention and prognosis of SJS and help provide targeted therapy.
16
(7) Traditional Chinese Medicine: Scutellaria, Coptis, and Phellodendri can inhibit allergic reactions. Tripterygium wilfordii and glycyrrhiza have hormone-like effects. Glucocorticoid combined with Wuweixiaodu Drink and HuanglianJiedu Decoction can remove heat and toxin and cool blood, which brings a better healing effect.
17
Summary
In the case, the lesions primarily involved the mucosa of the pharynx and larynx and conjunctiva without skin damage. This is an extremely rare case and typical SJS symptoms are absent. Due to its unexpected presentation, the patient first sought treatment in the otorhinolaryngology department. But for otolaryngologists, most of us have an inadequate perception of SJS and easily confuse it with throat infection and other common related diseases, resulting in misdiagnosis. The significance of this case report is to remind otolaryngologists that in the event of unexplained mucosal lesions or a poor effect of conventional treatment, we should not ignore systemic diseases, previous drugs, the history of drug allergies of the patient himself and his immediate family members, and atypical SJS should be suspected.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.