
Abstract

Significance Statement
Granulomatosis with polyangiitis (GPA), renamed from Wegener’s 10°years ago, is an autoimmune granulomatous systemic disease characterized by necrotic vasculitis. Although head and neck area is frequently affected, about 6% and 8% of patients present with hearing loss as initial symptom and facial nerve palsy due to middle ear pathology, respectively. Much rarer are vertigo and meningeal involvement. We present a clinical report that combines hearing loss, vertigo, facial nerve palsy, and irritation of meninx.
A 64-year-old woman was referred to our ear, nose, and throat (ENT) department with a 3-day history of right facial nerve (VII) palsy, along with a 4-month history of bilateral hearing loss, ear fullness and pain, tinnitus, vertigo, and about 15 kg weight loss. Antibiotics and corticosteroids, prescribed at the onset by a private practice doctor, temporarily attenuated the symptoms. Clinical examination showed right VII palsy (HouseBrackmann IV), without other neurological findings (Figure 1). Otomicroscopy revealed granular tissue at the right middle ear combined with otitis media and intact tympanic membrane (Figure 2A). Pure tone audiometry demonstrated severe bilateral mixed hearing loss. Blood test presented elevated inflammatory markers, namely, C-reactive protein (CRP) = 19.60 mg/dL, erythrocyte sedimentation rate (ESR) = 120 mm, and high white blood cell count (14.200/μL). Image showing right facial nerve palsy of the patient. (Α) Otomicroscopy image showing granular tissue at the right middle ear, combined with otitis media and intact tympanic membrane. (B) Histopathological examination from middle-ear lesions showing connective tissue with inflammatory infiltrates, mostly lymphocytic. Amongst evident areas of crash artefact, vague signs of granulomatosis formation can be noticed. At the top center of the sample, a multinucleated giant cell is evident (H&E, ×10). H&E indicates hematoxylin and eosin.
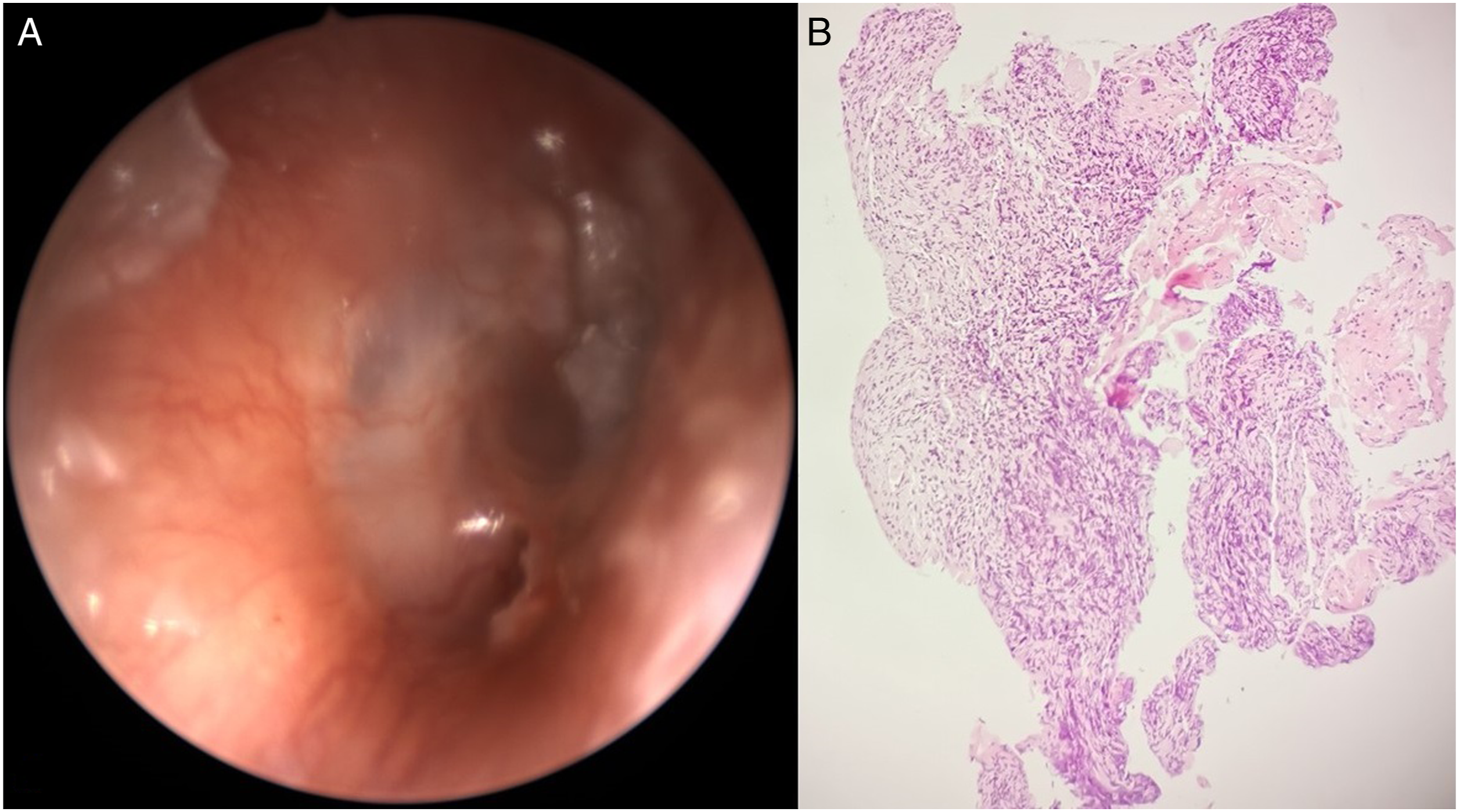
Brain, facial bones, skull base computed tomography (CT), and magnetic resonance imaging (MRI) were performed. Computed tomography showed right middle ear otitis with bone erosion of the anterior wall of epitympanum, which is in proximity to anterior facial nerve genu, osteosclerotic greater wing of right sphenoid bone, along with focal bone erosion (Figure 3A). Additionally, MRI revealed right temporal meningeal thickening—irritation of mater of the right epitympanum (Figure 3B). Chest CT showed solid, tuberous, and atelectatic lesions bilaterally (Figure 3C). Biopsies of the right middle ear lesions were taken, and were supportive of dense chronic inflammatory aggregates in granuloma resembling formations and the presence of a multinucleated giant cell (Figure 2B). All the above elements hinted the histology report towards granulomatous inflammation. Cytoplasmic antineutrophil cytoplasmic antibodies (c-ANCA) were 1:20 and ANCA-proteinase 3 (PR3), 112.3 units. A multidisciplinary approach was followed by rheumatologist, pulmonologist, pathologist, and neurologist. After study of imaging and immunological examinations, along with clinical and histopathological findings, diagnosis of GPA was confirmed. The patient took corticosteroids and immunosuppressants (methylprednisolone and cyclophosphamide), and blood test values were normalized 13°days later. She also mentioned improvement of vertigo and tinnitus. After 2 doses of cyclophosphamide, her hearing, along with VII palsy, improved eminently. Moreover, macroscopic evidence of disease at her middle ear could no longer be observed. At 6°months’ follow-up, she was in remission under regular surveillance from otolaryngologist and rheumatologist. (Α) Axial CT image of temporal bones showing opacification of right mastoid air cells (blue arrow), with bone erosion at epitympanum (green arrow). It also demonstrates osteosclerotic greater wing of the right sphenoid bone, along with focal bone erosion (yellow arrow). (B) MRI in the axial plane showing right temporal meningeal thickening (white arrow), indicative of meningeal irritation. (C) CT of lungs in an axial plane showing a radiopaque mass at the right lung (red arrows) along with scattered tuberous lesions bilaterally. CT indicates computed tomography; MRI indicates magnetic resonance imaging.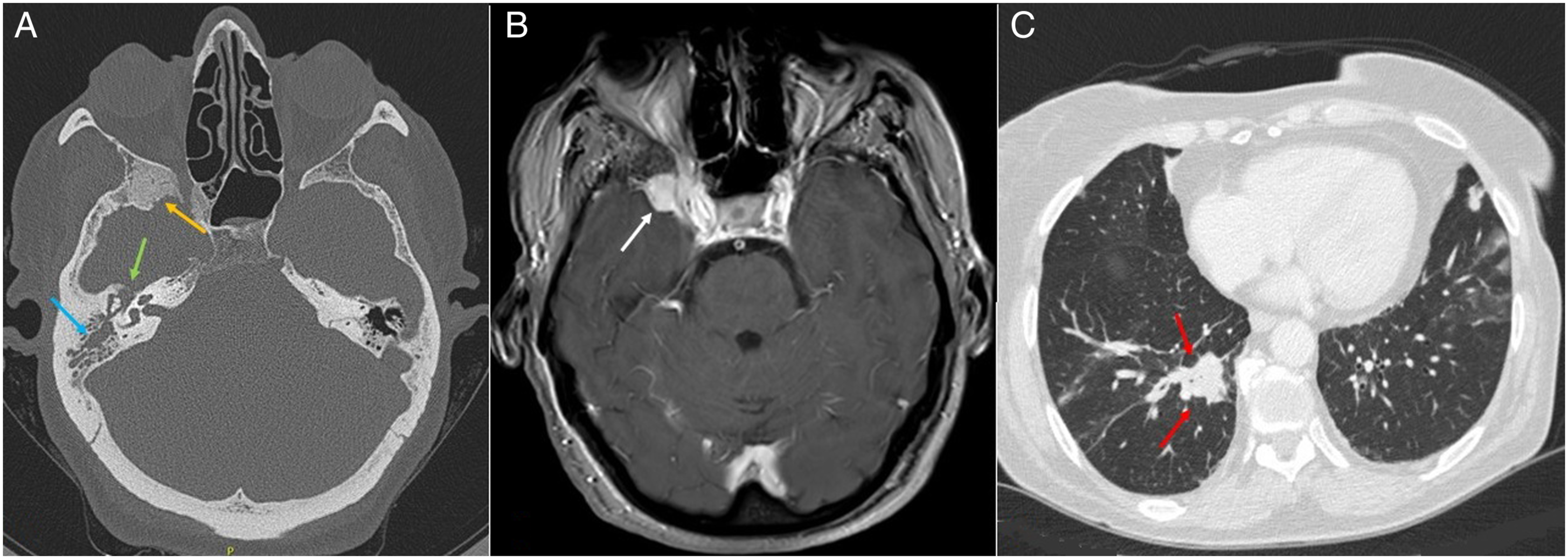
Granulomatosis with polyangiitis is an autoimmune multisystemic disease that affects mainly upper and lower respiratory tracts, as well as kidneys (glomerulonephritis), and is associated with the presence of ANCA. It is characterized by necrotizing granulomatous inflammation of small- to medium-sized vessels. It is divided into limited disease when only head and neck area is affected and generalized when upper, lower respiratory tract and kidneys are involved. 1 Concerning epidemiology, it mostly affects people between ages 45 and 60°years old and has interestingly higher prevalence in northern Europe compared to southern (150/million and 20/million, respectively). 2 About 70100% of cases of GPA involve the upper respiratory tract, and concerning the head and neck area, nasal cavity and paranasal sinuses are most frequently affected (85100%). Otological manifestations are present at about 1 out of 3 cases. 3 Other otolaryngological manifestations include oral cavity, trachea, larynx, and salivary glands. 4 The middle ear is affected by granulomatous inflammation at about 24%. Vertigo is infrequently described, and is attributed either to the vestibule autoimmune process or to central nervous system involvement. 5 Central nervous system manifestations are rare, about 213%. 6 Meningeal involvement is also rare (about 411%) due to either vasculitis of the area or spread of inflammation from adjacent structures, for instance, epitympanum as in our case. 7 Hearing loss is a common symptom (about 23%) for GPA, however it is much rarer as the initial symptom (6%). 6 Finally, about 8% of patients have VII palsy due to middle ear involvement. 8
In the revised Chapel Hill criteria (2012), it is clearly stated that it is not necessary for granulomatous inflammation to be histologically diagnosed, and non-invasive methods could also diagnose. 9 Obviously, histopathology is the cornerstone of definite diagnosis, but in some cases, ANCA or anti-PR3 positivity along with clinical suspicion and examination evidence are enough to start treatment.2,9
Differential diagnosis includes ChurgStrauss syndrome, sarcoidosis, tuberculosis, malignancy, and infectious diseases. 6
Concerning treatment, an induction and a maintenance phase have been proposed, with the former including corticosteroids and immunosuppressants (duration, 36 months) and the latter, a combination of corticosteroids and supplementary methotrexate or azathioprine (duration, 1224 months). 4 If left without treatment, GPA is almost always fatal, whereas if treated properly, the 10-year survival rate is about 80%. Relapse is frequent, and in over 50% of patients, it happens within 5°years from diagnosis. 2
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
We declare that written informed consent for patient information and images to be published was provided by the patient.