
Abstract
Pulsatile tinnitus is a rhythmic type of tinnitus. Most cases are caused by vascular disorders and present as synchronous with the patient’s heartbeat. A dilated mastoid emissary vein may cause pulsatile tinnitus. Here, we report the first case of bilateral pulsatile tinnitus caused by dilated bilateral mastoid emissary vein. The patient suffered from bilateral pulsatile tinnitus for 2 years. His bilateral tinnitus disappeared temporarily when the bilateral mastoid processes were compressed. Temporal bone computed tomographic (CT) showed the bilateral dilated mastoid emissary canals. Cranial Magnetic resonance venograms (MRV) showed the bilateral dilated mastoid emissary veins. We explained the risk of surgery to the patient. Because the patient could tolerate his tinnitus and did not have a hemangioma or tumor, he did not choose to undergo surgery.
Introduction
Pulsatile tinnitus is a rhythmic type of tinnitus. Most cases are caused by vascular disorders and present as synchronous with the patient’s heartbeat. Pulsatile tinnitus associated with venous lesions is the most common type. Causes include transverse sinus stenosis, sigmoid sinus diverticulum, sigmoid sinus dehiscence, high riding or dehiscent jugular bulbs, and dilated mastoid emissary veins. 1 Here in, we report the first case of bilateral pulsatile tinnitus caused by dilated bilateral mastoid emissary vein.
Case Study
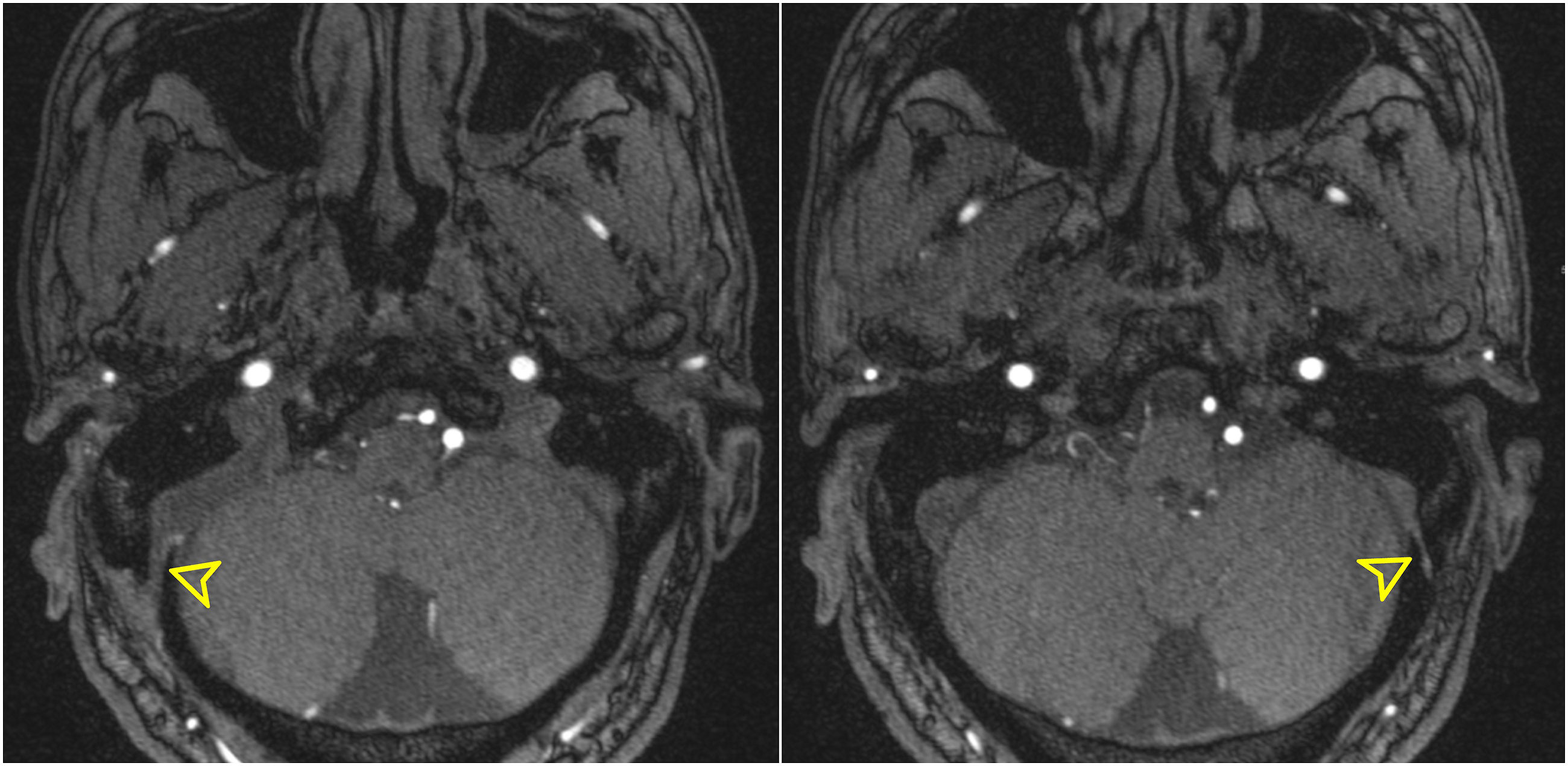
A 61-year-old male patient sought medical attention at the otolaryngology department for bilateral pulsatile tinnitus lasting 2 years. The patient said the bilateral tinnitus was more pronounced in the right ear and tinnitus was both persistent and synchronous with heartbeat. Tinnitus was more pronounced in quiet environments and after strenuous exercise. Bilateral tinnitus did not weaken or disappear when bilateral neck blood vessels were compressed. However, bilateral tinnitus did disappear temporarily when the bilateral mastoid processes were compressed. Sounds that were consistent with the heartbeat could be heard upon auscultation of bilateral mastoid processes. Otoscopic examination showed that bilateral external auditory canals were patent, bilateral tympanum was intact, and light transmission was good. There were no space-occupying lesions in the tympanic cavity. Temporal bone CT showed the bilateral dilated mastoid emissary canals (Figure 1). The diameters of the patient’s right and left mastoid emissary canals were 4 mm and 2.6 mm, respectively. Cranial MRV showed the bilateral dilated mastoid emissary veins (Figure 2). We explained the risk of surgery to the patient. Because the patient could tolerate his tinnitus and did not have a hemangioma or tumor, he did not choose to undergo surgery.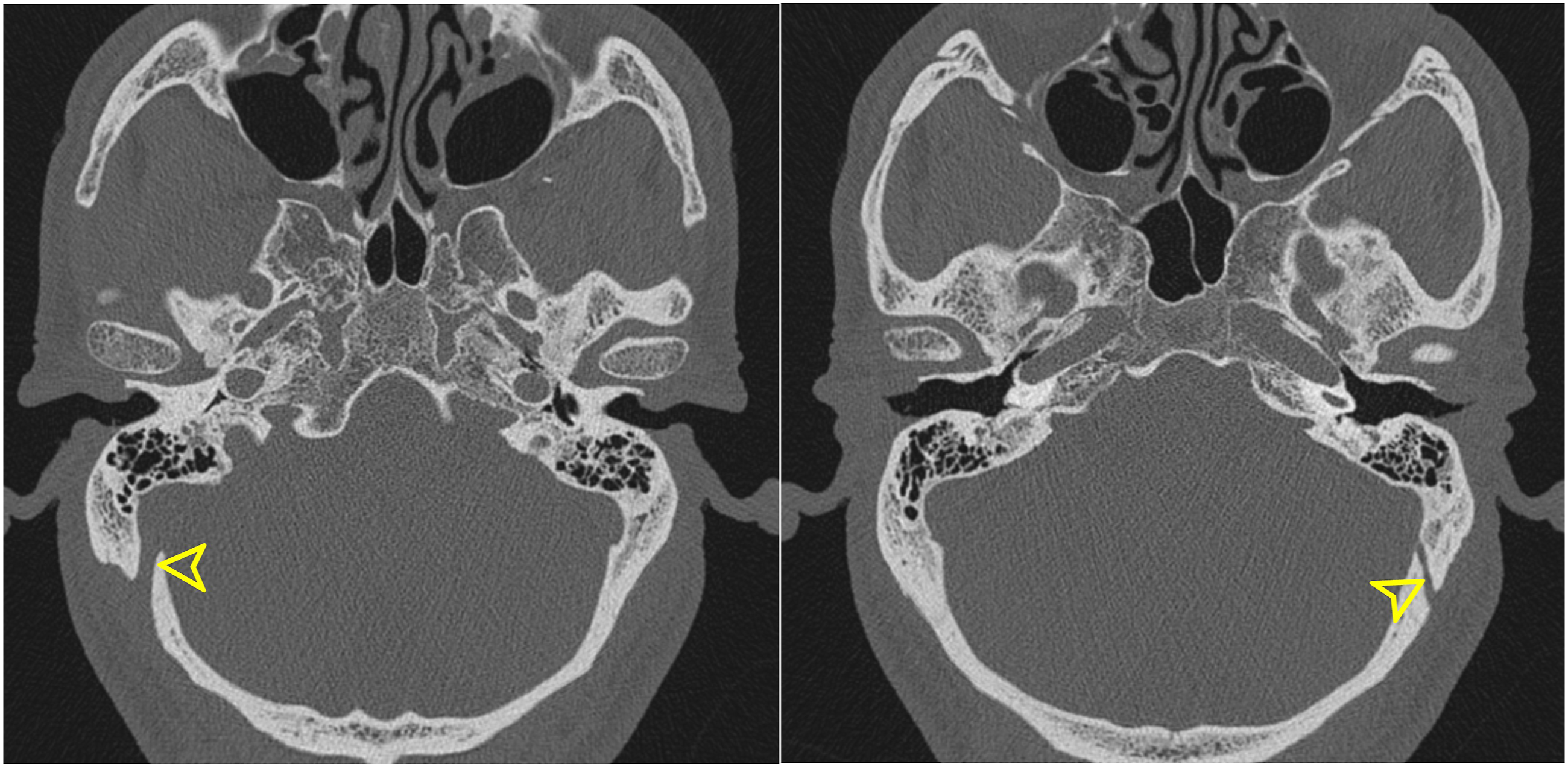
Discussion
The mastoid emissary vein is located in the mastoid emissary canal and communicated with the sigmoid sinus and suboccipital venous plexus. Because of the absence of valves, blood flow is bidirectional. Under normal conditions, blood flows inward toward the sigmoid sinus. 2 If the sigmoid sinus drainage is blocked or intracranial pressure is high, blood in the intracranial venous sinuses can flow outward to the vertebral venous plexus. Demirpolat et al performed CT scans of 248 patients and found that mastoid emissary canals were present in 92.3% of patients. The average diameters of these right and left mastoid emissary canals were 1.58 ± .86 mm and 1.48 ± .79 mm, respectively. The proportion of mastoid emissary canals with diameter >3 mm accounted for under 5% of cases. 3 Tsutsumi et al 4 performed MRV examination on 96 patients and found mastoid emissary veins to be present in 89.5% of patients, and 59.3% of patients had bilateral mastoid emissary veins. There are still no unified criteria for mastoid emissary vein dilation and the cause of dilation is still unknown. Intracranial hypertension, high-flow vascular malformations, and jugular vein hypoplasia may be associated with mastoid emissary vein dilation. 5
In extremely rare cases, a dilated mastoid emissary vein may cause pulsatile tinnitus synchronous with the patient’s heartbeat. This is generally considered to be due to the transmission of increased blood flow sounds to the ear through the mastoid process. This disease is characterized by temporary weakening or disappearance of tinnitus when the mastoid process behind the ear is compressed. Dilation of the mastoid emissary canal can be seen on temporal bone CT and the inward course of the mastoid emissary vein can be seen on cranial MRV. Treatments for pulsatile tinnitus caused by dilated mastoid emissary vein include endovascular embolization and vascular ligation. We carefully reviewed the literature and found that only 4 cases in English-language reports showed explicitly the cause of pulsatile tinnitus to be dilated mastoid emissary vein. All patients in these studies were female and all had unilateral pulsatile tinnitus, with 2 each having left and right pulsatile tinnitus. The diameters of the mastoid emissary vein were 2.5 mm, 4.5 mm, 5 mm, and 7.5 mm.6 -9 Of these, 2 patients underwent surgery, 1 underwent endovascular coiling, and 1 underwent ligation, and all achieved good outcomes. Our patient is the first case of bilateral pulsatile tinnitus caused by dilated bilateral mastoid emissary vein and is the first male patient. The diameters of our patient’s right and left mastoid emissary canals were 4 mm and 2.6 mm, respectively.
Conclusions
Pulsatile tinnitus caused by dilated bilateral mastoid emissary vein is extremely rare. The possibility of dilated bilateral mastoid emissary vein should be considered if pulsatile tinnitus weakens or disappears when the mastoid process is compressed and temporal bone CT and cranial MRV can be used for diagnosis. Satisfactory treatment outcomes can be achieved through surgery for patients who cannot tolerate tinnitus.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.