
Abstract
Cricotracheostomy is a useful surgical procedure for opening the airway in cases where conventional tracheotomy is difficult. This is a safe and easy technique involving removal of the anterior portion of the cricoid cartilage. Herein, we report the case of a patient with difficulty in neck extension due to severe kyphosis, who underwent cricotracheostomy. A 65-year-old woman developed dyspnea and was transported to our hospital. SpO2 was 60% (room air) and endotracheal intubation was performed. She was managed on ventilator. However, weaning off the ventilator was difficult, and endotracheal intubation was prolonged. Subsequently, the patient was referred to us for a tracheostomy. The patient was unable to maintain the supine position due to severe kyphosis, and computed tomography revealed that the brachiocephalic artery was running just below the thyroid gland. Therefore, conventional tracheostomy was difficult to perform, and we performed cricotracheostomy instead. After the cricotracheostomy, there were no tracheal problems, such as tracheal stenosis and stomal hemorrhage. Cricotracheostomy can be performed in cases where multiple anatomical difficulties may be faced in the tracheostomy site, as in this case. Furthermore, cricotracheostomy is beneficial for long-term airway management because it causes fewer complications compared to conventional tracheotomy.
Introduction
Conventional tracheostomy is classified as high, middle, or low, depending on the cervical features, such as the size of the thyroid gland and neck extension.1,2 In general, low tracheostomy is recommended for placing a stoma between the second and fourth tracheal rings because of its lower complication rates compared to other techniques. High tracheostomy more frequently results in the surgical site granulation 3 and tracheostomy stenosis.4,5 Further, middle tracheostomy more frequently results in hemostasis from the resected thyroid gland than low tracheostomy. 6 However, low tracheostomy is sometimes difficult in patients with anatomical features like high brachiocephalic artery, short neck, and poor neck extension, and those with obesity and thyroid disease. Patients with these features have a higher risk of intraoperative and postoperative complications. 7 Cricotracheostomy is a useful surgical procedure for cases where performing conventional tracheotomy is difficult. In this article, we report the case of a patient with severe kyphosis due to repeated compression fractures of the spine, and with difficulty in neck extension, who underwent cricotracheostomy. Cricotracheostomy allowed the development of tracheostomy easily and safely, without intra- and postoperative complications, in this case.
Case report
A 65-year-old woman developed dyspnea 1 week before presenting to our hospital. She experienced exacerbation of dyspnea and was transported to our hospital by an ambulance. Her medical history included severe kyphosis due to repeated compression fracture of the spine, osteoporosis, rheumatoid arthritis, and Werner’s syndrome (suspected). Her height was 154 cm, and body weight was 32 kg. Her body temperature was 36.1°C, SpO2 was 60% (room air), and respiratory rate was 30/min. The external jugular vein was distended, and right ventricular failure was suspected. Arterial blood gas analysis (face mask O2 10 L/min) showed PaO2 42.9 Torr, PaCO2 75.7 Torr, and HCO3- 22.0 Torr, which indicated type 2 respiratory failure. Chest computed tomography (CT) revealed bilateral pleural effusion.
She was diagnosed with type 2 respiratory failure caused by pleural effusion associated with right ventricular failure. Emergency doctors performed endotracheal intubation and ventilator management. Right ventricular failure and pleural effusions gradually improved with intensive care provided by internal medicine doctors. However, weaning off the ventilator was difficult, and endotracheal intubation was prolonged. The patient was then referred to us for a tracheostomy. On physical examination, the patient was unable to maintain the supine position due to severe kyphosis and was unable to extend her neck (Figure 1A, 1B and 1C). Furthermore, CT revealed that the brachiocephalic artery was running just below the thyroid gland (Figure 1D). Consequently, we concluded that conventional tracheostomy was difficult, and cricotracheostomy was preferable in this case; the procedure was performed 20 days after intubation. Physical findings and CT imaging. A. Thoracic deformity was severe (arrow). B. and C. Severe kyphosis (arrowhead) and thoracic deformity (arrow). D. Brachiocephalic artery (*) was running just below the thyroid gland (T).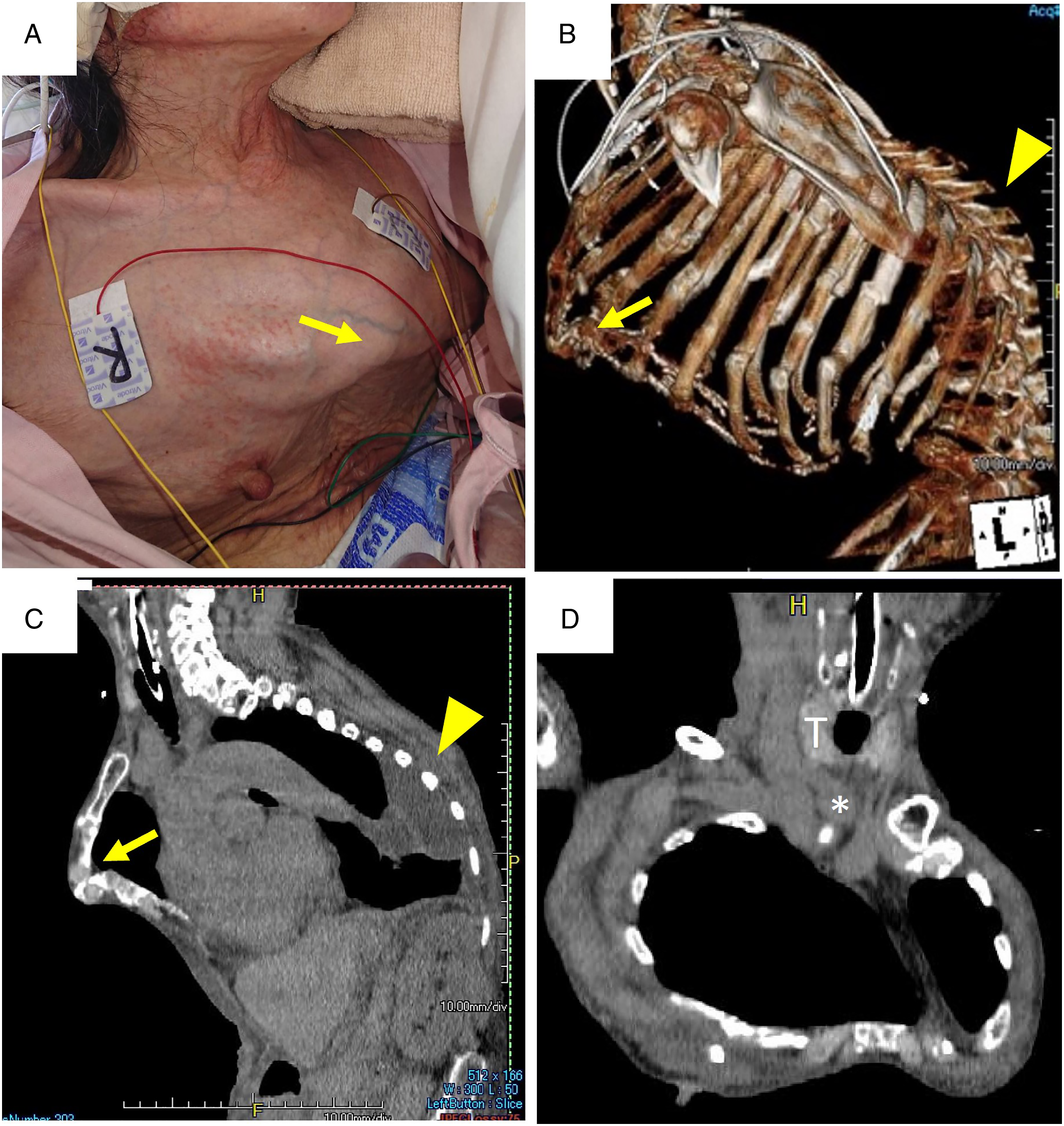
Surgical procedure
Cricotracheostomy was performed under general anesthesia. The patient’s neck floated due to severe kyphosis, even though we inserted a shoulder pillow. Several preparations were needed to obtain the supine position, such as bed rotation and a stabilizing device. A 5-cm vertical skin incision was made in the midline over the cricoid cartilage (Figure 2A). Bilateral sternohyoid muscles were divided and pulled laterally to identify the cricoid cartilage. The cricothyroid muscle was removed to expose the surface of cricoid cartilage. The anterior portion of the cricoid cartilage was removed, and the perichondrium was preserved using reul forceps. The perichondrium of the cricoid cartilage and cricothyroid membrane was incised using an I-shaped incision (Figure 2B). Finally, the perichondrial flaps were sutured to the skin (Figure 2C and 2D). Operative procedure of cricotracheostomy. A. A vertical skin incision was made over the cricoid cartilage (dotted line). B. The anterior portion of the cricoid cartilage was removed, and the perichondrium of the cricoid cartilage and cricothyroid membrane was incised using an I-shaped incision (solid line). C. The perichondrial flaps were sutured to the skin. D. The incised skin was sutured to create a tracheal stoma.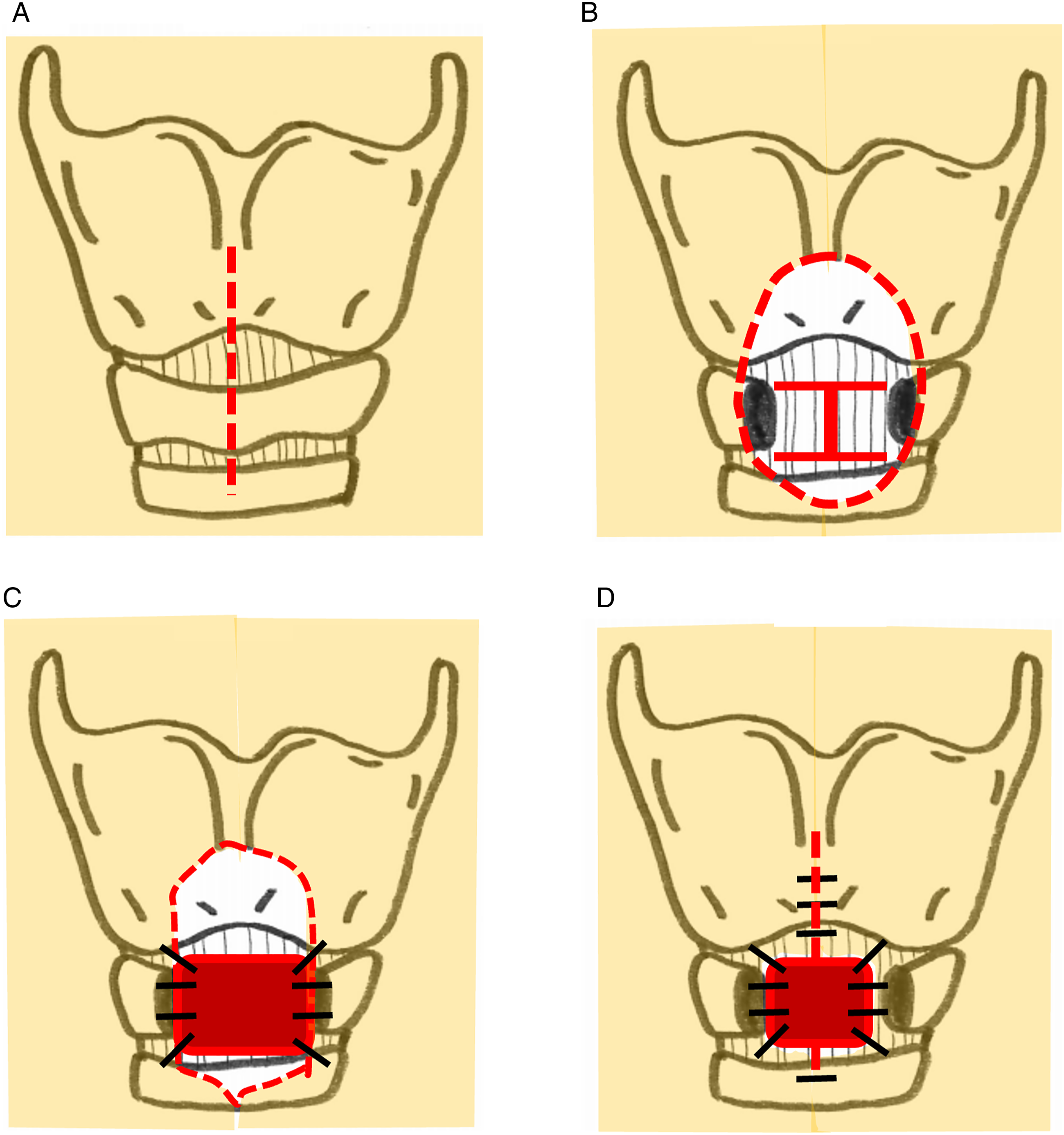
Postoperative course
No bleeding or infection was observed. The tracheostomy cannula could be easily replaced on postoperative day (POD) 8. The patient was weaned and released from the ventilator on POD 12. A speech cannula was inserted on POD 19. The patient was doing well and was able to take a meal orally on POD 34. No tracheal problems were observed, and the patient was transferred to a convalescent hospital on POD 44. Verbal informed consent was obtained from the patient for anonymized information to be published in this article.
Discussion
In the present case, conventional tracheostomy was considered difficult because of severe kyphosis and difficulty in neck extension. In addition, the brachiocephalic artery ran just below the thyroid gland, and the cricoid cartilage was barely palpable above the clavicle. Cricotracheostomy, as reported by Kano et al, 1 involves removing the anterior portion of the cricoid cartilage and creating a stoma at a high level. This surgery is especially useful in case of a short neck, where the trachea is hidden in the mediastinum and the cricoid cartilage is palpated just above the sternum. Furthermore, in case of short neck, intraoperative bleeding around the thyroid gland makes it difficult to maintain a clear surgical field, but cricotracheostomy rarely causes bleeding from the perithyroid gland. 1 Furthermore, cricotracheostomy is associated with fewer complications in long-term airway management. Kano et al. 3 reported 57 cases that involved cricotracheostomy, and long-term postoperative complications were not reported in any of them. However, there is a problem associated with cricotracheostomy in that the stoma is not completely closed just by removing the cannula. Kano et al. 1 reported that stoma closure was performed in three of seven patients who underwent cricotracheostomy, and no complications were observed after surgery.
In the present case, long-term postoperative cannula management was expected. If we chose the conventional tracheostomy (i.e., high, middle, and low) for such a short neck, there would have been a higher risk of surgical complications. As for a high tracheostomy, the movement of a cannula is likely to cause inflammation of the cricoid cartilage and compression necrosis of the luminal mucosa, resulting in long-term tracheal stenosis.8,9 Middle tracheostomy causes hemorrhage of the resected thyroid, and insufficient hemostasis may cause critical postoperative bleeding. 10 In low tracheostomy, the curved part of the cannula easily presses the first tracheal ring and the cricoid cartilage. The cartilage easily undergoes ischemic necrosis, resulting in tracheal stenosis. 11 The complication rate of conventional tracheostomy is reported to be about 6–58%.6,7 Japhet et al. 12 reported that complications related to conventional tracheostomy were seen in 46 of 214 patients (21.5%). Tracheal stenosis can be found in 31–85% of patients,13,14 and stomal hemorrhage was seen in 36%. 13 In our case, no tracheal stenosis or stomal hemorrhage was observed until the patient was transferred to the convalescent hospital on POD 44.
This case report has several limitations. First, the patient was transferred to the convalescent hospital on POD 44; therefore, the long-term postoperative course is unknown. There is a possibility that this patient did not need to undergo cricotracheostomy to wean off the ventilator if intubation was continued. However, we believe it was appropriate to perform a cricotracheostomy to prevent ventilator-associated pneumonia because endotracheal intubation had been prolonged for 20 days.
In the present case, we performed cricotracheostomy in a patient for whom conventional tracheostomy was difficult due to severe kyphosis. Cricotracheostomy might be a useful procedure in such cases.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was conducted with the approval of the Clinical Research Ethics Review Committee of Kawasaki Municipal Kawasaki Hospital (Approval No.: 2019-29).
Statement of Human and Animal Rights
All procedures performed in this study were in accordance with the 1964 Helsinki declaration and its later amendments.