
Abstract

Significance statement
Primary melanocytic tumors of the central nervous system (CNS) are rare, and optimal treatment is unknown. Here, we present a case of a patient with intermediate-grade melanocytic neoplasm of the cerebellopontine angle (CPA) who underwent subtotal resection and adjuvant radiation therapy. These lesions have a high rate of regrowth and recurrence with associated high mortality. Management should include total resection if possible, with consideration of adjuvant radiation therapy, particularly in cases of incomplete resection.
Report of a case
An obese 33-year-old female presented with 1 year of disequilibrium, hearing loss, and morning headaches. Magnetic resonance imaging (MRI) revealed a 4.5-cm irregularly shaped right CPA mass, compressing the brainstem and cerebellum, and extending into the jugular foramen. The mass was mildly hyper-intense to brain on T1- and iso-intense on T2-weighted images with homogenous enhancement with gadolinium contrast (Figure 1A-C), suspicious for meningioma or schwannoma. Audiologic testing revealed a right unilateral profound sensorineural hearing loss. MRI revealed a 4.5-cm right CPA mass with brainstem compression. The mass was mildly hyper-intense on T1-weighted images (A), iso-intense on T2-weighted images (B), and enhanced homogenously with gadolinium contrast (C). CPA, cerebellopontine angle.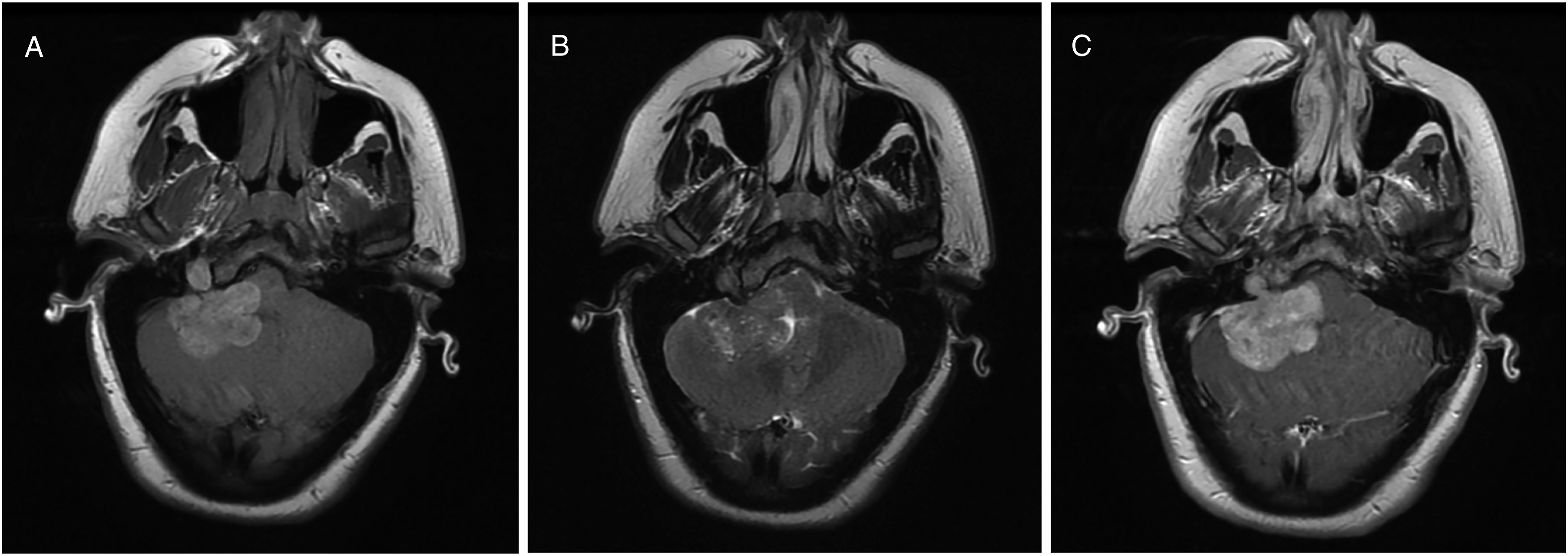
A subtotal resection was performed via retrosigmoid craniotomy, leaving the jugular foramen component to protect the lower cranial nerves with successful preservation of facial nerve function. The tumor was noted to be black, vascular, and adherent to the brainstem (Figure 2). Intra-operative images. A large, vascular, melanocytic mass was visualized via retrosigmoid approach at the CPA (A). Residual tumor at the jugular foramen was left to protect the lower cranial nerves (B). CPA, cerebellopontine angle.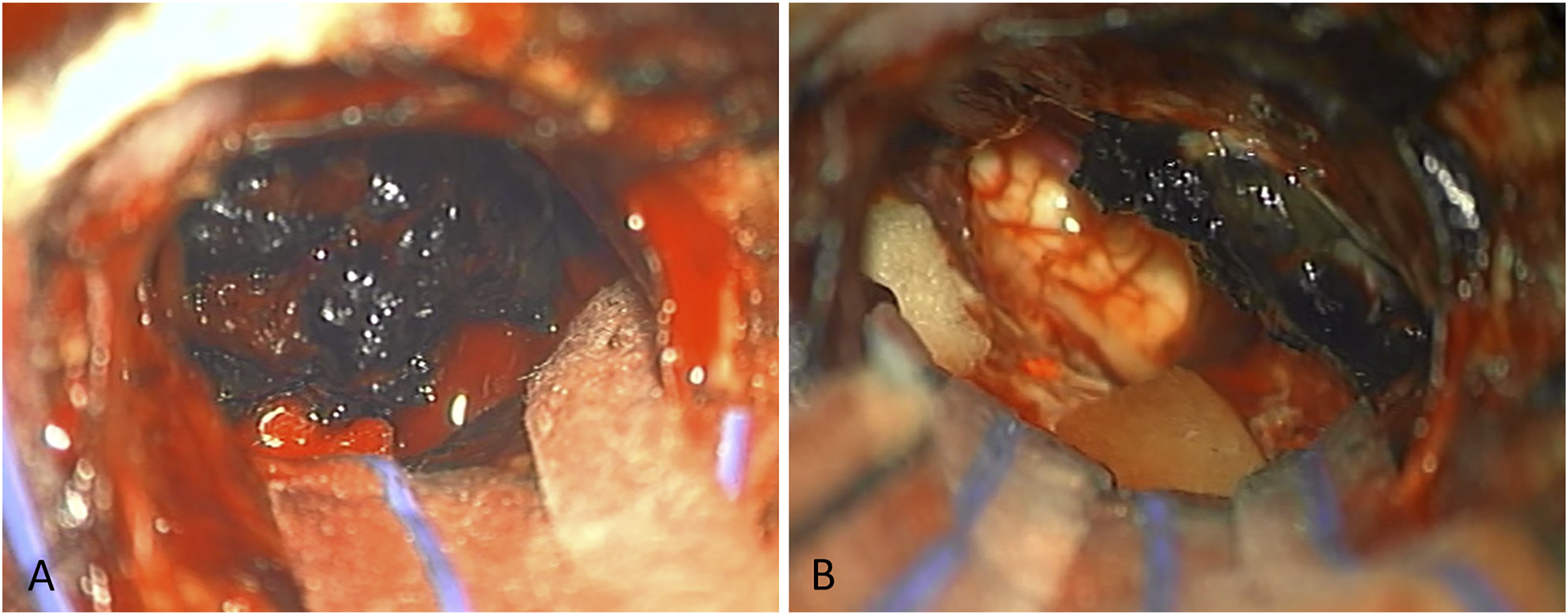
Histology demonstrated pigmented spindle cells arranged in fascicles, which stained diffusely positive for S-100, SOX10, HMB-45, and Melan-A (Figure 3A-D). Ki67 demonstrated focal mild-moderate increased proliferation with few mitotic figures. The diagnosis was intermediate-grade primary melanocytic neoplasm. Next-generation sequencing panel failed due to insufficient amplifiable DNA. Thus, the lesion was unable to be more specifically characterized. The tumor cells stained positive for S-100 (A), SOX10 (B), HMB-45 (C), and Melan-A (D) (Magnification 400x).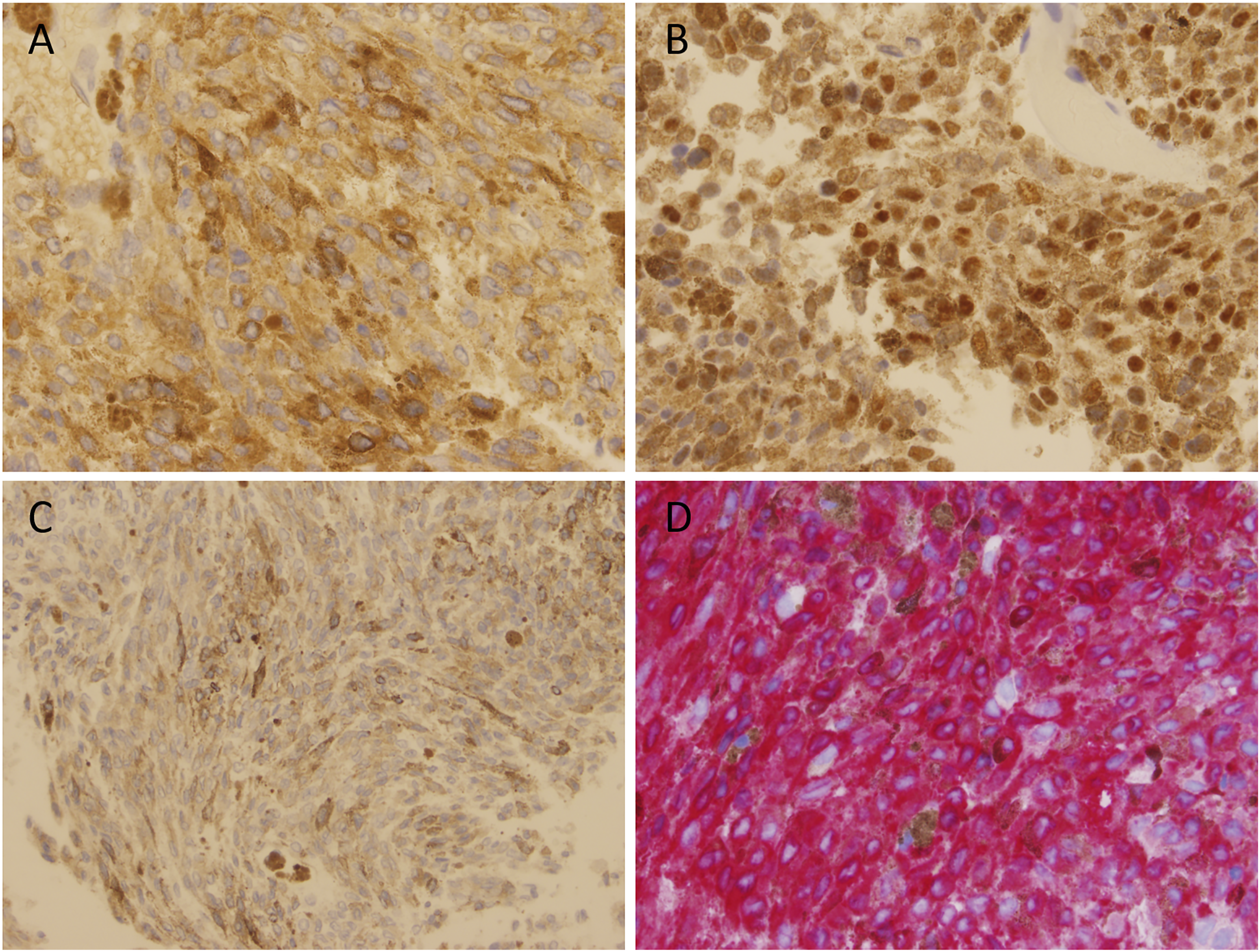
The patient completed 30 rounds of intensity-modulated radiation therapy. Surveillance imaging has shown no interval growth of the tumor at 10 months after tumor resection.
Discussion
Tumors of the CPA comprise only 10% of all intracranial neoplasms, of which the majority (70-90%) are schwannomas, followed by meningiomas (approximately 10%). 1 Pigmented lesions account for a much smaller subset of CNS tumors, yet the differential remains broad. This includes melanocytic neoplasms, melanotic schwannoma, melanotic medulloblastoma, melanotic neuro-ectodermal tumor of infancy, pigmented glial/ependymal or choroid plexus tumors, and teratoma. 2
Primary meningeal melanocytomas of the CNS are very rare, with a reported incidence of approximately 1 per 10 million 3 and few reports globally of primary melanocytic tumors in the CPA.3-10 The diagnosis is challenging, as these lesions may present similar to the more common schwannomas and meningiomas. Radiologic findings and even histopathologic analysis are often not definitive.2,4,9,11 Optimal therapy remains unknown. Here, we report a case of a primary melanocytic CPA tumor that was managed with subtotal resection and adjuvant radiation therapy.
Melanocytic neoplasms exist along a spectrum of disease from benign to malignant: primary meningeal melanocytoma to melanoma. Melanocytomas are slow-growing benign neoplasms arising from leptomeningeal melanocytes. Primary melanoma of the CNS occurs most commonly in the spinal cord and posterior fossa, with variable prognosis. Definitive classification of primary melanocytic neoplasms of the CNS can be difficult, and tumors with some but not all features of a melanoma are classified as intermediate-grade melanocytic neoplasms.2,3,12 On histopathology, primary melanocytic neoplasms stain positive for S-100, SOX10, and HMB-45.8,13
Within the CPA, metastasis of a cutaneous melanoma is much more common than a primary melanocytic neoplasm. While it is often impossible to distinguish metastatic from primary CNS melanoma histopathologically, targeted next-generation sequencing has been used successfully.10,14 Primary melanocytic neoplasms of the CNS demonstrate consistent mutations in GNAQ (71%) and GNA11 (12%), while other mutations more commonly found in cutaneous or uveal melanomas such as NRAS or BRAF are rare. 15
Imaging is of limited utility in distinguishing melanocytic lesions from other lesions of the CPA. Meningiomas have widely variable intensity on both T1- and T2-weighted images. Intra-lesional calcifications lead to heterogeneous enhancement with gadolinium contrast. Schwannomas are typically hypo-intense or iso-intense on T1- and hyper- to iso-intense on T2-weighted images. They may have heterogenous enhancement with gadolinium contrast when cystic degeneration has occurred. 16 Melanocytic lesions of the CNS are typically hyper-intense on T1- and hypo- to iso-intense on T2-weighted images. They enhance homogenously with gadolinium contrast. 4 In all cases, MRI characteristics may vary depending on the degree of melanization. 9
Prior small case series have recommended complete surgical resection with adjuvant radiation therapy, particularly in cases of incomplete resection. Recurrence occurs at a rate of 38% in 5 years after complete resection alone, 3 while 80% of subtotal resections had progression or death within 12 months of diagnosis. 4 There have been reports of the use of gamma knife radiosurgery with overall promising results after incomplete resection.3,9,17 Data is lacking regarding the role of chemotherapy in this disease. 3
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.