
Abstract
Objectives:
This study compared the rate of graft success, as well as hearing improvement and dry ear time between dry ears and wet ears with otomycosis or without otomycosis in patients with chronic suppurative otitis media (CSOM) after endoscopic cartilage myringoplasty.
Methods:
This retrospective study was conducted in a tertiary hospital in Shanghai. In total, 83 patients with CSOM (43 with dry ears and 40 with wet ears) were included. Among the 40 patients with CSOM and wet ears, 25 exhibited otomycosis. All patients underwent endoscopic myringoplasty, and perforations were repaired using tragal cartilage with a single-sided perichondrium. Patients were followed up for at least 6 months. Pure-tone hearing was examined preoperatively and at 3 months postoperatively. The graft uptake rate, hearing improvement, and dry ear time were compared between the groups.
Results:
The graft success rate did not differ significantly between the dry-ear and wet-ear groups (95.35% and 90.00%, respectively). Furthermore, the graft success rate also did not differ significantly between patients with wet ears and otomycosis and those with wet ears without otomycosis (92.00% and 86.67%, respectively). Hearing gain did not differ significantly between the dry-ear and wet-ear groups. No significant difference in hearing gain was also found in patients with wet ears with or without otomycosis. However, the time to dry ear was significantly longer in the wet-ear group than in the dry-ear group.
Conclusion:
Patients with CSOM and wet ears required more time to achieve a completely healthy status. However, the graft success rate and hearing improvement were not affected by a wet middle ear and otomycosis. Thus, endoscopic myringoplasty using tragus cartilage is an effective treatment for refractory CSOM in patients with wet ears and otomycosis.
Introduction
Chronic suppurative otitis media (CSOM) is characterized by repeated otorrhea through perforated tympanic membrane. Chronic suppurative otitis media often leads to conductive hearing loss. Myringoplasty is the standard, well-established procedure for closure of tympanic membrane perforations. Typically, ears that have been dry for at least 3 months are presumed to be most suitable for myringoplasty. Active ear discharge is considered a contraindication for myringoplasty due to the widespread belief that this discharge causes graft rejection. To avoid graft failure, a course of antibiotic ear drops is often administered, and the ear is allowed to become dry before surgery. However, for some patients with recurrent CSOM, extensive use of topical antibiotic ear drops and steroids can lead to otomycosis or multidrug-resistant bacterial infection, eventually resulting in refractory CSOM. Some studies have found that the effectiveness of myringoplasty is not affected by the presence of ear discharge during surgery.1-5 Otomycosis is a superficial fungal infection of the external auditory canal and is particularly frequent in hot and humid regions. It remains controversial whether patients with CSOM and otomycosis are good candidates for surgery. Some studies have found that fungal infections are common in patients with CSOM.6-8 One study showed that external auditory canal status was an important factor affecting the success of myringoplasty. 9 To determine whether actively discharging ears (ie, wet ears) and otomycosis in patients with CSOM were suitable for myringoplasty, this retrospective study compared the treatment efficacy, hearing improvement, and dry ear time after endoscopic cartilage myringoplasty surgery between dry ears and wet ears with otomycosis or without otomycosis in patients with CSOM.
Materials and Methods
This retrospective study was conducted in a tertiary hospital in Shanghai (China) from January to December 2019. Two groups of patients with CSOM were selected according to their clinical status at the time of surgery: those with dry ears and those with wet ears. Each selected patient met the following inclusion criteria: (1) age ≥16 years, (2) tympanic membrane perforation caused by otitis media, (3) endoscopic myringoplasty (over-underlay technique) using cartilage with a single-sided perichondrium, (4) primary ear surgery, and (5) at least follow-up duration of 6 months. The exclusion criteria were (1) ossicular chain abnormalities, (2) cholesteatoma, and (3) revision surgery. Preoperative temporal high-resolution computer tomography (HRCT) was performed in all patients to exclude ossicular chain abnormalities and cholesteatoma. Diffusion-weighted magnetic resonance imaging was done when cholesteatoma could not be excluded by HRCT.
Patients with mucoid or mucopurulent discharge or only edematous middle ear mucosa were considered wet ears, as described in a previous study. 10 Meanwhile, patients with both wet middle ear and otomycosis belonged to the wet-ear group in our study. The discharge sampled at 1 day preoperatively was cultured to identify the causative pathogens. Patient age, patient sex, perforation size and site, opposite ear status (unilateral/bilateral CSOM), and preoperative hearing level were recorded. The tympanic membrane perforation less than 1 quadrant of the tympanic membrane is considered as small perforation; perforation of tympanic membrane between 1 and 2 quadrants is considered medium perforation and more than 3 quadrants of the tympanic membrane is considered large. The perforation locations were classified as anterior, posterior, or central. Air–bone conduction pure-tone threshold at 500, 1000, 2000, and 4000 Hz was performed in all patients both preoperatively and at 3 months postoperatively. The results were used to calculate the mean air–bone gap (ABG). Unhealed tympanic membrane, reperforation of the graft, and persistent ear discharge at 6 months postoperatively were considered to indicate graft failure.
Surgical Technique
All surgeries were performed by an experienced surgeon who has focused on the ear surgery for 10 years and completed more than 200 endoscopic tympanoplasty cases each year. The ear canal and middle ear cavity were irrigated 3 times with povidone-iodine (5 minutes each time) after general anesthesia induction and before the initiation of surgery. The perforation margin was treated for fresh wounds with an angled knife. For the right ear, this incision was made 5 mm posteriorly from the tympanic annulus and extended from the 1 o’clock to the 6 o’clock position. For the left ear, an incision was and extended from the 11 o’clock to the 6 o’clock position. Then, the tympanomeatal flap was gently elevated to the level of the fibrous annulus. Residual tympanic membrane was removed from the malleus handle. The mobility of ossicular chain was checked. Tragal cartilage was harvested with a single-sided perichondrium. The autograft was placed on the inner surface of the residual tympanic membrane, lateral to the malleus. A notch was made in the cartilage to accommodate the malleus handle. Gelfoam was placed in the middle ear cavity to prevent the graft collapse. The tympanomeatal flap was subsequently returned to its original position. The external ear canal was packed with Gelfoam and antibiotic-soaked gauze up to the tragus incision. The tragus incision was then sutured. Patients were discharged on postoperative day 2.
Postoperative Follow-Up
The packing gauze soaked in antibiotic ointment was removed from the external auditory canal on postoperative day 2. Any remaining Gelfoam fragments were aspirated from the external auditory canal at 2 weeks postoperatively if they had not broken down, thus allowing the graft to be visualized. All patients were followed up in our outpatient clinic at 2 weeks, 1 month, 3 months, and 6 months postoperatively. Graft status and the time to dry ear were recorded during endoscopic examinations. Pure-tone hearing was examined preoperatively and at 3 months postoperatively. Complete healing of the tympanic membrane graft at least 6 months postoperatively was considered successful. Graft success and hearing improvement rates were compared between the 2 groups.
Statistical Analysis
All categorical data were compared between groups using the χ2 test. Quantitative data with a normal distribution were analyzed using a t test .Quantitative data with a non-normal distribution were analyzed using the Mann-Whitney U test. Paired t tests were used to compare preoperative and postoperative pure-tone audiometry values within groups. The P value <.05 was the threshold for statistical significance.
Results
In total, 83 patients were enrolled in this study (43 in the dry-ear group and 40 in the wet-ear group). The dry-ear group comprised 31 women and 12 men (mean age, 46 ± 12.67 years), whereas the wet-ear group comprised 26 women and 14 men (mean age, 44.3 ± 14.48 years). The duration of illness was 12.68 ± 15.63 years in the dry-ear group and 12.75 ± 14.13 years in the wet-ear group. Most patients (18 in the dry-ear group and 23 in the wet-ear group) had medium-sized perforations. Perforations were most commonly centrally located (21 patients in the dry-ear group and 23 patients in the wet-ear group). Table 1 summarizes the detailed patient characteristics. There were no significant differences in age, sex, duration of illness, smoking history, perforation size, or perforation position between the 2 groups (P > .05). Twenty-five patients in the wet-ear group were diagnosed with CSOM and otomycosis, based on their clinical symptoms and signs. Fungi were identified in 25 patients, consistent with their clinical manifestations. Bacteria were identified in 16 patients. Four patients had mixed fungal and bacterial infections. No fungi or bacteria were observed in the ears of 3 patients. The most common fungi were Aspergillus niger and Candida albicans. The most common bacteria were Staphylococcus aureus and Pseudomonas aeruginosa (Table 2).
Patients’ Characters.
Abbreviations: F, female; M, male.
Distribution of All Isolated Organism.
The graft success rate was 95.35% for the dry-ear group (2 patients with graft failure) and 90.00% for the wet-ear group (4 patients with graft failure; Table 3). These rates did not differ significantly. In the wet-ear group, 25 patients exhibited otomycosis. The graft success rate was 92.00% (23/25) for patients with wet ears and otomycosis and 86.67% (13/15) for those with wet ears without otomycosis. Although the rates were different, the difference was not statistically significant (P = .62). Figure 1 shows a representative tympanic membrane preoperatively and at 3 months postoperatively. Notably, postoperative fungal infection led to graft failure in 2 of 25 patients with otomycosis, whereas postoperative multidrug-resistant infection with S. aureus or P. aeruginosa led to graft failure in 2 of 15 patients with wet ears but without otomycosis.
Comparison of Graft Success Between the Dry-Ear and Wet-Ear Group.
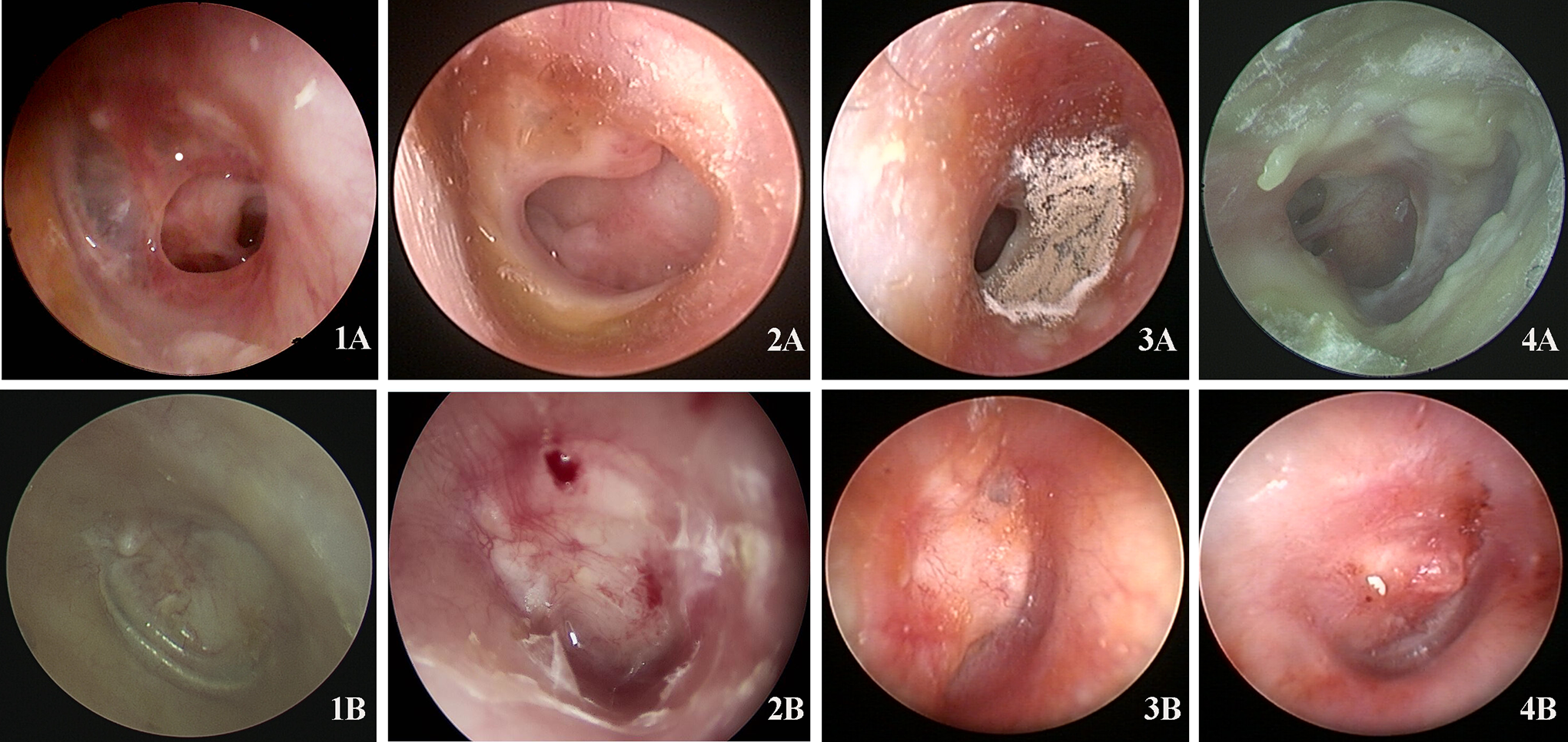
Preoperative and postoperative endoscopic images of the tympanic membrane. Panels 1A and 1B: Preoperative and postoperative images of the tympanic membrane in a dry ear. Panels 2A and 2B: Preoperative and postoperative images of the tympanic membrane in a wet ear without otomycosis. Panels 3A, 3B, 4A, and 4B: Preoperative and postoperative images of the tympanic membrane in a wet ear with otomycosis.
In the dry-ear group, the preoperative mean ABG was 17.34 ± 8.71 dB and the postoperative mean ABG was 10.97 ± 7.91 dB, with an ABG closure of 6.38 ± 4.71 dB. In the wet-ear group, the preoperative ABG was 19.09 ± 5.85 dB and the postoperative ABG was 11.38 ± 4.68 dB, with an ABG closure of 8.12 ± 6.11 dB (Table 4). Postoperative ABGs were significantly reduced in both the dry-ear and wet-ear groups, compared with preoperative ABGs. However, there was no significant difference in hearing gain between the 2 groups (P = .39). Furthermore, the preoperative ABG was 18.75 ± 6.32 dB and the postoperative ABG was 10.79 ± 4.13 dB, with an ABG closure of 8.13 ± 6.31 dB in the wet ears with otomycosis. The preoperative ABG was 20.55 ± 4.99 dB and the postoperative ABG was 11.64 ± 6.71 dB, with an ABG closure of 8.10 ± 5.93 dB in the wet ears without otomycosis. No significant difference in hearing gain was found in patients with wet ears with or without otomycosis (P = .86).
Comparison of Hearing Improvement Between the Dry-Ear and Wet-Ear Group Preoperatively and Postoperatively.a
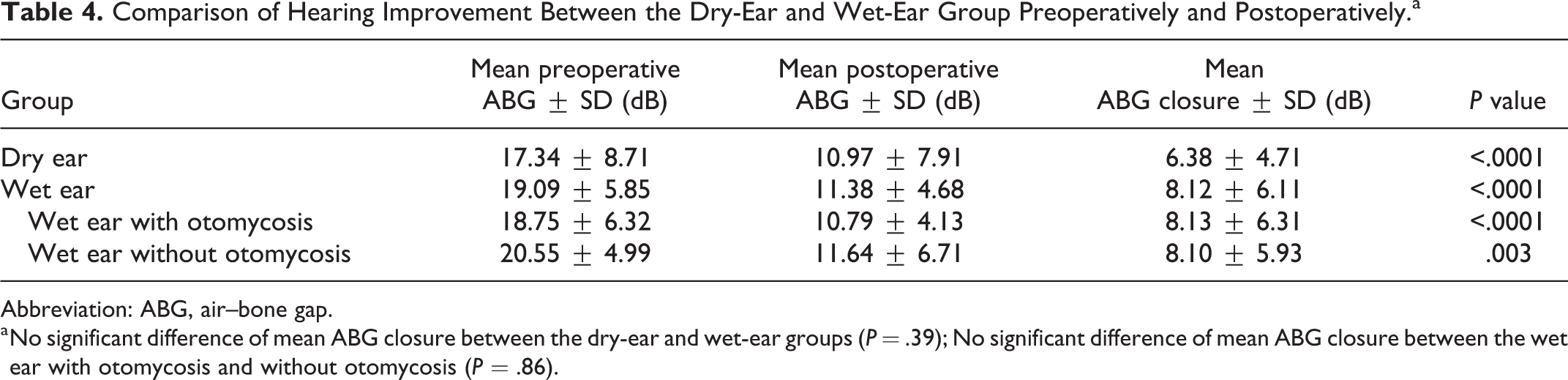
Abbreviation: ABG, air–bone gap.
a No significant difference of mean ABG closure between the dry-ear and wet-ear groups (P = .39); No significant difference of mean ABG closure between the wet ear with otomycosis and without otomycosis (P = .86).
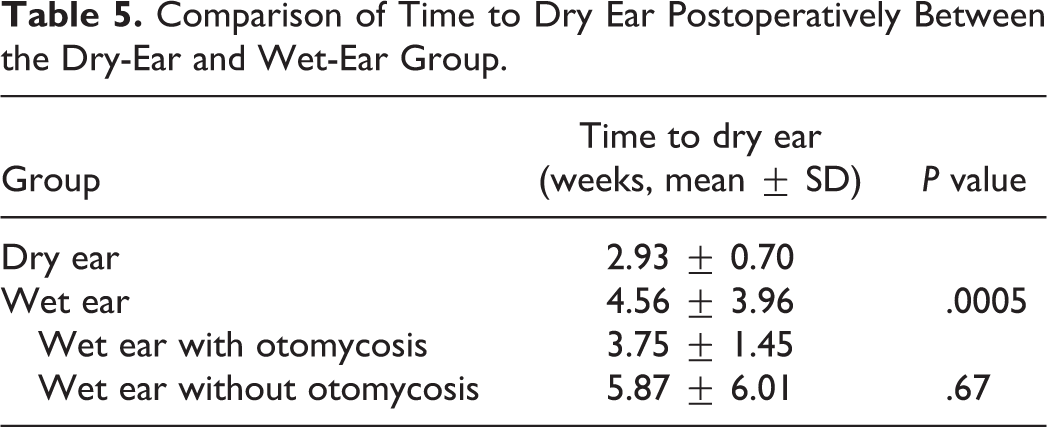
The time to achieve a dry ear was 2.93 ± 0.70 weeks postoperatively in the dry-ear group and 4.56 ± 3.96 weeks postoperatively in the wet-ear group. It took significantly longer to achieve a dry ear in the wet-ear group than in the dry-ear group (P = .0005; Table 5). However, no significant difference in the time to achieve a dry ear was observed in patients with wet ears with or without otomycosis (P = .67).
Comparison of Time to Dry Ear Postoperatively Between the Dry-Ear and Wet-Ear Group.
Discussion
Myringoplasty is a surgical procedure performed solely to repair a perforated tympanic membrane, without manipulation of the middle ear or ossicles. Recently, transcanal endoscopic myringoplasty has become popular due to the availability of high-resolution endoscopy technology. 11 Endoscopic myringoplasty results in treatment outcomes comparable to those of microscopic myringoplasty with respect to tympanic membrane, closure rates, as well as hearing improvement. 12 The endoscopic approach provides a much larger field of view and enables better cosmetic outcomes. Cartilage graft is the grafting material of choice for endoscopic myringoplasty. It is easy to harvest and suitable for one-handed operation under the endoscope due to its hardness. It has reported in many previous studies.13,14 In our study, all patients underwent transcanal endoscopic myringoplasty and achieved repair of a perforated tympanic membrane using tragal cartilage with a single-sided perichondrium. The results showed that the total graft success rate was 92.80%. Significant improvements in hearing were observed within the groups, based on preoperative versus postoperative measurements, similar to the results of other studies.15,16
The timing of myringoplasty surgery has been controversial. Gersdorff et al 17 found that the state of the middle ear at the time of surgery influenced the clinical outcomes—wet ears were associated with higher rates of perforation, myringitis, and retraction pockets. Another study by Zwierz et al 18 indicated that a better surgical outcome could be achieved in children with a dry ear, thus facilitating better middle ear conditions. In a multivariate analysis of otological, surgical, and patient-related factors involved in myringoplasty success, Onal et al 19 showed that a longer dry-ear period was a significant prognostic factor, positively influencing the rate of myringoplasty success. Moreover, the success rate was higher in dry ears than in wet ears. By contrast, Caylan et al 20 indicated that better healing was observed in discharging ears (100%) compared to dry ears (75%). In a prospective study, Hosny et al 21 reported that mucoid ear discharge has no adverse effect on the outcome of the operation as regard to graft uptake and hearing gain. Other studies1-5,22-25 have reported similar graft success rates between dry and wet ears. Notably, graft success and hearing improvement rates did not differ significantly between the dry-ear and wet-ear groups in our study.
Preoperative pathogen investigations provided important information concerning the reason for ear discharge (ie, bacterial infection, fungal infection, or both). Although some studies showed that otomycosis can lead to tympanic membrane perforation,26,27 the history of otomycosis was shorter than that of CSOM in most patients in our study. Recurrent middle ear discharge and the use or abuse of topical antibiotics and steroids in patients with CSOM are more likely to cause fungal infection in the external auditory canal. Furthermore, the graft success rate did not differ significantly between patients with wet ears and otomycosis and those with wet ears without otomycosis in our study. To the best of our knowledge, there has been limited research concerning graft success rates in patients with CSOM according to otomycosis status. One study reported that fungal otitis externa and a mucopurulent wet ear were factors influencing tympanic membrane closure. 9 However, that study only included a small number of patients. Among the 25 patients with otomycosis in our study, 2 experienced graft failure due to postoperative fungal infection. Graft failure occurred in 2 other patients in the wet-ear group because of multidrug-resistant S. aureus or P. aeruginosa (1 patient each). Among the remaining 36 patients with CSOM and wet ears, no postoperative infections were observed. No patient in the dry-ear group experienced postoperative infection. An important reason for these low rates of postoperative infection may be the use of povidone-iodine. In our study, povidone-iodine was used to irrigate the external auditory canal and middle ear at least 3 times during surgery. Some studies28-30 have shown that topical povidone-iodine can effectively kill bacteria and fungi in patients with otomycosis or CSOM. The discharge from all patients in the wet-ear group at 1 day preoperatively was cultured to identify causative pathogens. Multidrug-resistant S. aureus and P. aeruginosa were found in 2 patients and 1 patient, respectively. Graft failure occurred in 2 of the 3 patients. Therefore, patients with preoperative multidrug-resistant bacterial infection require preoperative and postoperative medication, as well as timely follow-up.
A notable finding was that the time to achieve dry ear was significantly longer in the wet-ear group than in the dry-ear group but did not influence the closure failure rate. Although postoperative otorrhea persisted in patients in the wet-ear group, this otorrhea was aseptic in most patients. No specific drugs were used on these patients. Only 4 patients exhibited persistent infection postoperatively. Possible causes of postoperative otorrhea are noninfectious, such as secretory middle ear mucosa, external auditory canal skin exudates, eczema, or eustachian tube dysfunction. 10 These results were similar to findings in a previous study. 31
Occasionally, ear discharge in patients with CSOM is difficult to control with drug treatment alone and often recurs preoperatively. The otology center in our hospital is one of the largest otology centers in China and receives a variety of patients from all areas of the country. Some patients at the time of registration may exhibit dry ears. However, at the time of surgery, those patients may have ear discharge. Therefore, it is difficult to ensure a dry ear status at the time of surgery. In this study, the results showed that otomycosis and mucopurulent discharge did not influence graft success or hearing improvement. However, this does not suggest that myringoplasty can be performed at any time. Preoperative discharge culture and antibiotic sensitivity tests should be performed routinely. When an infection is caused by multidrug-resistant bacteria, myringoplasty should be performed with caution.
Conclusion
Patients with CSOM and wet ears required more time to achieve a completely healthy status following endoscopic myringoplasty. However, graft success and hearing improvement rates were not affected by a wet middle ear or otomycosis. Thus, endoscopic myringoplasty using tragus cartilage is an effective treatment for refractory CSOM in patients with wet ears and otomycosis.
Footnotes
Authors’ Note
Juanmei Yang, MD, and Jihan Lyu, MD, contributed equally to this work. The patients gave their informed consent, and the study protocol was approved by the institutional review board of Hospital, and informed consent was provided by patients enrolled in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded in part by the National Natural Science Foundation of China (NSFC; Grant Nos. 81771017 and 81970880 to D.R.).