
Abstract
Introduction:
Central compartment atopic disease (CCAD) has recently been suggested as a phenotype of chronic rhinosinusitis (CRS). This study aims to investigate the prevalence of the radiologic CCAD phenotype in CRS within a pediatric population and identify its ability to predict comorbid allergy and asthma.
Methods:
Computed tomography and endoscopic examination were conducted on pediatric patients with CRS either with or without nasal polyps. Allergen sensitization was determined with the multiple-allergen simultaneous test and skin prick test. Serum total immunoglobulin E (IgE), peripheral blood eosinophil percentage, and presence of asthma were also evaluated.
Results:
A total of 82 pediatric patients were enrolled. Overall, 55 (67.1%) of the participants demonstrated aeroallergen sensitization, and 31 (18.9%) of the 164 sides of sinuses were radiologically defined to fit the CCAD phenotype. Patients having CRS with the CCAD phenotype had a higher prevalence of aeroallergen sensitization (87.1% vs 62.4%, P = .008), particularly house dust mite (74.2% vs 53.4%, P = .035), and a higher incidence of asthma (16.1% vs 3.8%, P = .010). Additionally, patients having CRS with the CCAD phenotype demonstrated a high serum total IgE levels (51.6% vs 30.1%, P = .023) in comparison to patients having CRS without CCAD.
Conclusion:
In pediatric CRS, the radiological CCAD phenotype was associated with allergen sensitization and asthma. Furthermore, the CCAD phenotype was associated with high serum total IgE levels, suggesting allergy etiology should be considered with this type of pediatric patients with CRS.
Keywords
Introduction
Chronic rhinosinusitis (CRS) is defined as an inflammatory condition within the paranasal sinuses that persists for more than 12 weeks and is underdiagnosed in childhood and adolescence. Chronic rhinosinusitis is characterized by a multifactorial inflammatory process influenced by a combination of genetic, environmental, bacterial, and immunologic factors as well as other etiologies. 1 Traditionally, primary CRS was classified into 2 major subtypes based on the presence of nasal polyposis: CRS with nasal polyposis (CRSwNP) and CRS without nasal polyposis (CRSsNP). However, recent studies have highlighted accumulating evidence for further differentiation of CRS phenotypes, 2 which may help predict CRS risk factors, disease progression, and treatment response. Furthermore, the role of allergy as a comorbidity for CRS remains unclear and may have a greater association with certain CRS phenotypes.
Central compartment atopic disease (CCAD) is a relatively newly defined CRS variant strongly associated with allergy. First described in 2014, White et al defined an association between isolated middle turbinate (MT) polypoid changes and inhalant allergen sensitization. 3 In 2017, DelGaudio et al coined the term CCAD describing it as a more advanced stage of the previously described isolated MT atopic polypoid changes, with additional involvement of the superior turbinate (ST) and posterosuperior nasal septum (PSNS). 4 Radiologic findings associated with CCAD evaluated by Hamizan et al supported an association between radiological patterns defined by centrally limited changes and allergy status. 5 A few additional studies and reviews have reported the strong association between this central pattern of inflammatory changes and allergy; however, the occurrence and impact of CCAD have yet to receive necessary attention in pediatric patients.1,6-8
Since early diagnosis is required for optimal care and outcomes in allergic disease, any associated factors should be recognized as early as possible, especially in pediatric patients given their long time frame of treatment. Here we attempted to ascertain the predictive ability of radiologic CCAD at identifying allergy and asthma in pediatric patients.
Methods
Study Design
This single-center retrospective study included pediatric patients (≤ 20 years old) with suspected CRS who underwent both allergic and radiological assessments in Korea University Anam Hospital between January 2019 and February 2020. Diagnosis of CRS was made in accordance with the 2012 European position paper on rhinosinusitis and nasal polyps. 9 Patients having CRS both with and without nasal polyps identified by nasal endoscopy were included. Patients diagnosed with other sinus conditions, such as barosinusitis, mucocele, recurrent acute rhinosinusitis, antrochoanal polyps, and sinusitis from dental origin, or those who had prior sinus surgery were excluded. Patients with systemic conditions (immunodeficiency, vasculitis, cystic fibrosis, or granulomatous disease) that may potentially affect mucosal tissue were also excluded. In addition, patients with any ongoing medical treatment for CRS or allergic rhinitis (intranasal corticosteroid, antihistamine) or for any other condition within past 4 weeks were excluded.
Adenoid hypertrophy was defined as choanal obstruction identified by nasal endoscopic examination or using the Saedi criteria on the sagittal section of computed tomography (CT) in cases when the patients were uncooperative in nasopharynx examination. 10 Asthma was estimated based on the presence of symptoms such as wheezing, cough, or rapid breathing along with a previous physician’s diagnosis. The study’s protocol was approved by the institutional review board of Korea University Anam Hospital (2020AN0511), and the requirement for informed consent was waived.
Evaluation of Allergen Sensitization and Peripheral Blood Eosinophil
Allergy assessments were performed with either a multiple-allergen simultaneous test (MAST) or skin prick test for inhalant allergens. Aeroallergen profiles were grouped into the following: house dust mite, animals, pollen, and others (Supplemental Table S1). Participants with a positive result for any specific allergen were classified into the allergen-sensitized group.
Serum total immunoglobulin E (IgE) levels and blood eosinophil percentages were measured from laboratory assessments. High serum total IgE levels were defined as values of 100 IU/mL or greater. The cutoff value of high peripheral blood eosinophil was defined as 5%, according to Japanese Epidemiological Survey of Refractory Eosinophilic Chronic Rhinosinusitis (JESREC) score, which predicts eosinophil dominance in CRS. 11 All of laboratory and allergy assessments were conducted within 3 months of radiologic and endoscopic assessment.
Radiologic Assessment
All patients underwent a CT scanning, with the images evaluated by an experienced pediatric radiologist, who was blinded to the patient’s allergy status. The radiologist evaluated soft tissue thickening in the central compartment of the nasal cavity (MT, ST, and PSNS) and the presence and pattern of sinus involvement for each side. Before interpretation, the criteria to describe the patterns that could be associated with CCAD were established (Figure 1). Nasal cavity involvement with CCAD was defined as swelling of the MT and ST accompanied by significant narrowing of the superior and middle nasal meatus. Sinus involvement with CCAD was defined as soft tissue thickening in the medial walls of the sinus cavity along with sparing of the roof and lateral walls of the sinus cavity. The classification of radiologic finding into either CCAD phenotype or non-CCAD phenotype was done per side following the method of Hamizan et al. 5 The cases of inflammation in which one side is a CCAD radiologic phenotype and the other side is involved to lateral side of sinuses were considered as unilateral CCAD.
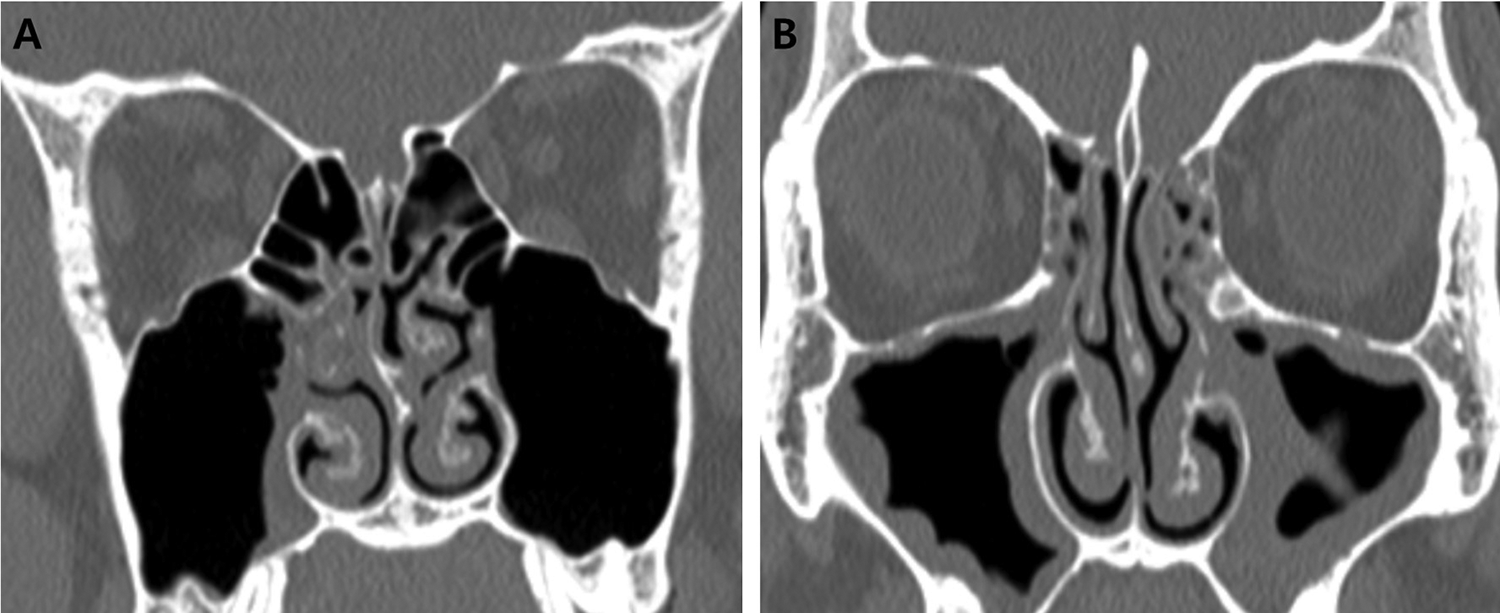
Computed tomography images demonstrating (A) chronic rhinosinusitis (CRS) with central compartment atopic disease (CCAD) and (B) CRS without CCAD. A, This coronal image shows bilateral swelling of middle turbinate with narrowing of middle meatus. Right maxillary sinus exhibits soft tissue thickening involving the medial wall, with sparing of the roof and lateral walls. B, This coronal image shows diffuse involvement of the bilateral maxillary sinus walls with preserved middle and superior meatus.
Statistical Analysis
Statistical analyses were conducted using SPSS version 20.0 (IBM Corp). Values for continuous variables were represented as mean with standard deviation, and those for categorical variables were expressed using number and percentage. Student t test was used to analyze the differences between 2 groups for continuous variables, and chi-square analysis was conducted for categorical variables. Binary logistic regression analysis was used to predict allergic sensitization and asthma by evaluating the contribution of parameter associated with chronic sinusitis.
Results
Demographics
A total of 82 pediatric patients diagnosed with CRS were enrolled in the study, and 55 (67.1%) patients were classified as allergen-sensitized group (Table 1). The mean age was 16.10 ± 3.53 and 61 (74.4%) were male. Of the total cases, 55 (67.1%) were considered sensitized to at least 1 aeroallergen. The mean age was 16.56 ± 2.83 in the allergy group and 15.15 ± 4.54 (P = .015) in the nonallergy group. Further, the proportion of male participants was significantly higher in the allergy group (80.0%) than in the nonallergy group (63.0%; P = .019). The prevalence of radiological defined CCAD was significantly higher in the allergy group (24.5%) than in the nonallergy group (7.4%; P = .008). The prevalence of asthma was higher in the allergy group (9.1%) than in the nonallergy group (0.0%; P = .022). Furthermore, the proportion of participants with peripheral blood eosinophil over 5% was greater in the allergy group (27.3%) compared to the nonallergy group (11.1%; P = .020). There was no statistical difference in the presence of nasal polyps and adenoid hypertrophy between the 2 groups.
Demographic Characteristics of Allergen-Sensitized and Nonallergen-Sensitized Pediatric Patients With CRS.
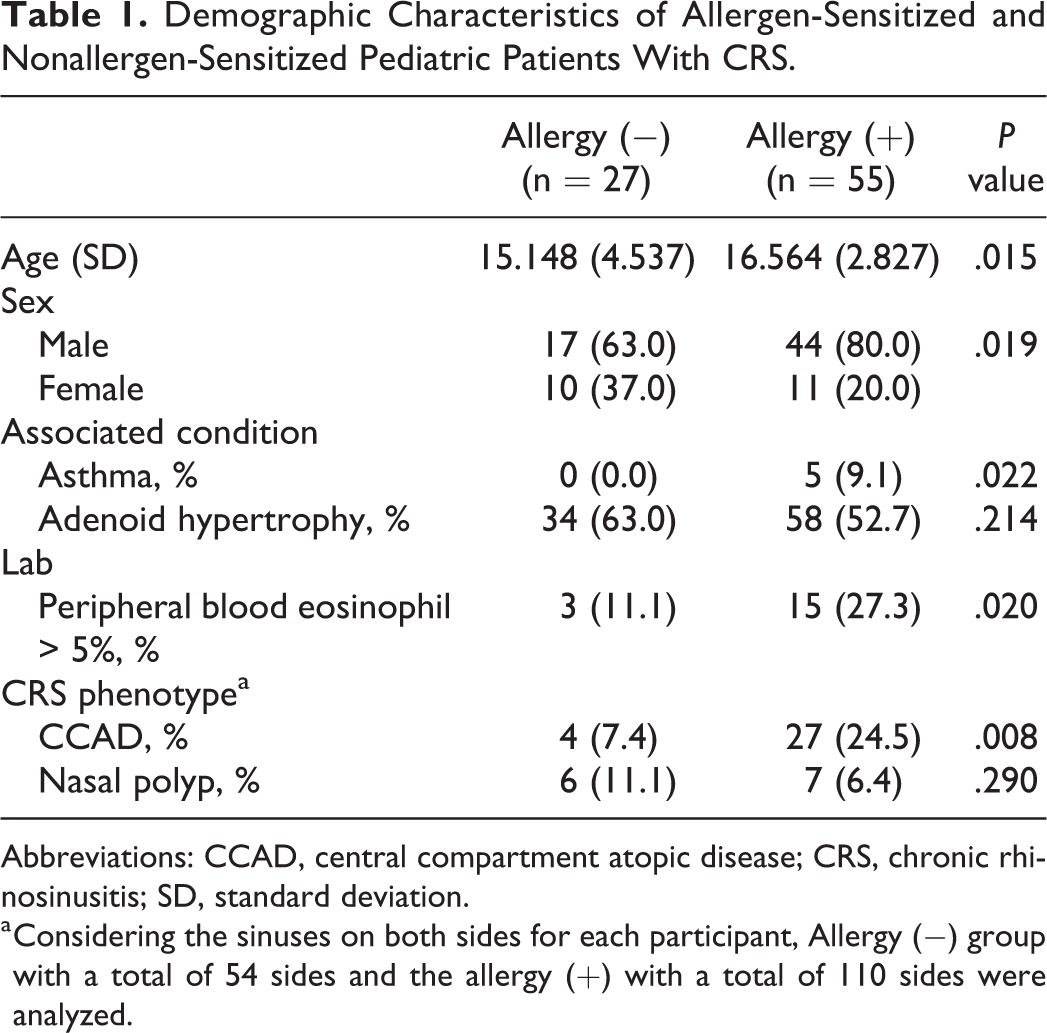
Abbreviations: CCAD, central compartment atopic disease; CRS, chronic rhinosinusitis; SD, standard deviation.
a Considering the sinuses on both sides for each participant, Allergy (−) group with a total of 54 sides and the allergy (+) with a total of 110 sides were analyzed.
Prevalence of CRS-Associated Factors in Patients With and Without the Radiologic CCAD Phenotype
Among the 164 sides of sinuses from 82 participants evaluated, 31 (18.9%) were determined to exhibit the CCAD phenotype. The characteristics, including allergen sensitivity, for patients with and without the radiologically determined CCAD radiologic phenotype are shown in Table 2. There was no statistical difference in age or sex distribution between patients with and without the CCAD phenotype. Additionally, the CCAD group had a greater proportion of individuals with high serum total IgE levels (51.6% vs 30.1%; P = .023). They also had a greater proportion test positive in response to any of the aeroallergens (87.1% vs 62.4%; P = .008). Furthermore, patients having CRS with the CCAD phenotype demonstrated higher HDM sensitization (74.2%) than did non-CCAD patients (53.4%; P = .035), there was no statistical difference in sensitization to pollen (P = .227) or animals (P = .071) between the 2 groups.
Characteristics of Patients Having Chronic Rhinosinusitis With and Without the Radiologically determined Central Compartment Atopic Disease Phenotype.
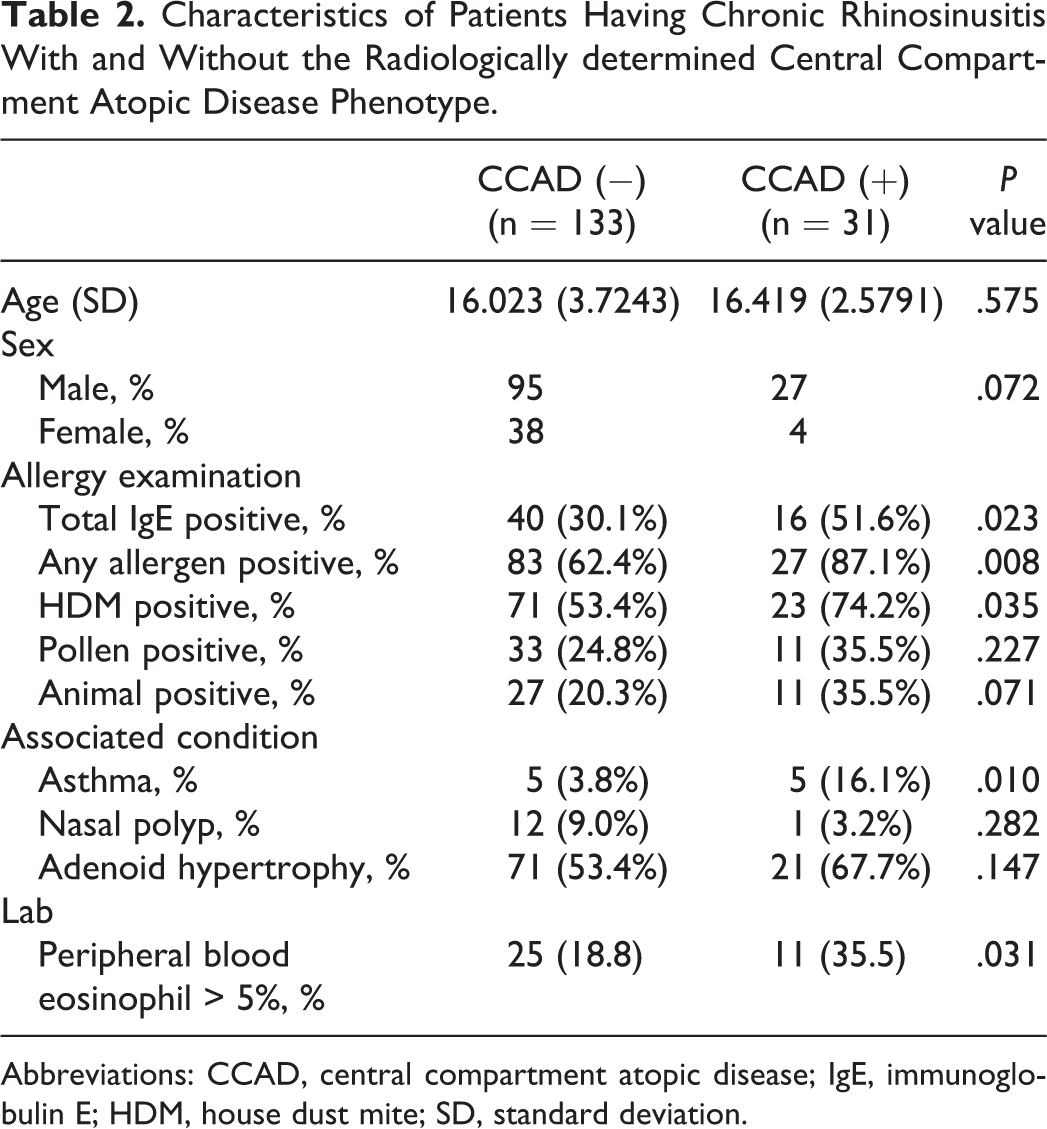
Abbreviations: CCAD, central compartment atopic disease; IgE, immunoglobulin E; HDM, house dust mite; SD, standard deviation.
Asthma prevalence (16.1% vs 3.8%; P = .010) and high peripheral blood eosinophil percentage (35.5% vs 18.8%; P = .031) were both greater in patients having CRS with CCAD. The presence of nasal polyps (P = .282) and adenoid hypertrophy (P = .147) was not statistical different between the 2 groups.
Allergy-Related Serum Markers in Each CRS Phenotype
Since the most important factor in determining the CRS phenotype is nasal polyps, we classified CRSwNP (n = 12) by endoscopic examination, and further classified CRSsNP as CCAD CRSsNP (n = 30) or nonCCAD CRSsNP (n = 122) based on their radiologic findings. The endoscopic findings of the patients with CCAD CRSsNP tended to show polypoid changes or mucosa swelling of MT or nasal septum (Figure 2A), which was distinguished them both from the endoscopic findings of non-CCAD CRSsNP (Figure 2B) and CRSwNP (Figure 2C).
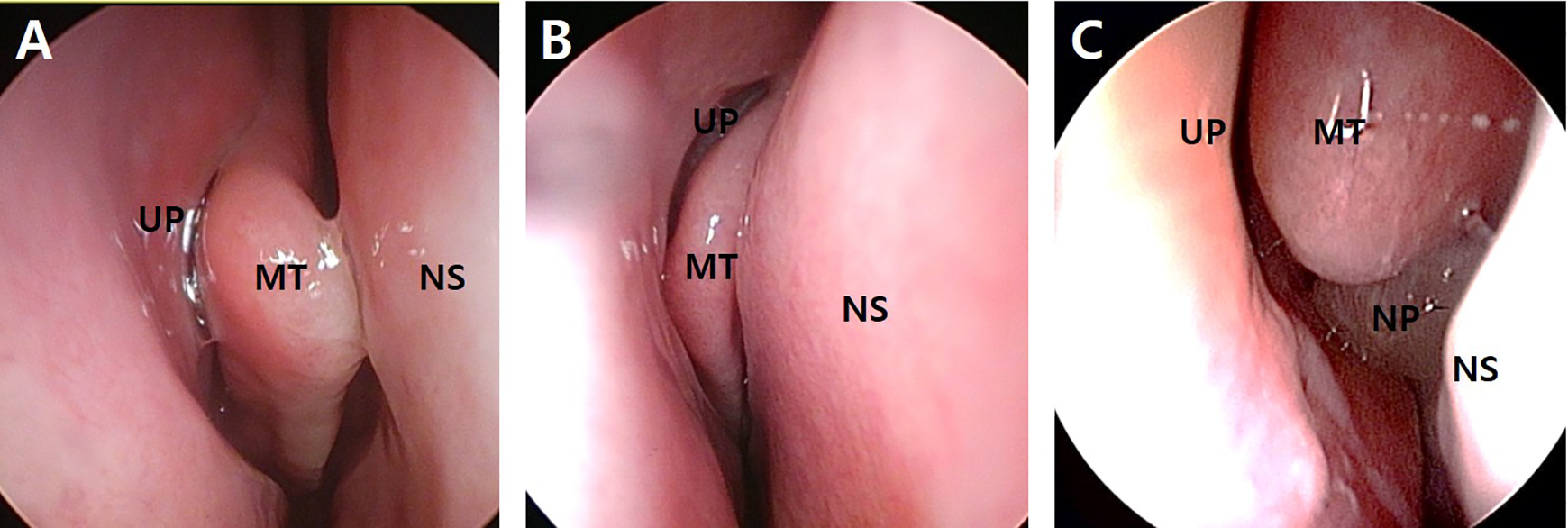
Endoscopic images of chronic rhinosinusitis (CRS) phenotypes. A, Central compartment atopic disease (CCAD) exhibiting polypoid changes of middle turbinate (MT) of right nasal cavity; B, CRS without nasal polyp (NP) without radiological findings of CCAD of right nasal cavity; C, CRS with NP of right nasal cavity. UP indicates uncinate process; NS, nasal septum.
We further analyzed differences in laboratory results related to allergic inflammation among each of the CRS phenotypes. The CCAD CRSsNP group (86.7%) demonstrated the highest prevalence of sensitization to any aeroallergen compared to the non-CCAD CRSsNP group (63.9%; P = .016) and the CRSwNP group (50.0%; P = .020; Figure 3A). The CCAD CRSsNP group also had the greater proportion of participants with high serum total IgE (53.3%) compared to the non-CCAD CRSsNP group (30.3%) and CRSwNP group (25.0%); however, this difference was only statistically significant when compared with the non-CCAD CRSsNP group (P = .031; Figure 3B). Further, the proportion of participants with the peripheral blood eosinophil percentage over 5% was significantly higher in CCAD CRSsNP group (42.8%) compared to both the non-CCAD CRSsNP group (21.0%; P = .045) and the CRSwNP group (0.0%; P < .001; Figure 3C).
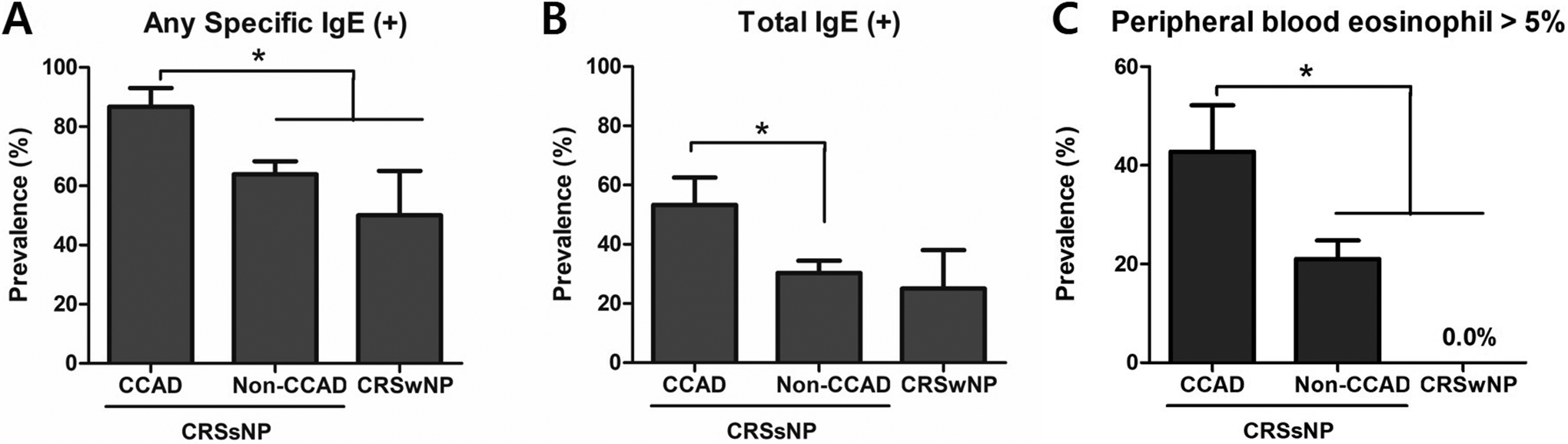
Differences between serum markers of Th2 inflammation among each CRS clinical phenotype. A, Prevalence of any aeroallergen sensitization; B, prevalence of high (≥100 IU/mL) serum total immunoglobulin E (IgE) levels; C, serum eosinophil percentage.
Contribution of Individual Parameters to Predict Allergy and Asthma
A binary regression model was conducted to analyze the predictability of variables related to CRS including CCAD for allergen sensitization and asthma (Table 3). Of all the variables tested, radiological findings of CCAD showed the greatest association both with allergen sensitization (odds ratio [OR] = 4.066, P = .013) and asthma (OR = 4.923, P = .017). Peripheral blood eosinophil greater than 5% was also demonstrated an association with both allergen sensitization (OR = 2.836, P = .032) and asthma (OR = 5.948, P = .009). Adenoid hypertrophy was found to have no significant ability to predict either allergen sensitization or asthma in patients with CRS.
Binary Logistic Regression Model Predicting Allergen Sensitization and Asthma Among Pediatric Patients With Chronic Rhinosinusitis.
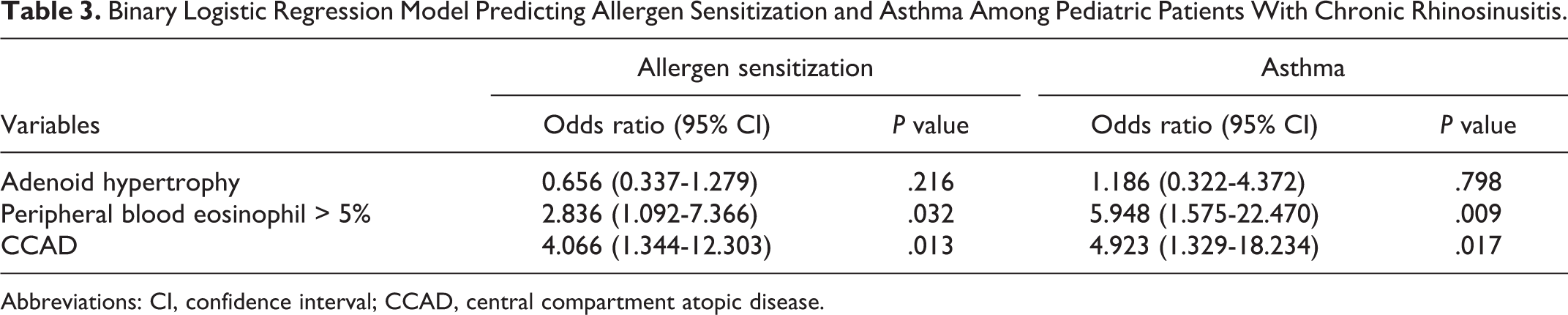
Abbreviations: CI, confidence interval; CCAD, central compartment atopic disease.
Discussion
Central compartment atopic disease is a disease process wherein the primary pathology is allergic edema of the turbinate mucosa, resulting in nasal airway obstruction and sinonasal findings in advanced disease. This may secondarily obstruct the sinus ostia with minimal lateral sinus changes, giving rise to CRS. 12 Although allergic airway inflammation commonly occurs in childhood or adolescence, and allergic rhinitis is an important contributing factor in pediatric CRS, research studies of CCAD in CRS have primarily been conducted in adults. 7 To the best of our knowledge, this study is the first report evaluating the correlation between CCAD and both allergy and asthma in pediatric patients.
The prevalence of the radiologic CCAD phenotype in pediatric patients with CRS (18.2%) was found to be slightly higher than had been previously reported in adults (15.2%) by Hamizan et al. The results of our study indicate that the radiologic CCAD phenotype is associated with atopic condition, especially with house dust mite allergen sensitivity. 5 These findings are consistent with a previous study evaluating radiologic features of CCAD in adults. They reported a higher prevalence of dust aeroallergen sensitization in the radiologic CCAD phenotype patients with CRS compared to their controls, but not for animal, mold, or grass. 5 Our subtype analysis classifying CRSwNP separately suggested that radiologic CCAD was more strongly associated with allergen sensitization than the presence of nasal polyps. Previous studies of nasal endoscopic findings and allergic sensitization in CRS also reported that nasal polyps were not related to aeroallergen sensitization. 13 However, polypoid changes of MT were found to be a useful indicator for atopic condition, this may be due to the deposition of inhaled allergens on the head of the MT, resulting in mucosal inflammation.3,14 We were able to confirm the presence of known characteristics for the CCAD phenotype of CRS in adults within our pediatric population, specifically edema of the MT and nasal septum. Thus, both endoscopic and radiologic features suggesting CCAD might be used as indicators for predicting atopic condition in children.
Since CCAD is known to be an IgE-mediated condition, we investigated the association of the CCAD phenotype with both serum total IgE levels and peripheral blood eosinophil percentage, both of which are known markers for Th2 inflammation including allergic rhinitis, asthma, and atopic dermatitis.15,16 Pediatric patients having CRS with the CCAD phenotype showed a higher prevalence of high serum total IgE levels. In addition, the peripheral blood eosinophil percentage was also higher in the CCAD phenotype in comparison to the other CRS phenotypes including CRSwNP. In CRS, peripheral blood eosinophil elevation correlates with tissue eosinophilia, which is known to be prominent in eosinophilic type CRSwNP.17,18 However, since onset of eosinophilic CRS typically occurs after 30 years of age, this may explain why peripheral blood eosinophilia was not identified in our CRSwNP pediatric group, and higher eosinophil percentage was identified in CCAD, which is characterized by Th2 dominant inflammation. 7
In the present study, pediatric patients having CRS with the CCAD phenotype were found to have a greater prevalence of asthma, an IgE-mediated lower airway disease closely related to CRS and allergic rhinitis. A previous study in adults reported that prevalence of asthma was not associated with radiologic CCAD phenotype of CRS. 5 However, further results from the European survey conducted by the GA2LEN suggested a strong association between CRS and asthma is prominent in populations with allergic rhinitis. 2 Additionally, a study of 4044 children found the presence of allergic rhinitis to be an independent factor associated with asthma in patients with CRS, with OR of 8.25, further supporting the results from our study. 19
Adenoid tissue is a known contributor to the pathophysiology of CRS in children. 20 Thus, we analyzed the correlation between CCAD and adenoid hypertrophy in CRS, which has not previously been conducted in studies with adults. Past studies evaluating the association between allergic rhinitis and adenoid hypertrophy have claimed conflicting results. Studies by Eren et al 21 and Ameli et al 12 reported that the presence of adenoid hypertrophy was negatively correlated with allergic rhinitis. However, Huang and Giannoni 23 and Dogru et al 22 suggested a positive association between allergic rhinitis and adenoid hypertrophy in children sensitized to certain allergens such as mold or pollen. Our results showed adenoid hypertrophy in pediatric CRS was not associated with either the CCAD phenotype or positive tests for aeroallergen sensitization. Our results support previous findings that suggest that in pediatric CRS, obstruction of posterior nasal passages and adenoid tissue itself serving as a bacterial reservoir may be the main mechanism of adenoid hypertrophy in sinus pathology.24,25 Nevertheless, since adenoid hypertrophy is known to be less common after age 15, the high proportion of older pediatric population in our study could have an effect on the results.
The present study has several limitations. First, the majority of the study participants were aged 15 years or older, thus could not reflect younger pediatric population. Since our study design was cross-sectional, it might not have adequately reflected possible fluctuations in allergen sensitization or CT findings due to seasonal changes or symptom severity, and previous transition from CCAD phenotype to diffuse sinus inflammation. Additionally, the presence of asthma could be overdiagnosed as it was assessed by questionnaire, and pulmonary function tests were not conducted. Future prospective studies are needed to evaluate the impact of CCAD on the disease prognosis and to investigate the clinical relevance of CCAD in younger pediatric population. However, this study is significant as the first to evaluate the CCAD phenotype in pediatric CRS and elucidate its association with various factors using endoscopic examination and serum markers.
Conclusions
The CCAD phenotype was associated with allergen sensitization, particularly house dust mite, in pediatric CRS. Additionally, serum total IgE levels and eosinophil percentage were both higher in patients with CCAD than other CRS phenotypes including nasal polyps. The findings may result in improvements in classification strategies resulting accurate diagnoses and patient-tailored therapy for patients with pediatric CRS, such as allergen-directed immunotherapy or anti-IgE therapy in the CCAD phenotype of CRS.
Supplemental Material
Supplemental Material, sj-pdf-1-ear-10.1177_0145561321997546 - Predictive Value of Radiologic Central Compartment Atopic Disease for Identifying Allergy and Asthma in Pediatric Patients
Supplemental Material, sj-pdf-1-ear-10.1177_0145561321997546 for Predictive Value of Radiologic Central Compartment Atopic Disease for Identifying Allergy and Asthma in Pediatric Patients by Kijeong Lee, Tae Hoon Kim, Sang Hag Lee, Chang Ho Kang, Bo-Kyung Je and Saelin Oh in Ear, Nose & Throat Journal
Footnotes
Authors’ Note
Lee and Oh contributed to conceptualization, methodology, writing—review and editing, project administration, and funding acquisition. Lee and Kang contributed to software. Kim and Je contributed to validation. Lee contributed to formal analysis, data curation, and writing—original draft preparation. Oh contributed to investigation and project administration. Kim and Lee contributed to resources. Je and Kang contributed to visualization. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant of Korea University Anam Hospital, Seoul, Republic of Korea (Grant No. O2000711, O2000721).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.