
Abstract
Epstein-Barr virus (EBV) associated lymphoproliferative disorders includes a diverse group of diagnoses, encompassing both B-cell and T-cell lineages. With EBV mucocutaneous ulcers becoming a World health Organization diagnosis in 2018, introduction of the disease entity will be beneficial to the practicing otolaryngologist. We are reporting a case of a 69-year-old male with history of rheumatoid arthritis on methotrexate, recently undergoing dental extractions, who then developed multiple oral ulcerations and bony erosions of his palate and alveolar ridge. Associated symptoms included a large 3.0 cm neck mass, splenomegaly, and pulmonary nodules. Histopathology showed EBV+ lymphomatoid granulomatosis. Upon removal of immunosuppressive agent, patient’s symptoms improved with resolution of oral lesions, as well as systemic symptoms.
Keywords
Introduction
Epstein-Barr virus (EBV)-associated lymphoproliferative disorders includes a diverse group of diagnoses, encompassing both B-cell and T-cell lineages. 1 Since Docjcinov et al first described EBV mucocutaneous ulcers (EBVMCU) in 2010, sparse literature has been produced on the participant, including 90 cases discussed in 26 papers. 2 Understanding the pathophysiology of such disorders including their clinical picture is integral in early diagnosis and correct treatment.
We are reporting a case of a 69-year-old male with history of rheumatoid arthritis on methotrexate, recently undergoing dental extractions, who then developed multiple oral ulcerations with an associated 3.0 cm ipsilateral neck mass. On diagnostic studies there was computed tomography (CT) proven bony erosion of the alveolar ridge and inferior maxillary sinus, associated with pulmonary nodules and splenomegaly.
Histopathological examination showed angiocentric and angiodestructive lymphoid infiltrate associated with several admixed histiocytes, cells positive for CD20, CD30, as well as EBV+, which concluded with suspicion for EBV+ lymphomatoid granulomatosis. Upon ruling out large B-cell lymphoma due to EBV, patient had methotrexate removed from rheumatoid treatment, and within 4 weeks patients clinical symptoms and physical examination significantly improved to normal healthy mucosa, and subsequent bone biopsy showed removal of EBV+ tissue and lymphoid aggregate.
Case Report
A 69-year-old male was referred from his dentist for oral ulcers on the alveolar ridge and hard palate after dental extractions 4 months prior. On physical examination, the patient had a large infiltrative lesion on left alveolar ridge and palate (as seen in Figure 1), and a 3.0 cm level 3 neck mass. Computed tomography scan showed left anterior alveolar ridge destruction along the cortical margin anterior to the incisive foramen measuring 2.2 cm associated with left inferior maxillary sinus destruction with 3.0 cm lymphadenopathy (as seen in Figure 2). There was clinical suspicion for a malignant process and patient was scheduled for panendoscopy and biopsy of lesion.

Infiltrative lesion on the alveolar ridge and hard palate.
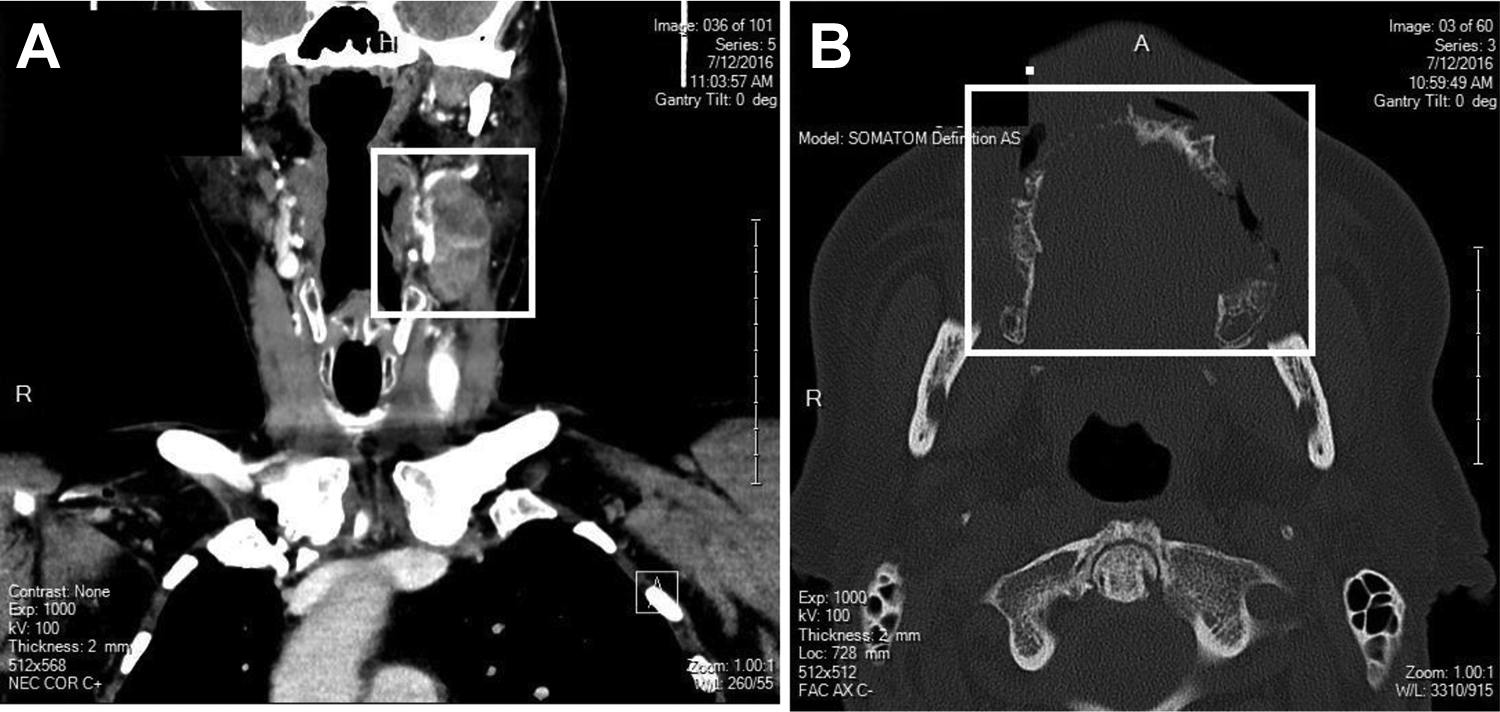
A, Coronal view of large left 3 cm lymphadenopathy; (B) axial bone window of hard palate and left alveolar ridge erosion.
Patient’s histology showed atypical angiocentric lymphoid infiltrate with admixed histiocytes and mucosal ulceration, suspicious for lymphatoid granulomatosis (as seen in Figure 3). Patient’s specimen was CD20+/30+, as well as EBV assay positive (Figure 4). Histology was sent off for expert opinion, who concurred with diagnosis, but was hesitant with diagnosis of EBV mucocutaneous ulcers. This in part was due to disseminated disease of pulmonary nodules and splenomegaly, and recommended trial off of methotrexate, with hopeful resolution of patient’s symptoms. There was also recommendation for further biopsy of bony lesions to definitively rule out EBV-associated non-Hodgkin lymphoma (NHL).
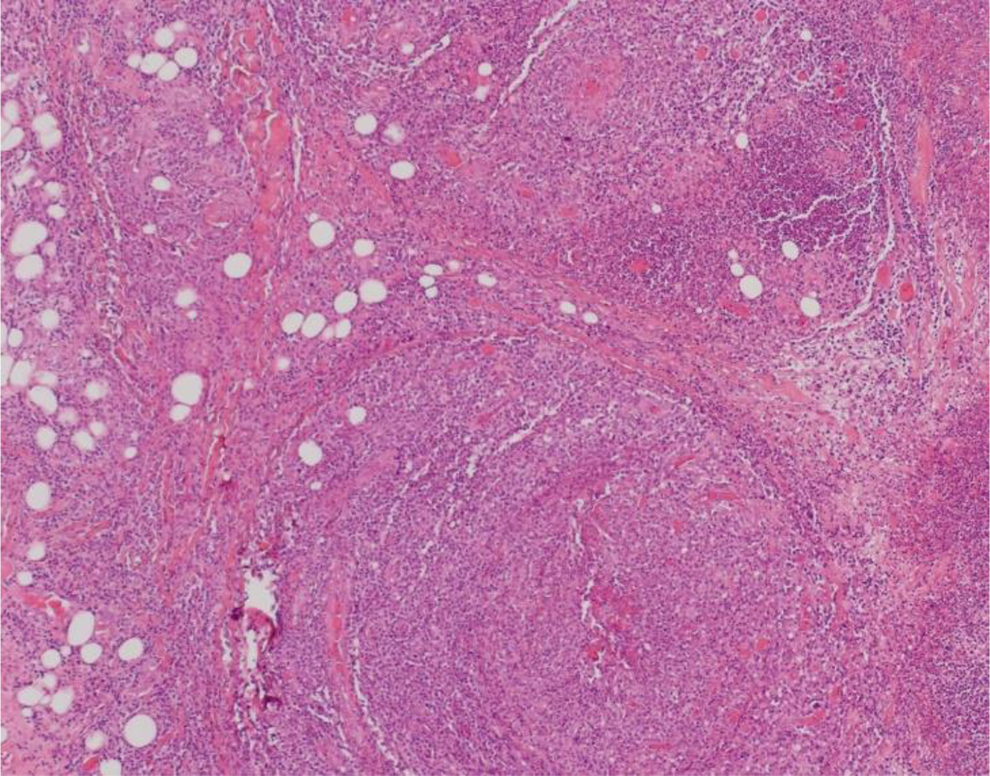
Nodular angiocentric infiltrate with vessel necrosis surrounded by large lymphocytes.
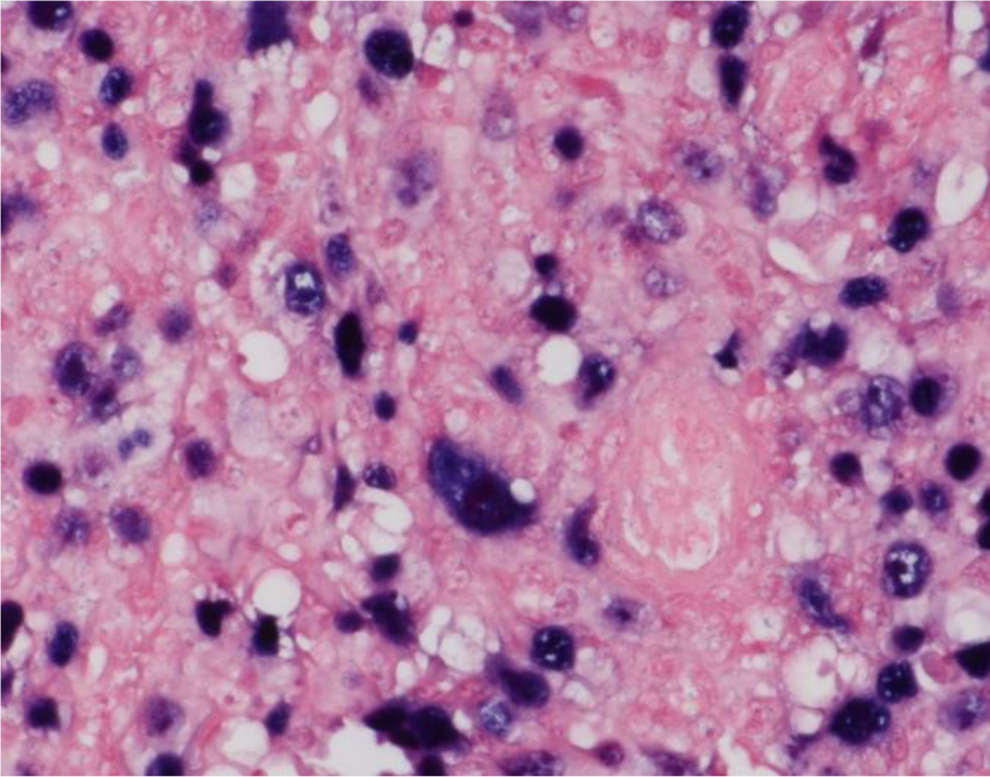
Epstein-Barr virus positive staining.
Patient was taken off methotrexate, and within 3 weeks there was significant improvement of clinical symptoms and resolution of ulcers. Positron emission tomography scan showed improved soft tissue changes with residual bony obstruction of inferior maxillary sinus, with reduced lymphadenopathy to 10 mm. In terms of the systemic process, there was a decrease in splenomegaly and pulmonary nodule size. A bone biopsy was performed which showed no evidence of NHL, and recommendation was CT scan of lesions at 6 months off methotrexate to evaluate residual disease.
The sixth-month CT showed less prominent bony destruction to maxillary sinus and alveolar ridge, as well as less prominent soft tissue changes, no further splenomegaly, and small pulmonary nodules still present. Patient had no sign of malignancy at this time and was diagnosed with EBV-associated lymphoproliferative disease secondary to methotrexate.
Discussion
Epstein-Barr virus lymphoproliferative disorders encompass a disease modality associated with immunosuppression, whether associated with immunosuppressive diseases such as HIV or iatrogenically caused by medications due to autoimmune disease. Over 95% of the population has detectable levels of EBV, positive forimmunoglobulin G, but most remain asymptomatic. The World Health Organization (WHO) divided EBV-associated disorders into B-cell and T-cell types. Epstein-Barr virus-associated B-cell type include acute infections such as infectious mononucleosis, chronic active EBV infections over periods longer than 6 months, lymphomas such as EBV-positive diffuse large B-cell lymphoma, local latent infections including EBV mucocutaneous ulcer, and systemic latent manifestation which includes lymphomatoid granulomatosis.2,3 It wasn’t until 2018 that the WHO declared EBVMCU its own diagnostic entity. 4
For the otolaryngologist, mucocutaneous ulcerations carry a wide range of diagnoses, from benign lesions to malignant neoplasms. The patient in this study arrived with an alarming lesion encompassing a large part of his oral cavity (Figure 1) with significant lymphadenopathy which directed our diagnosis toward malignancy. 3 Histopathology performed on the oral lesions showed atypical angiocentric lymphoid infiltrate with admixed histiocytes and mucosal ulceration, positive for EBV and CD20+/30+. With these findings, the differential diagnosis ranges from indolent EBV-associated mucocutaneous ulcer, lymphomatoid granulomatosis, to EBV associated large B-cell lymphoma.5,6 Since encounters with these pathologies are quite rare in otolaryngology, having a skilled team of pathologists, oncologists, and hematologists is necessary.3,7
Understanding the nature of these disease processes is integral for correct diagnosis. Immunosuppression hinders the autoregulation of suppressed EBV cells, allowing certain gene upregulation to activate the cell cycle, leading to overexpression of B-cells, resulting in local or systemic manifestations.1,8 The patient in this study began methotrexate for rheumatoid arthritis which led to upregulation of EBV-associated B-cells in his oral cavity leading to mucocutaneous disease. Although not confirmed by biopsy (spleen and lung lesions), this patient had other manifestations consistent with lymphomatoid granulomatosis including lung nodules and splenomegaly found on imaging.
Ruling out malignancy by differentiating between mucocutaneous ulcer, lymphomatoid granulomatosis, and large B-cell lymphoma involved further consultation. This included remote tissue biopsy to evaluate for possible gene alteration leading to a malignant neoplasm, as well as removing the offending agent from patient’s medication and tracking results. After just 3 weeks of methotrexate removal, patient’s clinical symptoms of pain and oral bleeding significantly improved, as well as ulceration and breakdown on physical examination. The remote tissue biopsy showed no signs of NHL, which placed our diagnosis on the benign scale between EBV-associated mucocutaneous ulcer and lymphomatoid granulomatosis.
In summary, our patient arrived with alarming clinical symptoms which included large oral ulcers and significant lymphadenopathy resembling a malignant process. Over the course of 6 months, working with a multidisciplined team, we were able to diagnose our patient, remove the offending agent, and restore normal life to the patient.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.