
Abstract
Neonatal HNT in the pharynx is a rare cause of respiratory distress and poor feeding in the newborn, but must be differentiated from teratoma, encephalocele, and nasal glioma. While surgical resection is the preferred treatment modality, we posit there is a role for sclerosis of the glial heterotopic cyst if complete surgical excision is not possible or carries risk of high morbidity. Here, we present a case of a 7-day-old neonate presenting with acute respiratory distress found to have a nasopharyngeal/oropharyngeal mass ultimately treated with sclerotherapy at 9 months of age.
Keywords
Introduction
Heterotopic neuroglial tissue is a rare benign, congenital disorder that presents most commonly in the nasal cavity, and also uncommonly in the scalp, parapharyngeal space, orbit, temporal bone, oral cavity, and palate.1-4 It is often associated with neonatal respiratory distress and difficulty feeding. 1 It can be associated with Pierre Robin Sequence, cleft palate, or choanal stenosis.4,5 There have been approximately 200 cases reported in the literature of heterotopic neuroglial tissue with fewer than 40 cases originating in the pharynx, nearly all of which were treated with surgical excision. 4 Here, we report a rare case of heterotopic neuroglial tissue in a 7-day-old female presenting with respiratory distress and feeding difficulties.
A 7-day-old term female was evaluated for acute respiratory distress and difficulty feeding in the neonatal intensive care unit following transfer from an outside hospital. On nasal endoscopy and laryngoscopy examination, the patient had a pedunculated, polypoid, obstructive nasopharyngeal/oropharyngeal mass. Magnetic resonance imaging (MRI) revealed a homogenous, T2-hyperintense mass in the nasopharynx and posterior oropharynx without dural connection (Figure 1A). The patient was taken to the operating room at 11 days of age and underwent transoral excision of the obstructing nasopharyngeal portion of the mass without complication. Histopathology revealed mature glial tissue with astrocytes, oligodendrocytes, neurons, and complex ependymal-like cystic structures (Figure 1B). Despite initial improvement, the patient’s family reported increasing episodic stertor, difficulty feeding, and snoring by 1 month postoperatively. Examination revealed residual submucosal fullness partially obstructing the left-sided nasopharyngeal and oropharyngeal airway (Figure 1C). Continued worsening of symptoms at 2-months postoperatively prompted a computed tomography (CT) scan to evaluate for skull base defect suggestive of meningeal tail prior to consideration of sclerotherapy instead of surgical excision. To rule out encephalocele the patient was taken to the operating room at age 6 months for aspiration of cystic fluid, which tested negative for β-2-transferrin. As the fluid reaccumulated alongside a return of nasal obstruction symptomatology, the decision was made to treat the obstructing cystic portion of the lesion with slcerotherapy. Sclerotherapy with bleomycin was successfully performed on the cystic lesion at 9 months of age. The postoperative course was uneventful. At 8-month post sclerotherapy, the family reported sustained improvement in snoring, stertor, feeding, and weight gain. On nasopharyngolaryngoscopic examination, wide patency of the oropharynx was visualized.
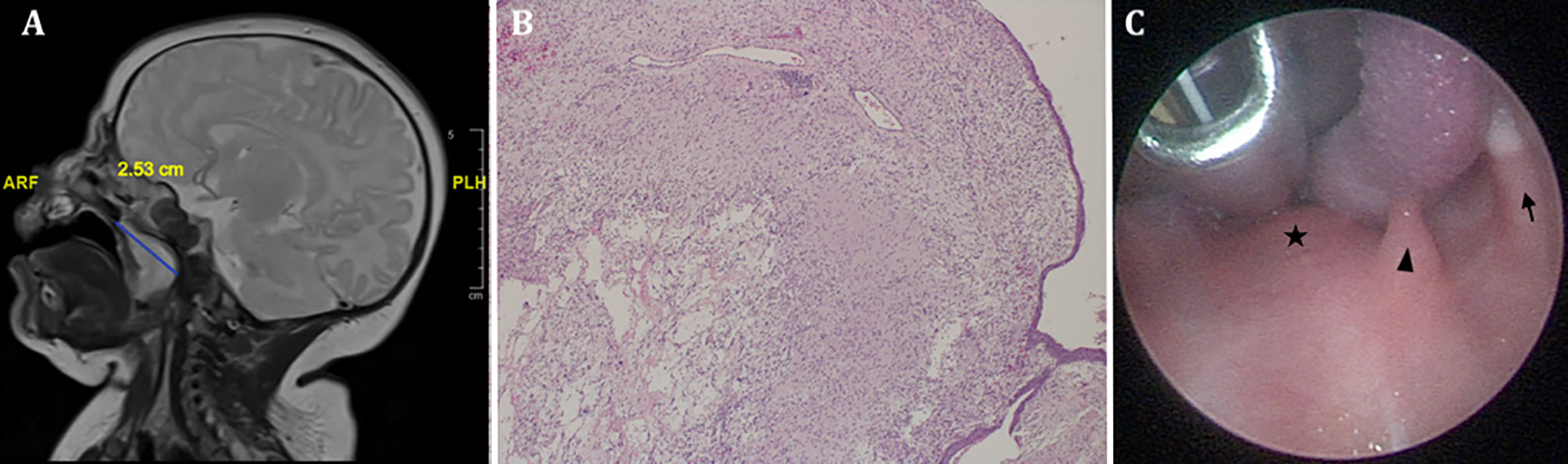
A, Magnetic resonance imaging of brain with and without contrast, T2 sequence coronal plane imaging reveals a 1.33 cm transverse lesion. T2 TSE sagittal plane imaging reveals 2.53 cm AP and 1.89 cm CC dimensions of the lesion. B, Histopathology of cystic lesion revealing mature glial tissue with cystic lesions. Hematoxylin and eosin stain; 40× magnification. C, View of oral cavity prior to aspiration and sclerotherapy. There is soft palate (star) fullness and bulge with underlying cyst. The uvula (arrowhead) is deviated toward the retromolar trigone (RMT, solid arrow) on the right.
Discussion
Embryology and Pathogenesis
There are multiple theories on the pathogenesis of heterotopic neuroglial tissue. One theory posits that during early embryo development, the frontal bones close prior to involution of the extracranial projecting neuroectoderm. This neuroectoderm is attached to surface ectoderm during this period, which explains the nasal and pharyngeal predisposition of heterotopic neuroglial tissue. 1 If a fistula is present between the intracranial and extracranial space, then it is diagnosed as an encephalocele. 6 Another theory is that there is a defect in chondrofication or ossification of the skull base that allows for extracranial heterotopic neuroglial tissue to persist. 2 A third theory hypothesizes that there is a displacement of totipotent neuronal precursors extracranially or there is abnormal migration or retention of olfactory neuroglial cells. 7
Management
Heterotopic neuroglial tissue was first described by Reid in 1852 and the histopathological finding of glial tissue in the nasopharynx was first described by Bratton and Robinson.5,7 Magnetic resonance imaging and CT imaging have become the main modalities for delineating size and location of the mass, as well as the presence of intracranial extension. Magnetic resonance imaging has replaced CT in an effort to spare the neonate early exposure to ionizing radiation.1,8 However, CT imaging may be necessary, as in this case, to determine bony defects or erosions in the skull base if MRI is indeterminate.
Most cases of heterotopic neuroglial tissue were treated surgically with transoral, transcervical, and endoscopic excision with some requiring intubation, tracheotomy, or gastrostomy to address airway compromise or feeding complications.7,9 Timing of surgery is determined by symptoms of respiratory distress or poor feeding or if the mass size is concerning.1,7,10 Proponents of early timing of surgery point to decreased distortion and erosion of facial structures by the mass as it enlarges and better swallow function and pharyngeal coordination with surgical correction. 3 However, even in recurrence and growth, asymptomatic patients often are treated with observation. 4 As was demonstrated successfully in this patient, sclerotherapy of the cystic portion of the lesion may offer a viable alternative to surgical resection.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.