
Abstract
Arthropods may become lodged inside the ear and cause considerable emotional and physical trauma. Cases of centipedes being lodged in the external auditory canal have rarely been reported. In this article, we present the case of woman who had a centipede lodged inside her right external auditory canal. Removal using a topical local anesthetic can lead to vigorous activity of the centipede, which can cause harm to the patient and clinicians. Therefore, we developed and successfully applied a practicable method that involved using a modified plastic bottle for safe centipede removal. In conclusion, centipedes can express distinct and threatening behavior, and clinicians should pay attention to the activity of the lodged centipede and possibly use the proposed method to safely remove it.
Background
In the emergency department, visits for the removal of arthropods that have crawled into the ear account for only 14% of the visits for all aural foreign body removal. 1 However, no report on aural centipede removal has been published in English. In this article, we present a rare case of a centipede entering the external auditory canal of a woman, share our experience with regard to its management, and introduce an innovative method for the safe removal of the centipede.
Case Presentation
A 31-year-old woman presented to our emergency department. She had developed sudden-onset right ear pain with loud noise in her ear when she was asleep. On visual examination, her family members had noted a black creature lodged inside her right ear, which they attempted to draw out using a flashlight, but this was ineffective. Through video-otoscopy of the right ear, we visualized a tightly coiled, brownish black arthropod-like creature with pointed legs fully occupying the right external auditory canal. Thus, a centipede was speculated to be lodged inside the patient’s right external auditory canal (Figure 1).
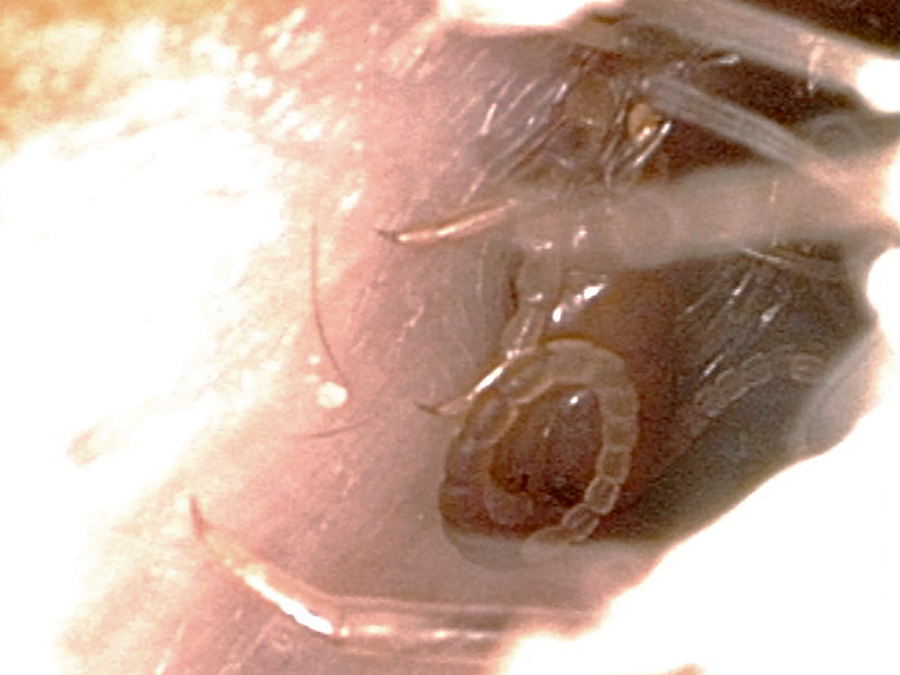
A live tightly coiled centipede-like creature noted in the right external auditory canal.
According to our past experience, when a local anesthetic is administered, centipedes are not paralyzed. Rather, they become aggravated into vigorously uncoiling and rapidly jumping out of the ear—endangering not only the patient but also clinicians. Therefore, we developed an innovative method for removing the centipede safely. We cut and removed the bottom part of an empty 500-mL plastic bottle of normal saline and created a small hole in the middle of the side of the top part of the bottle (Figure 2). This small opening of the bottle was then placed around the patient’s right ear such that it was completely sealed off. Next, a nozzle of a bottle containing 10% lidocaine (local anesthetic) was inserted though the aforementioned small hole. The lidocaine solution was then sprayed into the external auditory canal through the nozzle (Figure 3). Immediately, a black centipede measuring approximately 5 cm in length emerged out of the external auditory canal and was trapped inside the bottle. The extracted centipede had 20 arthroses and was highly mobile.
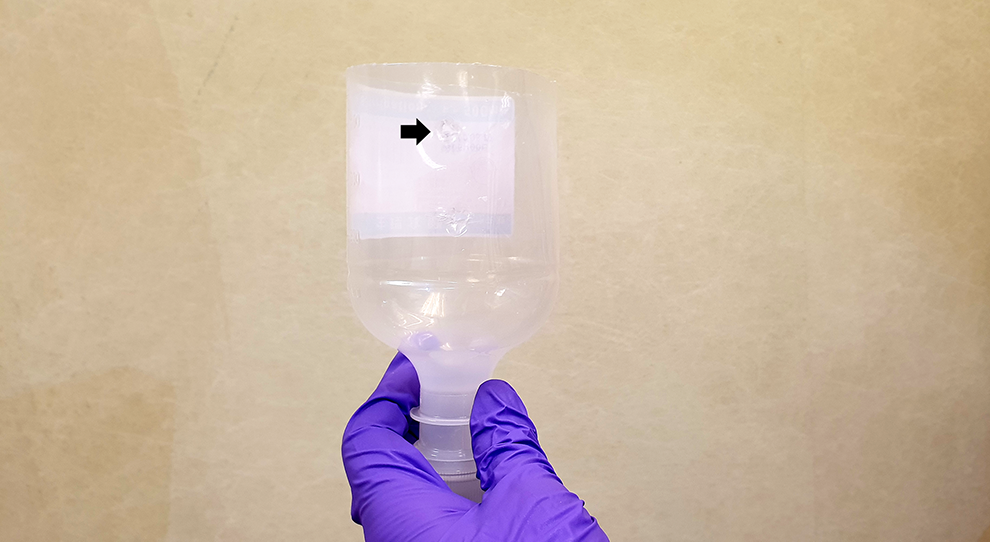
Our apparatus for centipede removal from the ear. Black arrow indicates the hole created for anesthetic delivery.
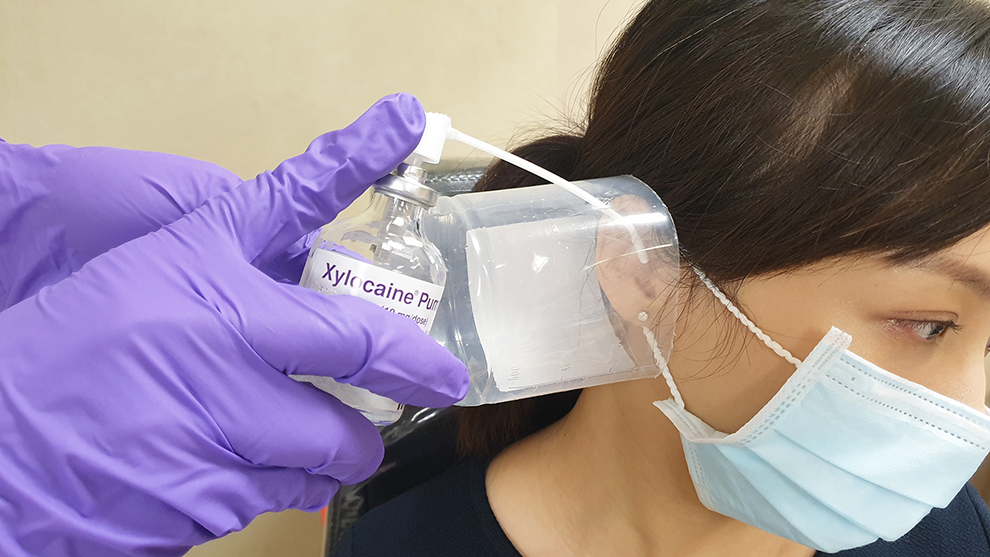
Application of our centipede removal device.
After the removal, the patient’s eardrum was found to be intact. Only some erosive wounds were noted around the external auditory canal. These wounds had healed by the time of her follow-up 1 week later.
The publication of this case report was approved by the Institutional Review Board of Chang Gung Memorial Hospital (No.: 201600449B0).
Discussion
Antonelli et al reported that arthropods represent 14% of all cases of aural foreign bodies. Cockroaches are the most commonly identified arthropods and account for nearly 50% of aural creatures. 1 In this article, we report for the first time a case of a live centipede lodged inside an ear and present a practicable and easy-to-use method for its safe removal.
Centipedes, which are typically found in tropical and subtropical regions, are mostly active at night during spring and summer. Thus far, 16 centipede species of 5 genera (Scolopendra, Rhysida, Otostigmus, Cryptops, and Colopocryptops) have been identified in Taiwan. 2 According to its length and number of body segments, the centipede extracted in the present case may have been Rhysida longipes longipes, which is a common nocturnal centipede in Southern Taiwan.
The presence of a live centipede in the external auditory canal may cause distressing noise, tenderness, and the sensation of aural fullness. This condition often requires immediate foreign body removal to obviate further damage to the middle ear structure. However, during our previous encounters with cases of centipedes lodged in the ear, we noted that centipedes exhibited some characteristics that were distinct from those of other living foreign bodies in the ear: Centipedes are photophobic arthropods and active at night; therefore, any attempt to draw them out using light may have adverse or no effects.
2
This finding may explain the reason that the patient’s family members were unable to draw out the centipede by using a flashlight. Centipedes cannot be drowned or paralyzed using topical local anesthetic. Moreover, if a centipede is tightly coiled, the anesthetic can aggravate it to vigorously uncoil, stretch, and finally, jump out of the ear.
Therefore, we developed a convenient practicable method, which involves the use of easily available material, to help clinicians smoothly and safely extract highly active creatures from the ear. Over 2015 to 2019, we have successfully used this method at our hospital in three cases of centipede removal from the ear without any complications after the procedure. When implementing our method, careful manipulation; prevention of strong light stimulation; and the implementation of protective measures such as 2-layer gloves, long-sleeve medical gowns, and surgical towels to protect the patient’s skin are recommended.
Centipede bite and venom may cause skin manifestations such as local erythema, tenderness, edema, and blisters. Lymphadenopathy, rhabdomyolysis, acute renal failure, and myocardial infarction have also been reported in some cases.3,4 The treatment for a centipede bite is symptomatic, including ice-pack application, wound care, analgesic use for pain control, and antihistamine and steroid use for pruritus. In addition, prophylactic tetanus vaccine application may be prescribed. 5
Conclusions
During removal, centipedes can cause severe damage to the external auditory canal through their vigorous activity. Clinicians should thus be careful when removing a suspected centipede-like alive foreign body lodged inside their patient’s ear. Moreover, for ensuring safe removal, the use of easy-to-make devices, such as that used in this case, is highly recommended.
Footnotes
Authors’ Note
The data used in the article were permitted by the patient with consent for publication. The publication of this case report was approved by the Institutional Review Board of Chang Gung Memorial Hospital (No.: 201600449B0).
Authors Contributions
Meng-Chang Ding contributed for article completion. Yao-Te Tsai, Ming-Shao Tsai, and Cheng-Ming Hsu contributed to draft the article. Geng-He Chang contributed to data acquisition, figure preparation, table making, critical article revision, and final approval for submission. All data during this study are included in this published article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.