
Abstract
Objective:
To evaluate the attitudes of physicians and patients toward physical examination in physically separated environments using a laryngoscopic examination model.
Materials and Methods:
Six experienced laryngologists performed laryngoscopic examinations in 30 patients in a closed-chamber examination unit. The physicians and patients were asked to compare all domains with their previous standard laryngoscopic examination experience using a 10-point visual analog scale (0, poor performance; 10, good performance), including effectiveness of communication, difficulty of examination, perception of safety against airborne transmission of COVID-19, applicability of the unit for future examinations, perception of protective environment, and overall comfort.
Results:
All laryngoscopic examinations were performed successfully. Effectiveness of communication, difficulty of examination, perception of protective environment, and overall comfort did not differ between physicians and patients (P > .05 for all comparisons). However, both physicians and patients found the examination to be difficult. While physicians evaluated the system as safe against airborne transmission of COVID-19, patients were not confident that the system was safe (8.70 ± 1.93 vs 2.87 ± 2.37, respectively, P = .001). Physicians also gave a higher score to future applicability of the unit for examinations than patients (8.90 ± 1.42 vs 7.10 ± 2.62, respectively, P = .001).
Conclusion:
Physically separating the physician and patient is a feasible method of physical examination in aerosol-contaminated environments.
Introduction
As of December 22, 2020, the World Health Organization (WHO) has reported 76 023 488 confirmed cases of COVID-19 caused by the novel coronavirus SARS-CoV-2, and 1 694 128 deaths from the disease. 1 Amnesty International has estimated that 1.4 million health care workers have been infected with SARS-CoV-2, and at least 7000 have died during the pandemic. 2 Most of these are frontline health care workers, with airborne transmission occurring during routine examinations. 3 This high rate of infection and high death rate have placed a great deal of pressure on health care workers. As the pandemic and its effects continue, there will be an increasing need for health care workers. There is a need for new insight into limiting the spread of the virus particularly among frontline health care workers, especially with regard to mitigating the risks of physical contact with patients. 4
The infection of health care workers with SARS-CoV-2 has multiple effects on health services. Although there are no specific data regarding the transmission rates among infected health care workers, from health care workers to the hospital environment, and from health care workers to uninfected patients, it is reasonable to assume that such transmission will be relatively common. Disease transmission results in several problems including deterioration of health care services and excess use of health care resources.
Transmission seems to rely on sharing the same physical environment with an infected person. We have previously designed a closed-chamber ear, nose, and throat (ENT) examination unit for ENT examinations, which are high-risk physical examinations due to the aerosol-generating capacity of endoscopic procedures. 5 The unit may be one way to help mitigate the spread of COVID-19 as it separates the physician and medical staff from the patient. Medical practice must continuously adapt to changes to improve the provision of health care services and protect both medical staff and patients from risk of infection. 6
Separating the patient from the physician represents a fundamental change in examination procedures. This study investigated the feasibility of the closed-chamber examination unit as well as the attitudes of physicians and patients to this type of examination. The unit was examined in laryngoscopy practice, as it requires effective communication, hand manipulation of endoscopes, and hand/eye coordination.
Materials and Methods
The present study was conducted at University of Health Sciences, Bakırköy Dr. Sadi Konuk Training and Research Hospital. Ethical approval was obtained from the local ethics board (approval number 2020/198). All subjects provided informed consent to participate in the study.
Over a 1-month period, patients undergoing examinations at the Laryngology Department were evaluated. Patients who required laryngoscopic examination were included in the study. Patients who had previous experience with laryngoscopy examination were selected. Patients who had not undergone a previous laryngoscopic examination, those with movement restrictions, pediatric patients, and those who did not provide informed consent were excluded. The physicians were all experienced laryngologists. All patients were examined in the closed-chamber ENT examination (Figure 1). 5

Closed-chamber ENT examination unit. 5
The technical details of the unit were as follows:
5
Dimensions 107 × 100 × 200 cm. Ultraviolet-C lamps (wavelength 254 nM) for disinfection. Air inlet in the ceiling protected by a filter. Exhaust system in the ceiling with an aspirating fan. The vented air is directed into the hospital’s central environmental suction climate system and treated from the central system. Isolation of the room to prevent the flow of air droplets outside. A Bluetooth speaker in the room to allow communication between the examiner and patient (JBL Go; Harman International Industries). An additional screen behind the patient to facilitate the physical examination, connected to a Storz Telepack system (Karl-Storz).
The initial examination was performed by one physician, and the second unit physician was blinded to the results of the previous examination. The patient entered the unit, and microphones were used to inform the patient of the examination process. Medical history was documented with the patient inside the unit. Instructions were given and complete laryngoscopic examinations were performed.
After this process, both the physician and the patient were asked to evaluate the examination compared to their previous experience with standard laryngoscopic examination using a 10-point visual analog scale (VAS) in terms of effectiveness of communication, difficulty of examination, perception of safety against airborne transmission of COVID-19, applicability of the unit for future examinations, perception of protective environment, and overall comfort.
Statistical Analyses
Statistical analyses were performed using Number Cruncher Statistical System 2007 (NCSS). Descriptive statistical methods (mean, standard deviation, median, frequency, ratio, minimum, maximum) were to evaluate the data. The normality of the distribution of quantitative data was examined by the Shapiro–Wilk test. Wilcoxon’s signed rank test was used to evaluate the responses to questions about the chamber. In all analyses, P < .05 was taken to indicate statistical significance.
Results
A total of 6 experienced laryngologists examined 30 patients. Overall, 14 (46.7%) patients were female, and the remaining 16 (53.3%) were male. The mean age was 45.00 ± 13.40 years (range 18-76 years). All laryngoscopic examinations were successfully completed. The scores for effectiveness of communication, difficulty of examination, perception of safety against airborne transmission of COVID-19, and overall comfort did not differ between patients and physicians (P > .05 for all comparisons; Table 1). However, both physicians and patients found the examination to be difficult. While physicians evaluated the system as safe against airborne transmission of COVID-19, patients were not confident in the safety of the system (8.70 ± 1.93 vs 2.87 ± 2.37, respectively, P = .001). Physicians also gave a higher score to future applicability of the unit for examinations than patients (8.90 ± 1.42 vs 7.10 ± 2.62, respectively, P = .001).
Ratings of Closed-Chamber Examination Unit by Physicians and Patients.
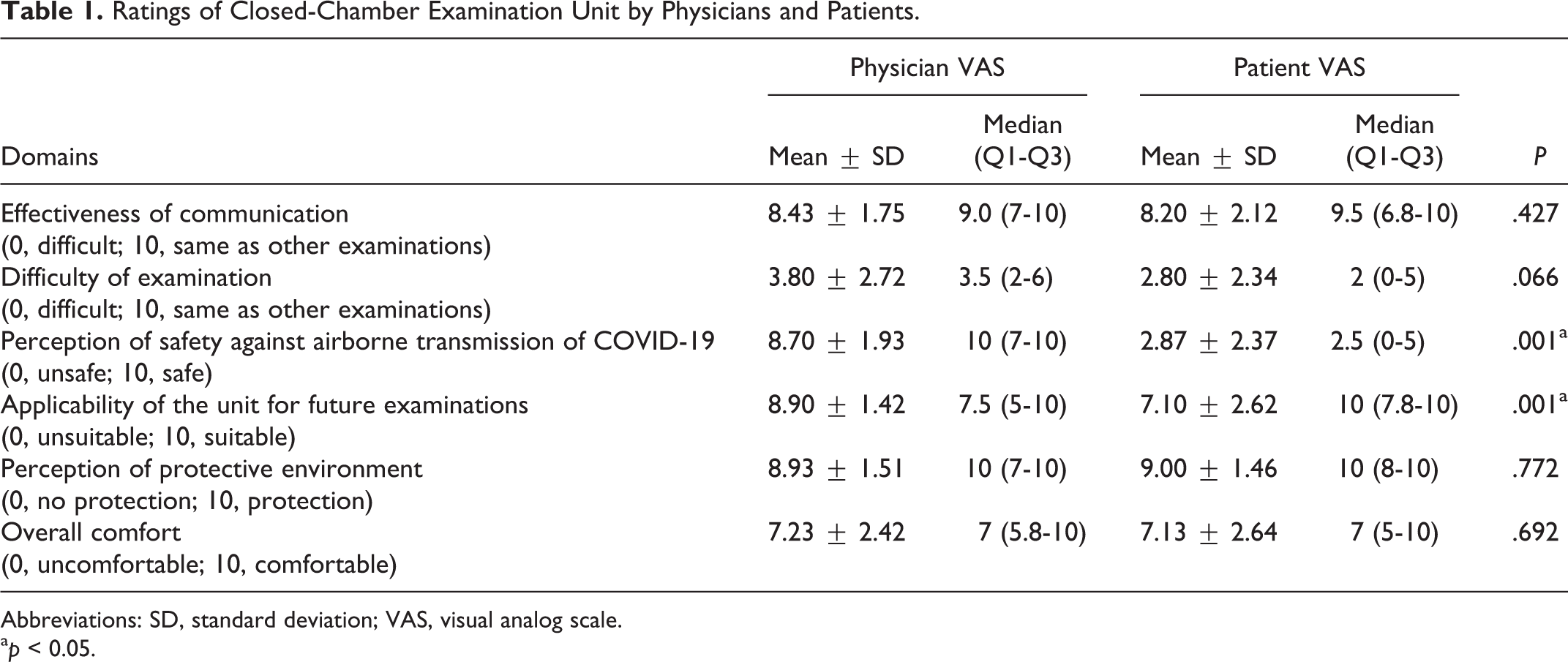
Abbreviations: SD, standard deviation; VAS, visual analog scale.
ap < 0.05.
Discussion
The present study assessed the perceptions of physicians and patients regarding physical examination in separated environments. Physicians felt that examining patients in a closed chamber provided safety and would be applicable for examinations in the future.
With the current SARS-CoV-2 pandemic, there is increasing emphasis on the risk for aerosol transmission of viral infections. In addition to influenza, a number of emerging viruses have been highlighted over the last several years, including rhinovirus type C, human bocavirus, human metapneumovirus, and so forth.7,8 An epidemiological study performed in China in 2019 indicated 2 peaks of coronavirus infections in 2016 and 2018, and suggested the likelihood of a new peak in subsequent years. A possible increase in number of infections is also expected for human bocavirus. 8 The current pandemic has shown that we should expect future pandemics. The same is also true in the case of biological attacks or infections by other organisms or bacterial infections, such as plagues, and so forth. With increase in the number of cases of infectious diseases, particularly the risk for possible future pandemics, novel methods are required to reduce disease transmission, especially among health care workers.
In the current pandemic, the WHO has reported that 10% of infections are in health care workers. There is also an increase in mortality rate of health care workers from COVID-19. 9 In aerosol-contaminated environments, health care workers are at higher risk than ordinary members of the community. Health care workers encounter several problems, including shortages of Personal Protective Equipment (PPE), restriction of daily work routine, and concerns regarding their own health. 4 Although not a direct focus of this study, a recent article also indicated that COVID-19 exacerbates violence toward health care workers due to various underlying causes. 10 There is a risk of transmission between health care workers in hospitals. Infected health care workers also affect the remaining number of health care workers. Transmission and illness of health care workers increase the workload and pressure on their uninfected coworkers. When a health care worker is infected, the work hours and shifts of their coworkers increase, further increasing the risk of transmission among the remaining staff. Health care workers are also sources of community transmission, but the percentage of such cases is not yet known. 3 This begins a vicious cycle that even the strongest medical systems cannot overcome.
Several vaccines have been developed, but they have several potential problems related to degree of effectiveness and side effects. It is also not clear whether vaccination can elicit a long-term immune response to SARS-CoV-2. In the absence of an effective vaccine, basic fundamental solutions to prevent airborne transmission are required. For example, simple masking has been shown to decrease the transmission of disease, reduce rates of symptomatic and asymptomatic infection, and decrease the rate of spread within the community. 11 In addition, changes to the physical environment may also help to reduce the transmission of COVID-19.
Simple masks and face coverings are the most basic solution available to health care workers. Even when coming into contact with infected patients, use of appropriate PPE is related to prevention of infection. This highlights the need for minimum/protected contact with infected patients. 12 The scarcity of PPE has also occurred almost all over the world. To avoid aerosol transmission, protect health care workers, and decrease the need for PPE use, we designed a closed-chamber examination unit for endoscopic examination. Separating the physician from the patient is a novel concept, and can be considered an option for future pandemics. This system has a number of advantages, including the lack of PPE requirement, continuous examination opportunity, and prevention of proximity-related transmission. To understand the feasibility of this system, this study evaluated the attitudes of physicians and patients toward this new examination concept.
The results indicated that communication between the physician and patient can be achieved effectively. However, both physicians and patients noted that the examination was more difficult than under standard conditions. Physicians rated the system highly with regard to safety and future applicability. Overall, both physicians and patients noted that the system was protective and comfortable.
In the future, we plan to combine multiple units together (Figures 2–4). The units can be constructed rapidly and located in any place. The use of these isolated units will contribute to the continuation of health care services with reduced risk for infectious disease transmission. The closed chamber can also serve as a small examination unit in the event of natural or biological disasters, such as earthquakes, disease outbreaks, and so forth. In underdeveloped countries, it will be possible to construct such closed chambers in rural areas to allow examinations to be performed without risking disease transmission.
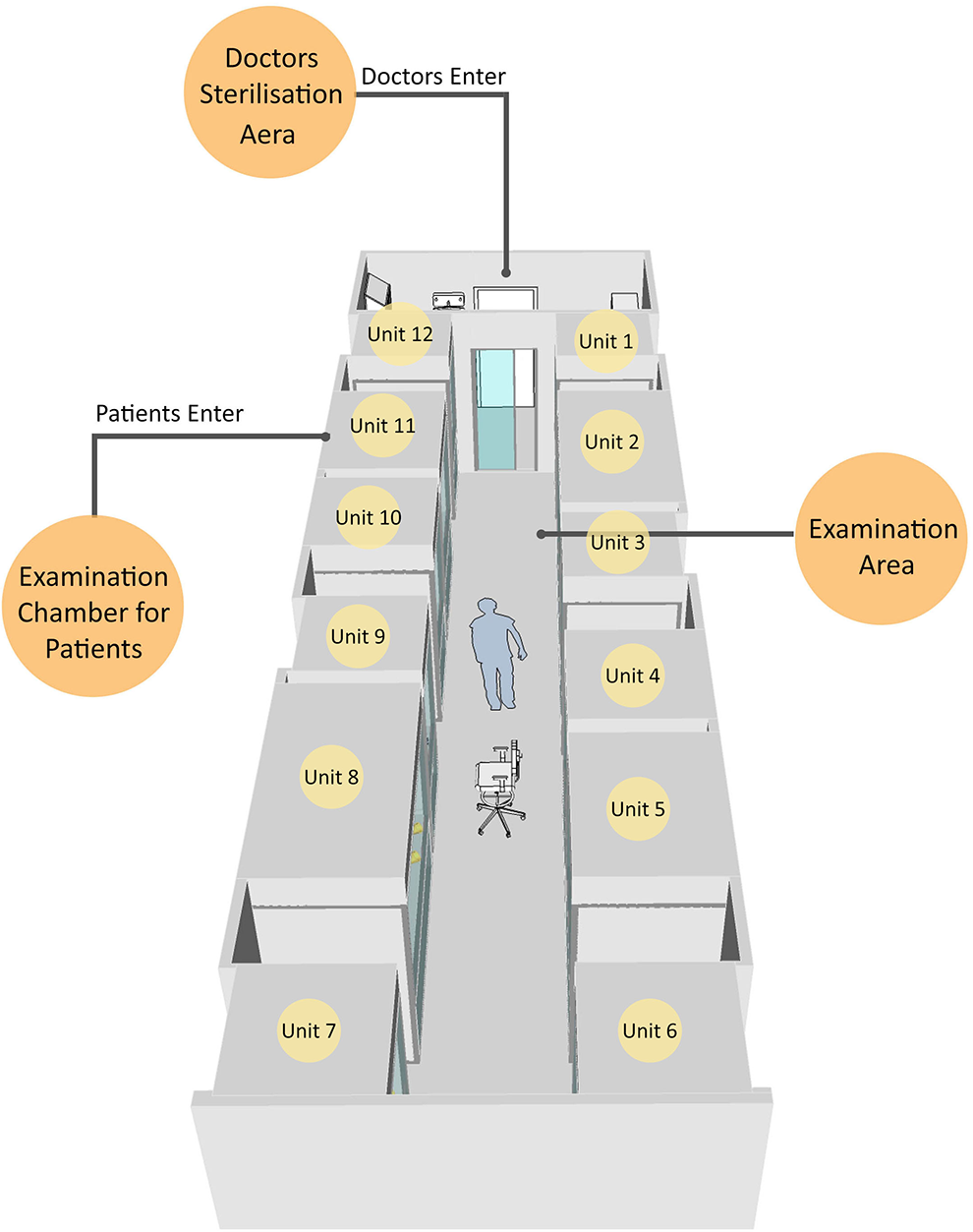
Type 1 design of examination unit.
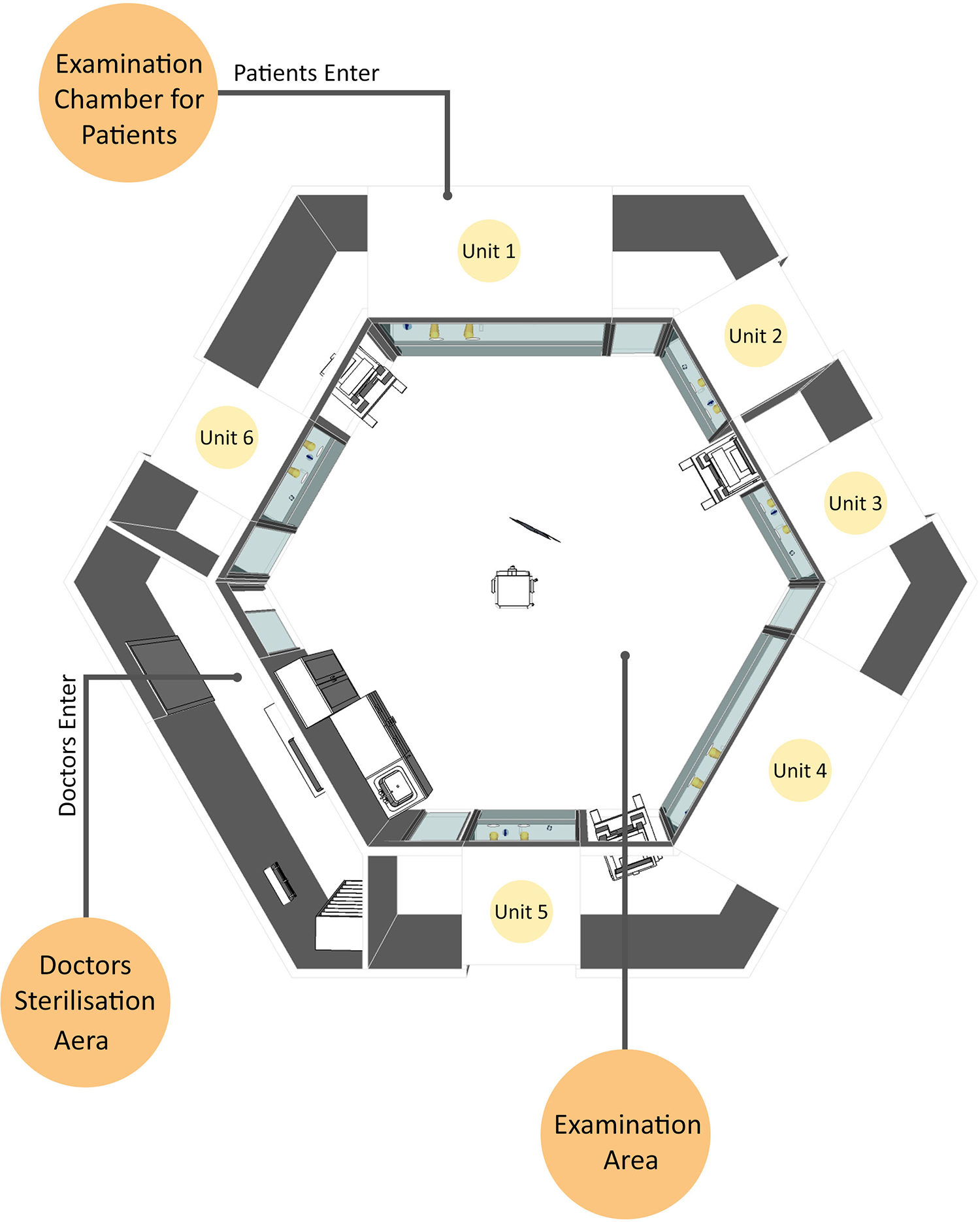
Schematic drawing of type 2 examination unit.
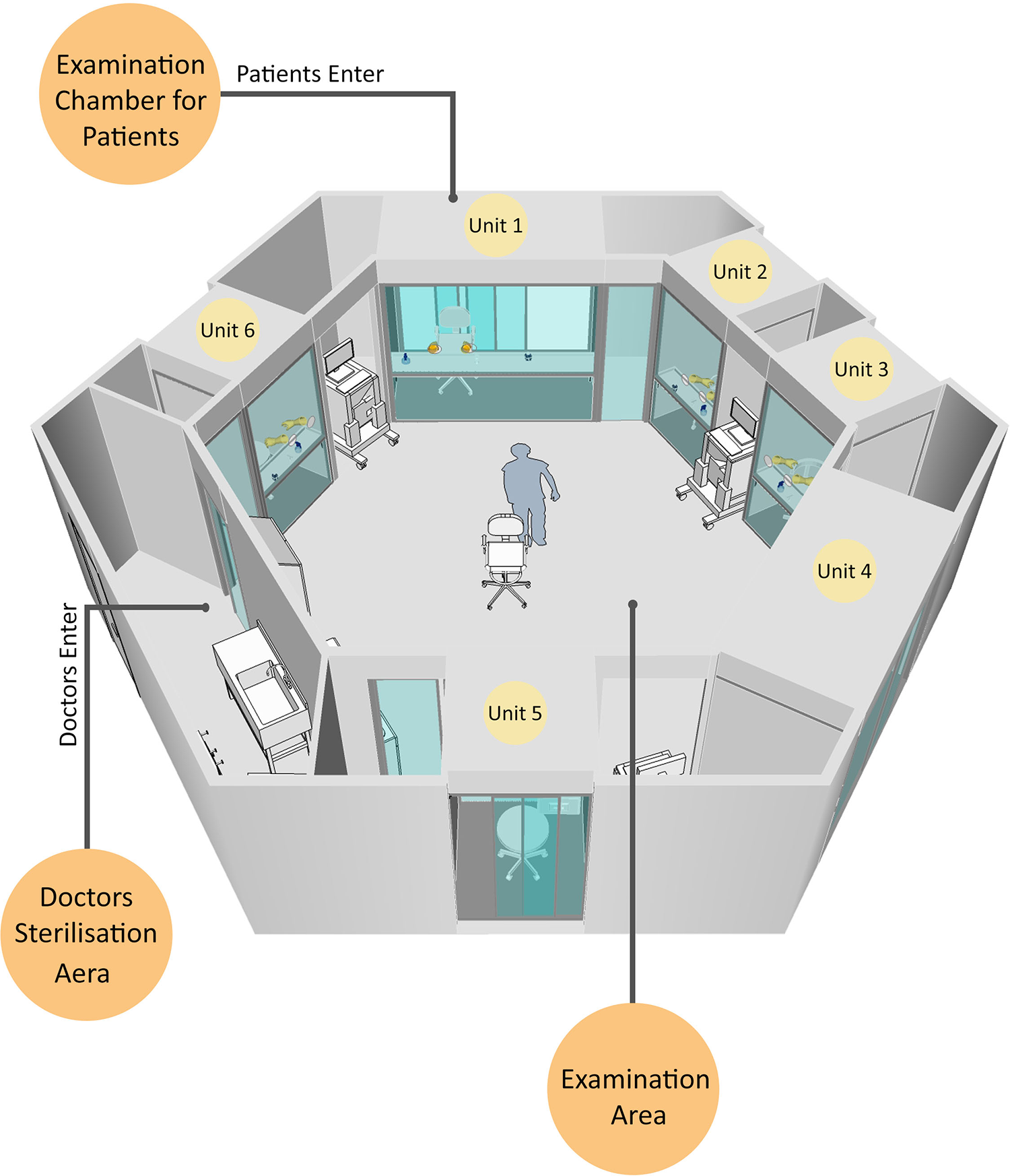
Type 2 design of examination unit.
This study had some limitations in that we cannot yet provide the cost of construction of this unit, and we also did not examine its use in other types of examinations.
Conclusion
Separating the physician and patients did not affect the overall quality of physical ENT examination. The new examination concept will be improved further and modified according to needs. The system may solve many of the problems related to risk of aerosol transmission and may be applicable to other types of contaminated environments.
Footnotes
Authors’ Note
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.