
Abstract
Background
Aerosol generating medical procedures (AGMPs) present risks to health care workers (HCW) due to airborne transmission of pathogens. During the COVID-19 pandemic, it is essential for HCWs to recognize which procedures are potentially aerosolizing so that appropriate infection prevention precautions can be taken. The aim of this literature review was to identify potential AGMPs in Otolaryngology - Head and Neck Surgery and provide evidence-based recommendations.
Methods
A literature search was performed on Medline, Embase and Cochrane Review databases up to April 3, 2020. All titles and abstracts of retrieved studies were evaluated and all studies mentioning potential AGMPs were included for formal review. Full text of included studies were assessed by two reviewers and the quality of the studies was evaluated. Ten categories of potential AGMPs were developed and recommendations were provided for each category.
Results
Direct evidence indicates that CO2 laser ablation, the use of high-speed rotating devices, electrocautery and endotracheal suctioning are AGMPs. Indirect evidence indicates that tracheostomy should be considered as potential AGMPs. Nasal endoscopy and nasal packing/epistaxis management can result in droplet transmission, but it is unknown if these procedures also carry the risk of airborne transmission.
Conclusions
During the COVID-19 pandemic, special care should be taken when CO2 lasers, electrocautery and high-speed rotating devices are used in potentially infected tissue. Tracheal procedures like tracheostomy and endotracheal suctioning can also result in airborne transmission via small virus containing aerosols.
Background
In the era of globalization, infectious disease outbreaks have brought unprecedented challenges to the medical community. Coronavirus disease 2019 (COVID-19), the clinical condition caused by infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), rapidly became the world's 6th public health emergency of international concern (PHEIC) declared by the World Health Organization since 2009 [1]. The other PHEICs were the swine flu in 2009, polio in 2014, Ebola virus in 2014 and 2018–20, and Zika virus in 2016 [1]. SARS, small pox and wild type poliomyelitis are automatic PHEICs and do not require declaration from the WHO [2].
Although the main environmental route of transmission of SARS-CoV-2 is through droplets and formites/surfaces, there is a potential risk of virus spread in smaller aerosols during various medical procedures causing airborne transmission [3–6]. “Airborne transmission” refers to transmission of infection via small (< 5-10um) inspirable aerosols over extensive distances, whereas “droplet transmission” refers to transmission of infection by (larger) aerosols over short distances directly from the infected person to the susceptible person [7, 8].
Various procedures performed by Otolaryngologists to assess and/or treat patients may generate aerosols from areas of high viral shedding, such as the nasal and oral-pharyngeal cavity [6, 9]. Such aerosol generating medical procedures (AGMPs) can lead to close proximity transmission of aerosols, but also in the spread of small aerosols over extensive distances resulting in airborne transmission. According to colleagues in other countries such as China, Italy, and Iran, Otolaryngologists are among the highest risk group of contracting viruses while performing upper airway procedures without appropriate Personal Protective Equipment (PPE) [10]. As there is worldwide limited availability of PPE, it is essential to distinguish which procedures justify the use of high level, airborne precautions. The objective of this literature review is to identify potential AGMPs in Otolaryngology - Head and Neck Surgery (OHNS) and provide evidence-based recommendations.
Methods
This manuscript followed the published methodology of developing an evidence-based review with recommendations by Rudmik et al. (2011) [11]. A literature search was performed on Medline, Embase and Cochrane Review Databases from inception to April 3, 2020. Given aerosol and droplet terminology has been used interchangeably in the literature, the search included both terms. A screening literature search was first performed using the search term (aerosol* or droplet*) and (procedure or treatment or surgery). The authors, J.H., A.H., C.L., J. P, YWQ, and P.Y. reviewed the articles for topics that pertained to the realm of the head and neck region. All abstracts were reviewed and the following inclusion criteria was applied: English articles, clinical or experimental studies involving procedures in the head and neck region. Studies were excluded if they were opinion papers, review papers, or if only the abstract was published (no manuscript available). This first review of papers led to the following procedures being identified: nasal endoscopy, nasal packing and treatment of epistaxis, endoscopic sinonasal and anterior skull base surgery, CO2 laser ablation, electrocautery, tracheotomy, endotracheal suctioning, oropharyngeal surgery, head and neck reconstruction surgery, dental procedures, mastoid surgery and nebulizer/atomizer. A second focused literature search was performed for each of the aforementioned procedures using the search term (aerosol* or droplet*) and the synonyms of the procedure (e.g. (aerosol or droplet) and (mastoidectomy or mastoid* or mastoid surgery)). The same inclusion and exclusion criteria were applied except this time procedures that were in the head and neck region but not performed by an Otolaryngologist were removed (example: irrigation wash in dental procedure). This was done in order to ensure no further articles were missed on the first search and to keep articles chosen were relevant to the audience of interest. Review papers were also cross referenced to ensure all studies were identified.
The included articles were categorized into various potential AGMP procedures. In this review an AGMP is defined as a medical procedure which has the potential to generate small (< 5-10um) aerosols that can travel greater than 2 m, and therefore an AGMP confers the potential for airborne transmission. In contrast, we defined droplet transmission as involving (larger) aerosols over short distances (< 2 m) directly from the infected person to the susceptible person via mechanisms such as coughing and sneezing. Each AGMP procedure category was assigned to a practicing Otolaryngologist Head & Neck Surgeon to review the evidence found in the articles, grade the evidence of the articles and develop recommendations for practice. The recommendations were created based on study design, the quality of research, directness of evidence and finally the balance between the potential harm of the procedure and the quality of evidence [12]. Since the potential harm of aerosolizing viable pathogens can have a large impact on the safety of HCWs, a strong recommendation can still be warranted despite low or very low confidence in effect estimates [12]. Direct and high quality evidence was defined as studies evaluating directly, or indirectly particles/aerosol concentrations in air samples. Indirect evidence could be obtained from experimental cadaver models, or retrospective epidemiological data. The manuscript then underwent an iterative review process in the following order: M. L, C.D., J.L., D.D.S., L. S and A.T.
Results
The first literature search retrieved 44,110 articles (titles and abstracts), which were screened for potential eligibility. From this, 111 papers fit the inclusion/exclusion criteria, categorized into similar procedures and the second focused search was performed leading to 10 categorical procedures for review (oropharyngeal surgery, head and neck reconstruction surgery, dental procedures summarized under one heading for simplicity) (Fig. 1). The procedures and their evidence were then summarized below.

Evidence Based Review Search Strategy. OHNS = Otolaryngology – Head and Neck Surgery
Nasal Endoscopy
Characteristics of included studies on nasal endoscopy
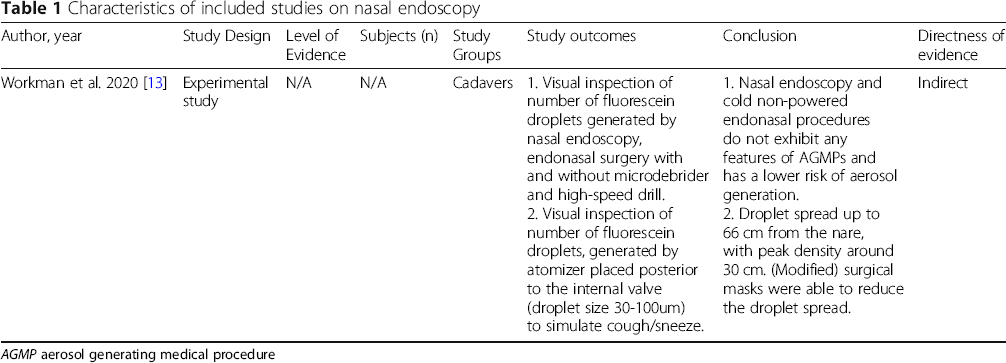
AGMP aerosol generating medical procedure
Aggregated Evidence: Grade D: one experimental study.
Recommendation:
Nasal endoscopy can cause coughing and sneezing of the patient, which may result in droplet transmission. It is unknown if this procedure can also lead to airborne transmission of small aerosols over extensive distances. Nasal endoscopy should be considered as a droplet forming procedure and as a potential AGMP.
Strength of recommendation: low.
Nasal Packing and Treatment of Epistaxis
Characteristics of included studies on nasal packing and treatment of epistaxis

RCT randomized control trial
AGMPaerosol generating medical procedure
Aggregated Evidence: Grade C: one level 3 study, and two indirect, descriptive cross-sectional studies.
Recommendation: There is clinical evidence that treatment of epistaxis can cause coughing and sneezing of the patient, which may result in droplet transmission. It is unknown if these procedures can also lead to airborne transmission of smaller aerosols over extensive distances. Treatment of epistaxis and nasal packing should be considered as droplet forming procedures and as potential AGMPs.
Strength of recommendation: moderate.
Endoscopic Sinonasal and Anterior Skull Base Surgery
Characteristics of included studies on endoscopic sinonasal and anterior skull base surgery

Aggregated Evidence: Grade D: one experimental study.
Recommendation:
Based on limited evidence and clinical reasoning, powered instruments, which include the microdebrider and the drill, can result in droplet transmission and airborne transmission, and should be considered as droplet forming procedures and as AGMPs. Cold non-powered procedures are less likely to result in droplet or airborne transmission, as the patient is paralyzed during the procedure, and should be considered as potential droplet forming procedures, but not as AGMPs.
Strength of recommendation: low.
CO2 Laser Ablation
Characteristics of included studies on CO2 laser ablation

PCR polymerase chain reaction
HPV Human papilloma virus
DNA deoxyribonucleic acid
Aggregated Evidence: Grade C: two direct, cross-sectional studies, one indirect level 4 study, and two experimental studies.
Recommendations: Consistent, direct evidence indicates that CO2 laser ablation of infected tissue can result in the spread of small, virus containing, aerosols. It is unclear if these aerosols can spread over longer distances, but given the small particle size generated by laser ablation, it is plausible. Laser ablation (CO2) should be considered as a droplet forming procedure and an AGMP.
Strength of recommendation: strong.
Electrocautery
Characteristics of included studies on electrocautery

PCR polymerase chain reaction
HPV Human papilloma virus
DNA deoxyribonucleic acid
HIV Human immunodeficiency virus
In contrast, Subbarayan et al. (2019) assessed the presence of viral DNA in electrocautery smoke produced during the resection of HPV16 positive oropharyngeal cancers [25]. PCR analysis of intraoperative smoke samples obtained from 6 different cases did not reveal HPV16 DNA [25]. This is in line with an experimental study assessing HIV-1 transmission via electrocautery smoke; the surgical smoke generated by cauterization of HIV-1 containing blood was collected and after 4 weeks of culturing no virus could be detected [28].
Aggregated Evidence: Grade C: four, direct cross-sectional studies, two experimental studies.
Recommendations: There is consistent, direct evidence indicating that electrocautery can result in small aerosols with potential spread over longer distances. It is uncertain if this can actually lead to clinically relevant transmission of viable pathogens. Electrocautery in tissue with potential high viral loads, i.e. aerodigestive tract, should be considered as a droplet forming procedure and as an AGMP.
Strength of recommendation: moderate.
Tracheotomy
No studies performed air sample analyses during tracheotomies. In the 2009 retrospective cohort study by Chen et al. (2009), 6 of 17 HCWs performing tracheostomy developed SARS, conferring an odds ratio of 4.15 (univariate analysis 1.50 to 11.50, p < 0.01) [29]. However, in their multivariate analysis, tracheotomy was not a significant prognostic factor for the development of SARS [29]. It is unknown whether these infected HCWs were wearing full aerosol PPE, while performing the tracheotomies [29].
Characteristics of included studies on tracheotomies

HCWs health care workers
SARS severe acute respiratory syndrome
OR odds ratio
Aggregated Evidence: Grade D: one level 3 study, and three level 4 studies with clinical reasoning.
Recommendations: There is only indirect evidence and expert opinion suggesting that tracheotomies are high risk of airborne transmission. Although there is paucity of evidence, tracheotomy should be considered as a droplet forming procedure and as an AGMP.
Strength of recommendation: strong.
Endotracheal suctioning
Characteristics of included studies on endotracheal suctioning

PICU pediatric intensive care unit
RT-PCR real time polymerase chain reaction
DNA deoxyribonucleic acid
HCWs health care workers
SARS severe acute respiratory syndrome
Aggregated Evidence: Grade C: two direct cross-sectional studies, one level 3 and two level 4 studies and two environmental studies.
Recommendations: There is consistent evidence that endotracheal suctioning can result in the spread of small aerosols containing viable pathogens. Long distance spread of small aerosols remains possible under certain conditions. Endotracheal suctioning should be considered as a droplet forming procedure and as an AGMP (especially if the patient is mechanically ventilated).
Strength of recommendation: strong.
Oropharyngeal Surgery and Dental Procedures
Characteristics of included studies on oropharyngeal surgeries and dental procedures
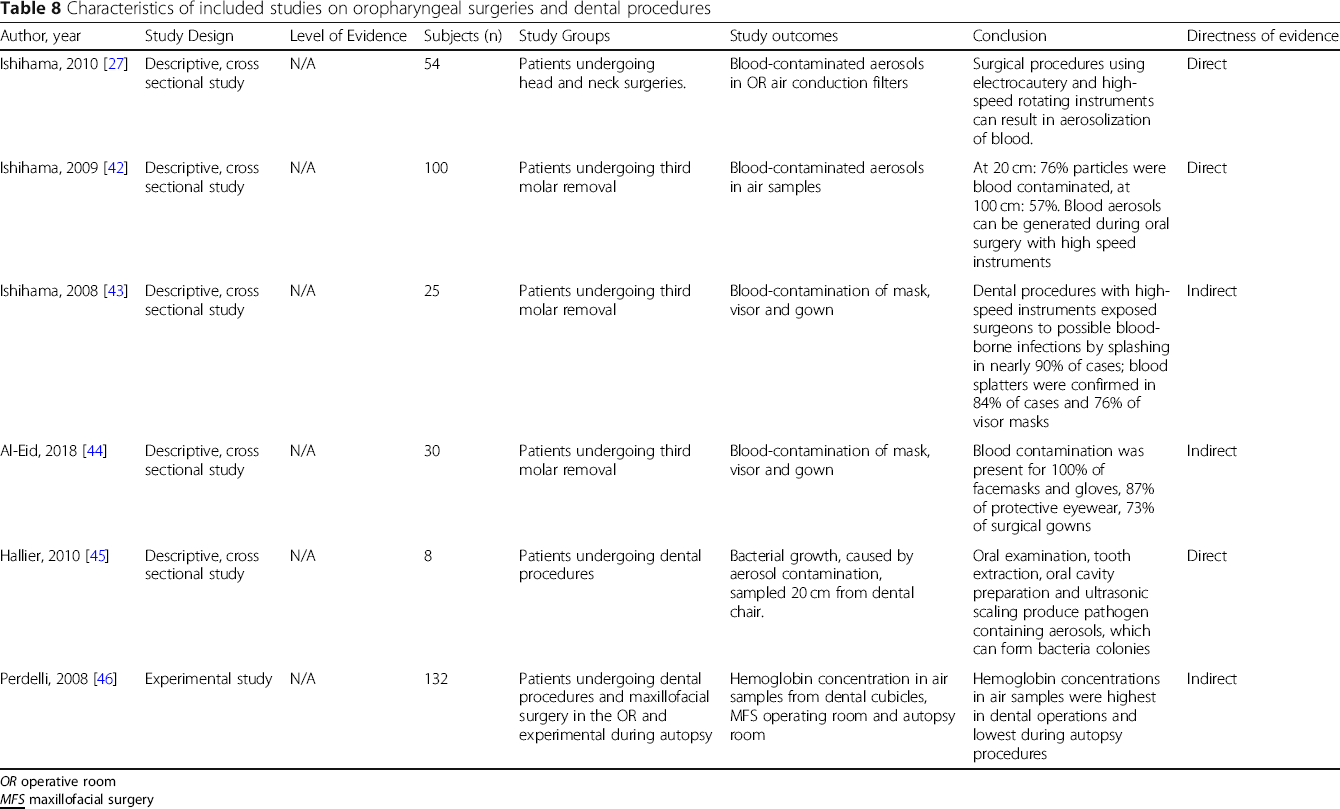
OR operative room
Aggregated Evidence: Grade C: three direct, and two indirect cross-sectional studies, and one experimental study.
Recommendations: Consistent and direct evidence indicates the risk of small aerosol formation when high-speed rotating instruments are used in the oral cavity. One study also suggests that these aerosols can become airborne. The use of electrocautery and high-speed rotating instruments (powered instruments) within the oral cavity and pharynx should be considered as droplet forming procedures and as AGMPs.
Strength of recommendation: strong.
Mastoid Surgery
Characteristics of included studies on mastoid surgery

RPM revolutions per minute
Aggregated Evidence: Grade D: three experimental studies.
Recommendations: Indirect evidence from studies with varying quality indicate that drilling of the mastoid generates small aerosols. Mastoidectomy should be considered as a droplet forming procedure and an AGMP.
Strength of recommendation: moderate.
Nasal Nebulizer/Atomizers
Characteristics of included studies on nebulizers/atomizers

Aggregated evidence: Grade D: one experimental study.
Recommendations: One experimental study suggests that the nozzle tips of powered atomizers can get contaminated but no evidence that the action of the atomizer generates aerosols from the patient. The use of atomizers/nebulizers should be considered droplet forming procedures given the risk of coughing and sneezing but not an AGMP.
Strength of recommendation: low.
Discussion
Surgical procedures using (CO2) laser vaporization, electrocautery and/or high-speed powered rotating instruments, like microdebriders, drills and saws, can result in airborne transmission of aerosols and should therefore be considered AGMPs. In addition, endotracheal procedures like endotracheal suctioning and tracheotomies should also be considered AGMPs as high tracheal airflow can result in airborne transmission of small aerosols. Nasal endoscopy, epistaxis management and in-office sinonasal procedures can induce sneezing and coughing of the patient. Although sneezing and coughing is considered to result in mainly droplet transmission, HCWs should be aware that the resulting clouds also contain small, inspirable aerosols, which can impose a risk, when they are working in close proximity to the patient [4, 7, 8].
For the protection of HCWs during this COVID-19 pandemic, it is not only essential to recognize which procedures are aerosolizing, but physicians should also be aware of the distribution of SARS-CoV-2 throughout the body. The highest viral loads of SARS-CoV-2 have been found in the upper and lower airways, but the virus has also been identified in feces [53]. Viral RNA has even been found in the blood of both symptomatic and asymptomatic COVID-19 patients, and as such, inhaled aerosol of blood may potentially transmit infection [54, 55]. SARS-CoV-2 appears to be quite sensitive to temperature, being largely inactivated at temperatures above 70 °C [56]. This is important given the high temperature of electrocautery may result in nonviable virus in the plume. This matter is of great importance, not just to our specialty, but to all surgeons operating in this era.
For Otolaryngologists performing aerosol generating procedures, guidelines on PPE use have been suggested in SARS-CoV-2 positive or suspected patients [57, 58]. Although coughing and sneezing mainly results in the emission of larger droplets, the risk of inhaling potentially smaller SARS-CoV-2 infected aerosols should not be neglected, especially if the HCW is in close proximity. For in-office endonasal procedures and nasopharyngoscopy, in the vast majority of patients, standard level 2 airborne PPE, including N95 masks are recommended. We further recommend keeping as much distance from the patient by using video endoscopy instead of the eye-piece. On the other hand, aerosolizing procedures in SARS-CoV-2 positive or suspected patients warrant extreme airborne precautions and level 3 PPE is recommended by our working group, which include either powered air purifying respirators (PAPR) or body/face/eye protection with N99/FFP3 respirators (99% filtration rate, or 95% if not available) [57, 58]. In addition, it is recommended that AGMPs are performed in negative pressure rooms to minimize the risk of spread of contaminated aerosols.
One of the major limitations of this review is the fact that most recommendations can only be based on evidence from small, descriptive case-series, experimental studies or indirect retrospective cohort studies. Even if direct evidence was available, the clinical applicability of the various study results can be questioned during the current COVID-19 pandemic. Virus kinetics can differ significantly and this not only includes the potential to survive in aerosols, but also its sensitivity to heat and shear stress during drilling. Extrapolating evidence obtained from studies investigating the potential of airborne transmission and infection of HPV or influenza virus might not hold true for SARS-CoV-2.
Given the limitations of the available research and knowledge surrounding this topic, we recommend HCWs err on the side of caution. As the risks of potential infection with SARS-CoV-2 are significant, a careful balance between the potential harms of the procedure and quality of the available evidence was considered in these recommendations. Therefore, a strong recommendation that a procedure is an AGMP can be provided despite the paucity of high quality and direct evidence. For example, regarding endoscopic use of microdebriders, due to high-speed rotation of the blade, the authors recommend the microdebrider be considered an AGMP as clinical experience intraoperatively conveys frequent microdebrider suction port plugging. To minimize the risk, we suggest the placement of a suction in the nose or suction catheter in the nasopharynx either in the contralateral nostril or via the oropharynx. The use of the suction near the surgical field is also recommended when using electrocautery or the CO2 laser. Furthermore, given the evidence that endotracheal suctioning is an AGMP, there is a similar theoretical risk of fenestrated suction use in the oral, ear and nasal cavity, for which we suggest the use of level 2 PPE precautions.
Summary of included procedures and recommendations

AGMP aerosol generating medical procedure
Y yes
N no
Conclusion
During the COVID-19 pandemic, tracheotomy, endotracheal suctioning, the use of high-speed rotating devices, CO2 lasers and electrocautery on aerodigestive tissue should be considered AGMPs.
Footnotes
Acknowledgements
The authors gratefully acknowledge Dr. Brian Westerberg for his editorial comments.
Authors’ contributions
All authors reviewed the literature, gathered and analyzed information and data. AT, AA, CD, DS, LS, JL, and ML made major contributions in writing the manuscript. All authors have read and approved the final manuscript.
Funding
The authors received no specific funding for this work.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.