
Abstract
Angioleiomyomas are smooth muscle masses originating from blood vessel tunica media. This is a rare tumor, comprising less than 1% of benign sinonasal cavity tumors. Failure to recognize and surgically excise nasal angioleiomyomas can result in lesion recurrence. We present 2 new cases of nasal septum angioleiomyoma at a single institution. Additionally, both cases underwent septal and nasal surgery. Due to the nonspecific clinical and imaging findings, a high index of suspicion is needed to diagnose nasal septum angioleiomyoma, often requiring histopathological verification. Preferred treatment is complete surgical excision. From our experience, concurrent corrective septal and sinus surgery can be completed with tumors less than 1.0 cm in size.
Introduction
Angioleiomyoma is a benign, vascular smooth muscle tumor which rarely presents in the nasal cavity. Since the first reported case of sinonasal angioleiomyoma by Maesaka in 1996, only 68 additional cases have been recorded worldwide. Most common reported locations of sinonasal angioleiomyoma growth include the inferior turbinates, septum, and vestibule. Women are more often affected than men, and common presenting symptoms include epistaxis and nasal obstruction. We present 2 new cases of nasal septum angioleiomyoma from a single institution, review diagnostic steps, and discuss the implications of tumor removal with concurrent septal and sinus surgery.
Case Reports
Patient 1
A 66-year-old male presented to the clinic for evaluation of a 5-year history of nasal obstruction and difficulty breathing through his nose. Symptoms were gradually increasing in severity. His medical history included hypertension, and he reported no major surgical history.
Physical examination revealed an obstructive mass in the right nasal cavity and significant left septal deviation. Computed tomography (CT) confirmed the presence of a right nasal lesion and showed moderate mucosal thickening of the maxillary sinuses bilaterally (Figure 1). A preoperative diagnosis of chronic sinusitis with nasal polyposis was made.
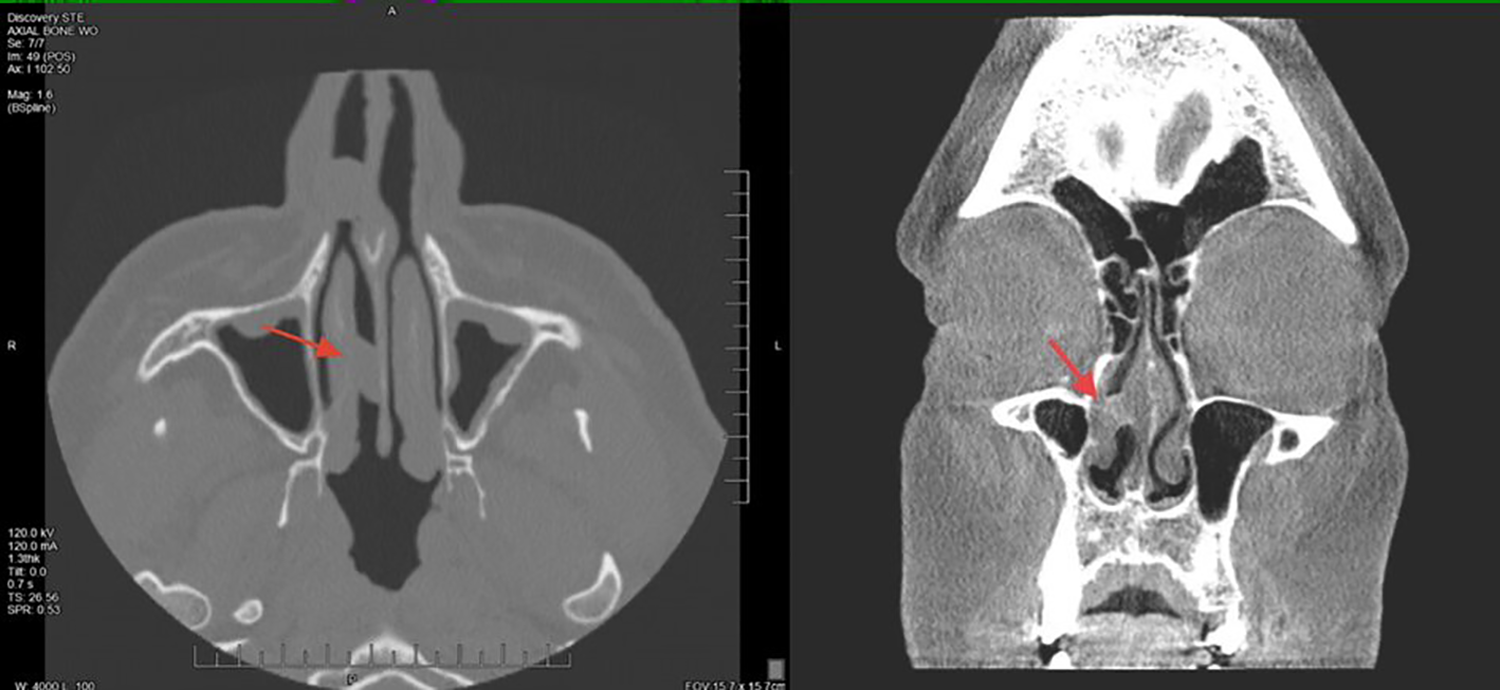
Left side shows a noncontrast axial computed tomography (CT) image of a right nasal septal mass (depicted by the red arrow) completely obstructing the nasal cavity in patient 1. Right side shows a noncontrast coronal computed tomography (CT) image of a right nasal septal lesion (depicted by the red arrow) in patient 2.
The patient was scheduled for septoplasty, sinus surgery, and excision of the nasal lesion under general anesthesia. Intraoperatively, the nasal lesion was noted to originate from the nasal septum and was located in the area of Kiesselbach’s plexus. The lesion was completely dissected off the septum, and the specimen was sent for histopathological examination. A mucoperichondrial flap was elevated at the site of excision. The patient completed a septoplasty with bilateral maxillary antrostomy, bilateral anterior ethmoidectomy, bilateral antral lavage, and bilateral coblation of inferior turbinates.
The gross specimen consisted of a pink-tan, rubbery tissue measuring 1.0 × 0.8 × 0.6 cm. Histopathologic evaluation revealed sections of nonkeratinizing squamous and respiratory type mucosa overlying a circumscribed proliferation of thick-walled blood vessels with lobular architecture (Figure 2). No cellular atypia was seen. A diagnosis of nasal septal angioleiomyoma was made.
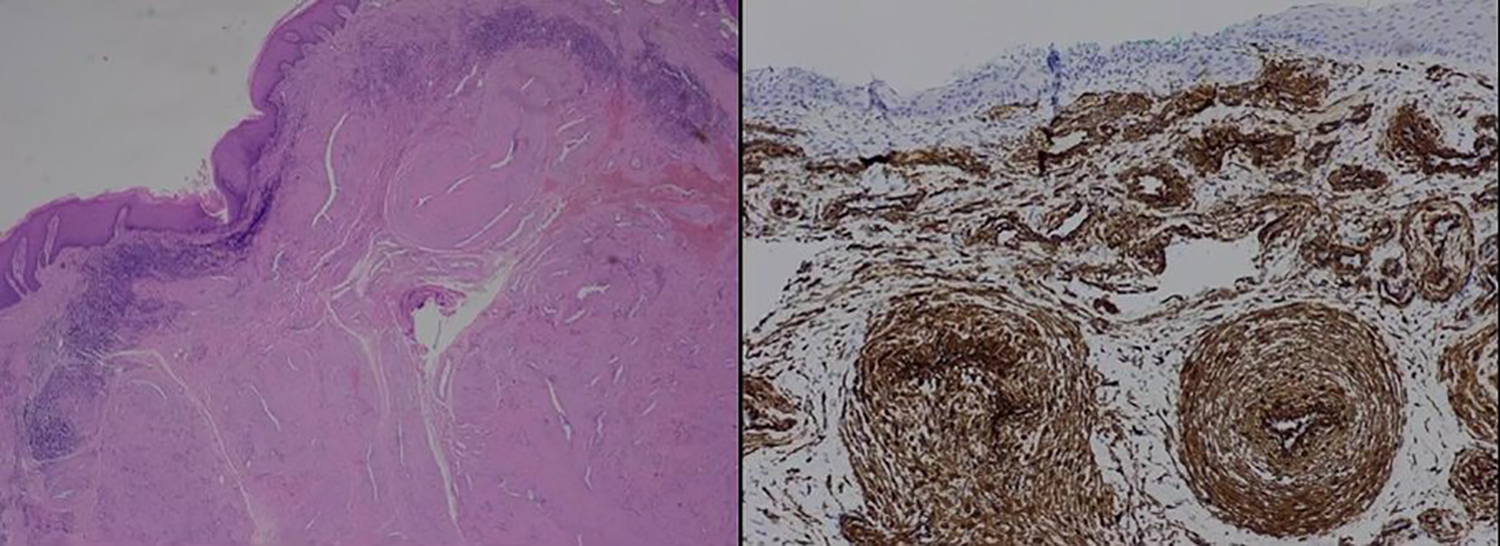
Left side shows hematoxylin and eosin staining (×200) of smooth muscle cell proliferation with thickened blood vessel walls from specimen of patient 1. Right side shows histopathologic image of positive immunostaining for α smooth muscle actin from specimen of patient 2.
The patient’s postoperative recovery period was uncomplicated and no septal perforation, excessive bleeding, or scarring was noted. He has remained disease free for 7 years.
Patient 2
A 52-year-old female presented to the clinic complaining of persistent epistaxis for 3 weeks which required anterior nasal packing multiple times in the emergency department. Her symptoms began after using allergy medications fluticasone and loratadine. Medical history was significant for nasal obstruction and recurrent sinusitis.
Physical examination showed a lesion in the right nasal cavity. Computed tomography (CT) demonstrated a right mid nasal septal mass, left septal deviation, and bilaterally enlarged inferior and middle turbinates (Figure 1).
The patient was scheduled for endoscopic sinus surgery and septoplasty with resection of the nasal mass under general anesthesia. The lesion was found to be an irregularly shaped, sessile mass originating from the right nasal septum and extending to the superior edge of the inferior turbinate. The base of the mass was pink and fleshy. The lateral part of the mass appeared glossy and erythematous. Excision of the tumor with wide margins was performed before proceeding with the septoplasty, bilateral inferior turbinate submucosa resection, bilateral concha bullosa reduction, and right maxillary antrostomy. The specimen was sent for pathologic examination.
On pathology report, the gross specimen measured 0.4 × 0.4 × 0.2 cm. Multiple sections were stained with hematoxylin and eosin (H&E), and periodic acid–Schiff (PAS) staining was negative for fungi. Immunostain for α smooth muscle actin (α-SMA) was positive and confirmed the diagnosis of angioleiomyoma (Figure 2).
The patient’s postoperative course was complicated with only mild nasal bleeding. Monthly follow-ups for 6 months showed no evidence of nasal mass recurrence. The patient has remained disease free for over a year with no signs of septal or sinus complications.
Discussion
Leiomyoma is a benign, smooth muscle tumor which can be classified into 3 histologic groups: leiomyoma, angioleiomyoma, and epithelioid leiomyoma.1,2 They most commonly occur in the uterus (95%), skin (3%), and gastrointestinal tract (1%). 3 Leiomyomas rarely present in the nasal cavity, and this can be attributed to the sparsity of smooth muscle in this location. Both of our patients were diagnosed with angioleiomyoma, leiomyoma originating from blood vessel tunica media, which is the most common histologic variant found in the nasal cavity. 4
On gross examination, angioleiomyomas typically present as tan-pink, fleshy masses with a smooth overlying mucosa. 5 Occasionally, blood vessels may be seen protruding through the mucosa. 6 Imaging with computed tomography (CT) is largely nonspecific and may be most useful as an adjunct technique to appreciate the extent of the tumor growth. 7 Due to the nonspecific appearance and imaging findings, angioleiomyomas are often initially misdiagnosed as more common nasal lesions such as polyps, fibromas, papillomas, hemangiomas, and angiofibromas. Histopathological evaluation provides a definitive diagnosis.
Characteristic histopathologic findings of angioleiomyoma include well-defined fascicles or whorls of mature smooth muscle cells surrounding blood vessel lumina, cigar-shaped nuclei with blunt ends, and absence of nuclear atypia and mitosis.4,5,6 These features suggest a benign lesion while severe atypia, pleomorphism with infiltrative borders, high mitotic count, and tumor cell necrosis would be characteristic of malignancy such as leiomyosarcoma.4,8 Positive staining for α smooth muscle actin, myosin, and desmin aids in confirmation of the diagnosis. Patient 1 was diagnosed with nasal septal angioleiomyoma by histopathological appreciation of the proliferation of blood vessels and smooth muscle. The specimen from patient 2 stained positively for α smooth muscle actin. Neither patient showed a high degree of nuclear atypia or mitosis.
Historically, nasal angioleiomyoma occurs in the fourth to sixth decade of life with a female to male ratio of 2:1. Most common tumor locations in the nasal cavity include the inferior turbinate, septum, and nasal vestibule. Some of the classic presenting symptoms include nasal obstruction (56.25%), epistaxis (56.25%), facial pain (25%), and headache (25%). 9
The preferred treatment for nasal septal angioleiomyoma is surgical excision resulting in clear margins. Complete removal of the mass is critical, because recurrence and malignant transformation have been reported. 3 The approach to excision is largely size dependent and can vary from direct transnasal, endoscopic transnasal, and even craniofacial resection of extensive tumors. In this small series, we report concurrent endoscopic transnasal complete excision of a septal angioleiomyoma and septoplasty with sinus and turbinate surgeries. The largest of these lesions measured 1.0 × 0.8 × 0.6 cm in size. Perforation of the septum, scar tissue and adhesion formation, and persistence and recurrence of disease are feared complications. Both patients reported good outcomes and no complications after their surgeries. From our experience, complete surgical excision of septal angioleiomyoma less than 1.0 cm can be safely performed with a simultaneous septoplasty procedure resulting in limited to no complications. To our knowledge, this is the first series report of concurrent septal angioleiomyoma excision with corrective septal nasal surgery.
Conclusions
Nasal septum angioleiomyoma is rare and seldom considered in the differential diagnosis for nasal cavity masses. Due to the nonspecific clinical findings of nasal septum tumors, definitive diagnosis requires histopathologic evaluation. Completely excising a septal angioleiomyoma and performing simultaneous corrective septal surgery without significant complications is possible. Although neither of our patients reported major postoperative complications, additional studies are needed to determine the largest size of nasal septal angioleiomyoma which can be adequately excised without affecting septal corrective surgery outcomes.
Supplemental Material
Supplemental Material, sj-docx-1-ear-10.1177_0145561321991322 - Nasal Septal Angioleiomyoma and Septal Sinus Surgery: A Review of 2 Cases
Supplemental Material, sj-docx-1-ear-10.1177_0145561321991322 for Nasal Septal Angioleiomyoma and Septal Sinus Surgery: A Review of 2 Cases by Gabriele Noreikaite, Sihun A. Kim and Adelaide Horcher in Ear, Nose & Throat Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.